
Recuperation of severe tumoral calcinosis in a dialysis patient:A case report
2019-04-22 09:01:00LukasWestermannLisaIsbellMarieBreitenfeldtFredericArnoldElviratheleJohannaSchneiderEugenWidmeier
World Journal of Clinical Cases 2019年23期
Lukas Westermann, Lisa K Isbell, Marie K Breitenfeldt, Frederic Arnold, Elvira R?thele, Johanna Schneider,Eugen Widmeier
Lukas Westermann, Frederic Arnold, Elvira R?thele, Johanna Schneider, Eugen Widmeier,Department of Medicine IV, Medical Center, University of Freiburg, Faculty of Medicine,University of Freiburg, Freiburg 79106, Germany
Lisa K Isbell, Department of Medicine I, Medical Center, University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg 79106, Germany
Marie K Breitenfeldt, Dialysis Center Freiburg, Freiburg 79100, Germany
Abstract
Key words: End-stage renal disease; Renal replacement therapy - dialysis;Hyperparathyroidism; Hypercalcemia; Hyperphosphatemia; Tumoral calcinosis; Case report
INTRODUCTION
End-stage renal disease (ESRD) is associated with significant comorbidity and mortality usually representing a condition of abnormal calcium-phosphate metabolism causing hypercalcemia and hyperphosphatemia with associated calcium salt deposits in soft tissues like blood vessels, visceral organs and skin[1-3].While soft tissue calcifications in patients with ESRD is common, the prevalence of extensive periarticular cyst-like calcium salt containing space-consuming lesions in the form of tumoral calcinosis is very rare[4,5].The pathophysiology underlying the development of this rare disease entity remains unclear.It is mostly associated with manifestation of hyperparathyroidism, hypercalcemia and hyperphosphatemia[6].That said, there is evidence of hormone-independent disease onset[7].We describe the case of a 40-yearold woman with ESRD due to IgA-type nephritis on peritoneal dialysis, who developed severe tumoral calcinosis associated with administration of vitamin D analogues, hypercalcemia, hyperphosphatemia and tertiary hyperparathyroidism experiencing complete remission during the next 11 mo after the modification of the treatment strategy.
CASE PRESENTATION
Chief complaints
A 40-year-old woman with ESRD secondary to IgA-nephritis, who had been on continuous ambulatory peritoneal dialysis (CAPD) for 24 mo, was admitted to our emergency department in September 2016 with continuously worsening bilateral immobilizing hip pain since 4 mo.
History of present illness
Her CAPD treatment regime was as follows:Four cycles involving a total dialysate volume of 8000 mL/24 h, three daytime exchanges and one nighttime exchange.The daytime dialysate bags consisted of 1x Dianeal PDG4 1.36%, 2x Dianeal PDG4 2.27%glycose solution containing a calcium concentration of 1.25 mmol/L and 1x overnight extraneal icodextrin solution containing a calcium concentration of 1.75 mmol/L.The CAPD efficacy was measured by peritoneal Kt/V (reference range > 1.7) and was performed on weekly basis.Before the hospital admission, tests had indicated a 24-h urine output of 900 mL, 24-h ultrafiltration rate of 900 mL and a peritoneal Kt/V of 1.32 showing insufficient dialysis quality with clinical signs of uremia.The overall situation was further complicated by the fact that her medical treatment compliance was doubtful, and her peritoneal Kt/V had been successively worsening for the previous 7 mo (for instance, 5 mo before admission, peritoneal Kt/V was indicated at 1.96).For the 4 mo prior to her diagnosis, she had complained of progressive, bilateral pain and immobility of her hips and having progressive, palpable painful indurations around her gluteal and hip regions.She had been taking vitamin D analogues:1, 25-Dihydroxycholecalciferol at a dose of 0.5 μg orally twice a week for 14 mo and cholecalciferol at a dose of 20000 IE orally every 14 d for 20 mo due to low vitamin D3 level associated with increasing parathormone levels.She had been on phosphate binders:calcium acetate with a total daily dose of 1900 mg for 26 mo and sevelamer carbonate with a total daily dose of 3200 mg for 1 mo.
History of past illness
Her past medical history showed preeclampsia associated with HELLP syndrome in September 2005 and usual ESRD comorbidities as follows:Renal anemia, arterial hypertension and hyperparathyroidism as well as a severe CAPD associated peritonitis (S.aureus) in December 2015.
Family history
Family history was positive for chronic kidney disease of unknown etiology in her aunt and cousin.
Physical examination
At admission, her physical examination showed reduced mobility of her hip joints associated with swelling and tenderness on percussion.
Laboratory examinations
Her laboratory findings showed increased serum calcium, phosphate and parathormone levels (Table 1).Her calcitriol level was at the lower reference range at 20 ng/mL 20 d after admission.
Imaging examinations
A computed tomography scan of her pelvic region at admission showed severe bilateral manifestation of tumoral calcinosis, mainly around the trochanter major(Figure 1A, 1B and Figure 2A).
Clinical course
Subsequently, the vitamin D analogue therapy was discontinued.She started lanthan(III)-carbonate, discontinued sevelamer carbonate and started an in-hospital low-calcium and low-phosphate diet.Furthermore, due to the severity of the clinical findings and insufficient quality of CAPD, she was instantly switched to daily hemodialysis (HD).Her HD schedule involved 5-h sessions six times weekly at a 250 mL/min blood pump speed and 500 mL/min dialysate pump speed with the following dialysate composition:Sodium 138 mmol/L, calcium 1.0 mmol/L and bicarbonate 32 mmol/L.The follow-up computed tomography scans, one at 2 mo(Figure 1C, 1D and Figure 2B) and another at 4 mo (Figure 1E, 1F and Figure 2C) after initial diagnosis, demonstrated significant improvement in her tumoral calcinosis.Based on these findings the above-mentioned HD schedule was subsequently reduced to 5-h sessions 3x weekly for the next 3 mo followed by a nighttime HD schedule of 7-h sessions 3x weekly until the present day.
The follow-up computed tomography scan at 11 mo after initial diagnosis revealed complete remission of the tumoral calcinosis (Figure 1G, 1H and Figure 2D) along with normal calcium levels.However, hyperphosphatemia and elevated parathormone levels remained.Due to persistent therapy-refractory tertiary hyperparathyroidism and despite the therapy with etelcalcetid and cinacalcet hydrochloride, the patient underwent a total parathyroidectomy 22 mo after the initial diagnosis and started calcium acetate with a total daily dose of 1900 mg with adequate response to treatment.Follow-up with the patient has, at the time of publication, reached a total of 34 mo with normal range values of calcium, phosphate,Ca x P product, parathormone and calcitriol.The patient is currently listed for kidney transplantation.
FINAL DIAGNOSIS
The final diagnosis of the patient was secondary tumoral calcinosis (calcinosis of chronic renal failure) due to ESRD associated with tertiary hyperparathyroidism,hypercalcemia and hyperphosphatemia.

Table 1 Patient’s calcium, phosphate, parathormone and 25-OH vitamin D2/D3 levels:timeline according to the initial diagnosis of tumoral calcinosis
TREATMENT
Right after the diagnosis of the tumoral calcinosis the patient was switched from PD to daily HD (5-h session 6x/wk for 4 consecutive mo) and subsequently reduced to 5-h sessions 3x weekly for the next 3 mo followed by a nighttime HD schedule of 7-h sessions 3x weekly.The medication was adjusted as follows:Vitamin D analogues and sevelamer carbonate were discontinued; lanthan(III)-carbonate was started upon the diagnosis and continued until parathyroidectomy and then subsequently switched to calcium acetate (continued until time of publication); in addition etelcalcetid was commenced 13 mo after diagnosis but did not have the desired effect and was replaced after 2 mo with cinacalcet hydrochloride, which continued until the parathyroidectomy.
OUTCOME AND FOLLOW-UP
At the time of publication, follow-up with the patient had reached a total of 34 mo.The patient experienced complete remission of tumoral calcinosis 11 mo after the initial diagnosis.The patient underwent a total parathyroidectomy due to persistent therapy-refractory tertiary hyperparathyroidism 22 mo after the initial diagnosis and is currently listed for a kidney transplantation.
DISCUSSION
The tumoral calcinosis (calcinosis of chronic renal failure) represents a benign rare disease entity in ESRD patients and is associated with hypercalcemia,hyperphosphatemia and hyperparathyroidism leading to widespread calcifications of soft tissues mostly in the periarticular regions of the large joints[8].The pathophysiology of tumoral calcinosis remains mostly unclear.ESRD patients often experience dysregulation of calcium phosphate metabolism due to impaired renal phosphate excretion and vitamin D activation causing hyperparathyroidism, elevated calcium phosphate product and the precipitation thereof in soft tissues[6].
In our case, the patient developed tumoral calcinosis due to the insufficient quality of CAPD, doubtful compliance and typical late sequela of calcium phosphate metabolism possibly aggravated by vitamin D3 administration.In addition, a concurrent rapid decrease of PD quality might have been caused by possible calcification of peritoneal microvasculature.Being on CAPD treatment, the patient had a high calcium phosphate product of 6.33 mmol2/L2(normal range:< 4.5 mmol2/L2) and a high parathormone level at admission.The switch of PD to HD led to a rapid and sufficient decrease of calcium phosphate product indicating its sufficient clearance by HD.The most likely explanation is that decreased intradialytic calcium and phosphate levels caused the mobilization of calcium located in soft tissue calcification leading to disaggregation of tumoral calcinosis in a short time with the achievement of a complete remission.However, the tertiary hyperparathyroidism remained present even several months after successful treatment with normal serum calcium levels and was finally treated by a parathyroidectomy.

Figure 1 Computed tomography images of severe tumoral calcinosis with complete remission in an end-stage renal disease patient.
CONCLUSION
We report a patient with ESRD and severe tumoral calcinosis who achieved complete remission.It is important for renal health care providers to recognize that ESRD patients may develop this rare disease entity based on reduced patient compliance and subsequent insufficiency of dialysis regime quality contributing to the aggravation of calcium phosphate disorder in such patients.However, improvement of the treatment strategy and reinforcement of patient compliance can enable the complete remission of this rare disease entity.
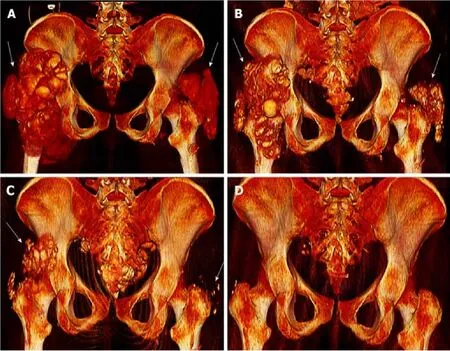
Figure 2 3D reconstruction of computed tomography scan images.
ACKNOWLEDGEMENTS
We are grateful to the patient for her contribution.We thank Patrick Salisbury for proofreading the manuscript.
 World Journal of Clinical Cases2019年23期
World Journal of Clinical Cases2019年23期
- World Journal of Clinical Cases的其它文章
- Pure squamous cell carcinoma of the gallbladder locally invading the liver and abdominal cavity:A case report and review of the literature
- Management of massive fistula bleeding after endoscopic ultrasound-guided pancreatic pseudocyst drainage using hemostatic forceps:A case report
- Fatal complications in a patient with severe multi-space infections in the oral and maxillofacial head and neck regions:A case report
- Bouveret syndrome:A case report
- Left armpit subcutaneous metastasis of gastric cancer:A case report
- Rigid esophagoscopy combined with angle endoscopy for treatment of superior mediastinal foreign bodies penetrating into the esophagus caused by neck trauma:A case report