
Fatal complications in a patient with severe multi-space infections in the oral and maxillofacial head and neck regions:A case report
2019-04-22 09:01:42TianGuoDaiHongBingRanYinXiuQiuBoXuJinQiangChengYingKaiLiu
World Journal of Clinical Cases 2019年23期
Tian-Guo Dai, Hong-Bing Ran, Yin-Xiu Qiu, Bo Xu, Jin-Qiang Cheng, Ying-Kai Liu
Tian-Guo Dai, Hong-Bing Ran, Bo Xu, Jin-Qiang Cheng, Ying-Kai Liu, Department of Oral and Maxillofacial Surgery, Central Hospital of Panzhihua City, Panzhihua 617067, Sichuan Province, China
Yin-Xiu Qiu, Department of Otolaryngology Head and Neck Surgery, Central Hospital of Panzhihua City, Panzhihua 617067, Sichuan Province, China
Abstract
Key words: Odontogenic infection; Multi-space infections; Complication; Oral;Maxillofacial; Head and neck; Case report
INTRODUCTION
Odontogenic infections such as acute periapical periodontitis, alveolar abscess, and pericoronitis of wisdom teeth are common infectious diseases in the oral and maxillofacial regions.Clinically, if these diseases are not treated timely, effectively and correctly in the early stage, the infected tissue may spread up to the skull and brain, down to the thoracic cavity, abdominal cavity and back through the natural potential fascial space in the oral and maxillofacial head and neck regions[1].Severe multi-space infections are formed, which can eventually lead to life-threatening complications (LTCs) such as intracranial infection, pleural effusion, empyema, sepsis and even death[2].When a patient develops LTCs, treatment becomes very complicated, the outcome is poor and the mortality rate is high[3].Nowadays, the occurrence of serious LTCs is less frequent due to rational use of antibiotics and early treatment of odontogenic diseases.Nevertheless, it is still difficult to predict the development of severe odontogenic multi-space infections in the oral and maxillofacial head and neck regions.We report a patient with odontogenic infection who was not effectively treated in the initial stage, and consequently developed severe multi-space infections in the oral, maxillofacial, head and neck, chest and back,mediastinum and posterior abdominal wall regions, and subsequently died of septic shock and acute multiple organ failure.
CASE PRESENTATION
Chief complaints
A 41-year-old man presented with pain in the right lower posterior teeth, followed by swelling and pain in the oral and maxillofacial head and neck regions for 7 d, and difficulty in breathing and swallowing for 2 d.
History of present illness
One week before admission, due to pain in the right lower posterior teeth, the patient placed a cigarette butt dipped in the pesticide "Miehailin" into the "dental cavity" to relieve the pain.However, two days later, there was no significant improvement in dental pain and he visited a local community clinic where the doctors removed the cigarette butt and the patient received an infusion of anti-inflammatory drugs for 4 d.However, the odontogenic infections gradually became aggravated, and spread bilaterally to the floor of the mouth, submandibular space, neck, chest, waist, back,temporal and other areas.The patient also began to have difficulty in breathing,swallowing and eating.Due to these complications, the patient was transferred to our hospital for follow-up treatment as an emergency admission.Since the onset of illness,he had been mentally exhausted, with a poor diet, poor sleep, and weight loss of approximately 2.5 kg.
History of past illness
Healthy, with no specific diseases.
Personal and family history
None.
Physical examination upon admission
Physical examination showed that the patient had an acutely painful face, extensive swelling and pneumatosis in the bilateral temporal, oral, maxillofacial, neck, chest,waist and back regions, combined with skin redness and high temperature.The submandibular space and neck regions pulsated when touched.Puncture revealed purulent fluid which was black, thin, with bubbles and had a foul odor.When the patient was admitted to hospital, mouth opening was less than 1 cm; therefore, the tooth lesion could not be examined properly.
Laboratory examinations
Laboratory examination results on emergency admission were as follows:leukocyte count was 13.53 × 109/L, neutrophil ratio was 88.40%, hypersensitive C-reactive protein was > 180 mg/L, and procalcitonin was 9.8 ng/mL.Electrolyte results were:potassium was 5.65 mmol/L, sodium was 136.4 mmol/L, chlorine was 101.9 mmol/L,calcium was 1.91 mmol/L, and magnesium was 0.93 mmol/L.Liver and kidney function test results were as follows:alanine aminotransferase was 19 U/L, glutamic oxaloacetic aminotransferase was 23 U/L, creatinine was 94 μmol/L, and urea was 19.1 mmol/L.The platelet count was 41.0 × 109/L and the D-dimer level was 1184 ng/mL.The results of blood culture indicated infection withStreptococcus viridans.Drug sensitivity testing indicated that the organism was sensitive to penicillin antibiotics.
Imaging examinations
Computed tomography scans of the maxillofacial, neck and chest regions showed extensive swelling and pneumatosis in soft tissues bilaterally in the oral, maxillofacial,temporal, cervical, parapharyngeal space, chest, back, mediastinum and posterior abdominal wall regions (Figures 1 and 2).The upper respiratory tract was narrowed slightly and bilateral lung pneumothorax was observed.A small amount of effusion was seen bilaterally in the pleura and pericardium (Figure 3A).Lung pneumothorax was more serious on the left side and the compression ratio was approximately 20%-30% (Figure 3B).Pulmonary infection was seen in both lungs, particularly in the left lung.
FINAL DIAGNOSIS
Initial diagnosis on admission was severe multi-space infections bilaterally in the oral and maxillofacial head and neck regions; secondary infections in the thorax, back and waist; mediastinal abscess; bilateral pneumothorax; bilateral pulmonary infection;purulent pleural effusion; pericardial effusion; secondary thrombocytopenia.
TREATMENT
Immediately after admission, the patient was transferred to the intensive care unit(ICU) for specialized intensive care.
Oral and maxillofacial surgeons immediately organized consultations and discussion of treatment plans with doctors from otolaryngology, thoracic surgery,general surgery, hematology, anesthesiology and ICU.
Oral and maxillofacial surgeons were responsible for extensive abscess incision and drainage in the oral and maxillofacial head and neck regions under emergency general anesthesia.Thoracic surgeons were responsible for thoracic and pericardial puncture, catheter drainage and pneumothorax management.General surgeons were responsible for the management of back and waist infections.Otolaryngologists and anesthesiologists were responsible for anesthesia and respiratory management.The hematologist was responsible for platelets and blood transfusion.ICU doctors were responsible for intensive care, antimicrobial administration (Norvancomycin hydrochloride), nutritional support, water, electrolytes and acid-base stability.On the first day after surgery, platelets decreased to 22.00 × 109/L, and liver and kidney function tests were abnormal (alanine aminotransferase 186 U/L, glutamic oxalate aminotransferase 450 U/L, cholinesterase 968 U/L, urea 21.3 mmol/L, creatinine 153μmol/L).Electrolytes were also abnormal (potassium 4.77 mmol/L, sodium 148.8 mmol/L, chlorine 114.6 mmol/L, calcium 1.38 mmol/L).On the second day after surgery, liver and kidney function continued to deteriorate (alanine aminotransferase increased to 168 U/L, glutamic oxalate aminotransferase increased to 1025 U/L,cholinesterase increased to 814 U/L, urea increased to 34.44 mmol/L, creatinine increased to 259 μmol/L).On the third day after surgery, the patient developed septic shock and sudden respiratory and cardiac arrest, and cardiopulmonary resuscitation was implemented immediately.Unfortunately, the rescue efforts were ineffective and the patient died.
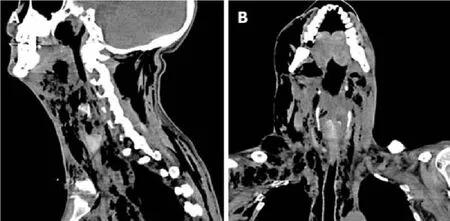
Figure 1 Sagittal and coronal computed tomography scans of the maxillofacial, neck and chest regions.
OUTCOME AND FOLLOW-UP
Despite unremitting efforts by the doctors, the patient eventually died of septic shock and acute hepatic and renal insufficiency.Medical diagnoses at death were as follows:Septic shock; acute hepatic and renal insufficiency; severe multi-space infections bilaterally in the oral and maxillofacial head and neck regions; secondary infections of the thorax, back and waist; mediastinal abscess; bilateral pneumothorax; bilateral pulmonary infection; purulent pleural effusion; pericardial effusion; secondary thrombocytopenia.
DISCUSSION
Approximately 62.6% of oral and maxillofacial head and neck space infections are odontogenic and multiple spaces are involved in 22.5% of cases.The age of these patients ranged from 2 to 84 years and the mortality rate was 1%[4].Huanget al[5]reported that the incidence of LTCs such as multi-space infections in the head and neck regions was about 12.20%, and descending mediastinitis was the most frequent(56.06%), followed by airway obstruction, pneumonia, pericarditis, intraorbital infection, multiple organ failure, intracranial infection and sudden cardiac death.Twelve patients (18.2%) with multi-space infections died during treatment.
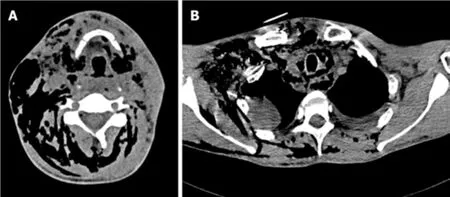
Figure 2 Transverse computed tomography scan of the hyoid plane and mediastinal plane.
In many remote rural areas of China, there is a proverb that toothache is not a disease.Due to this silly proverb, many people do not have a strong sense of oral health care, think that dental pain is not a disease, do not regularly see a dentist , or even use their own "indigenous method" to relieve pain.As reported in this case, the patient put a cigarette butt dipped in the pesticide "Miehailin" into the "dental cavity"to relieve the pain.Miehailin is a highly effective insecticide, which has a good quickkilling effect on mosquitoes, flies, cockroaches, bedbugs, ants and other pests.Why did our patient rapidly progress from having a simple odontogenic disease to multispace infections in the oral, maxillofacial, head and neck regions, which quickly spread to the temporal, chest, mediastinum, back and waist regions? Firstly, we think that the toxicity of pesticides may play a role in the rapid development of diseases.Secondary thrombocytopenia in this patient is the best proof of this proposal.Secondly, in the early stage, the patient visited a non-dental medical institution.The clinician only removed the cigarette butt without any other treatment for the tooth lesion, which resulted in spread of the odontogenic infection.Thirdly, when the patient's odontogenic infection was confined to the oral and maxillofacial region,timely incision and drainage were not performed, which was an important factor in the rapid spread of infection throughout his body.When the patient was rushed to our hospital, oral and maxillofacial surgeons took the lead, and doctors from various departments were urgently consulted to assist in his treatment and formulate a reasonable and appropriate rescue plan.All available rescue measures were adopted,including timely intensive care, anesthesia intubation to ensure that the respiratory tract was unobstructed, extensive systemic abscess incision and drainage under general anesthesia, accurate thoracic and pericardial puncture abscess drainage,administration of the highest level of antibiotics, and platelet transfusion.Unfortunately, the patient died despite unremitting efforts by the doctors.In an analysis of the causes of death, we believe that there were many causes, but the main causes were septic shock, acute multiple organ failure, secondary thrombocytopenia,and pesticide poisoning.
Odontogenic infection can be treated effectively, but can also lead to severe multispace infections in the oral and maxillofacial head and neck regions.The traditional treatment of multi-space infections in these regions is correct anti-bacterial drug administration and abscess incision and drainage[6].In recent years, Qiuet al[7]and Liet al[8]reported that a vacuum sealing drainage-assisted irrigation technique used in the treatment of severe multi-space infections in the oral and maxillofacial cervical regions showed high clinical and therapeutic efficacy.As the infection in our patient was very serious, following discussion and approval by the Drug Administration Committee, we administered the highest level of antibiotics (Norvancomycin hydrochloride) to combat the infection.For extensive incision and drainage of the multi-space infections in the oral and maxillofacial head and neck regions, we adopted disposable multi-functional tube drainage and irrigation technology.This technique can not only irrigate antibacterial drugs into the pus cavity continuously,but also remove infectious wastes by negative pressure suction.
Multi-space infections in the oral and maxillofacial head and neck regions can cause several LTCs.Effective prevention of the occurrence of LTCs is a challenge that oral and maxillofacial surgeons must address.Huanget al[5]reported that older age and underlying systemic disease can increase the risk of multi-space infections.Galloet al[9]reported that algorithm-based management of head and neck space infections was successful in avoiding the onset LTCs.To identify the deep neck infection factors related to LTCs, Mejzliket al[10]conducted a multi-institutional study involving 586 patients.The results showed that patients with neck movement disturbances,dysphonia, dyspnea and swelling of the external neck, accompanied by severe pain,and inflammatory changes in the retropharyngeal space and large vessel areas, with culture-confirmed infection withCandida albicans, are likely to develop LTCs.Osundeet al[11]reported that early recognition and treatment of established cases are necessary to prevent considerable morbidity and mortality.Heimet al[12]showed that simultaneous removal of the infection focus (tooth) and abscess incision reduced the length of hospital stay.Combining literature results and our clinical practice, we believe that patients with serious systemic diseases, extensive infection, extremely abnormal blood and biochemical indicators, and severe respiratory obstruction can be used as predictors of mortality in multi-space infections.
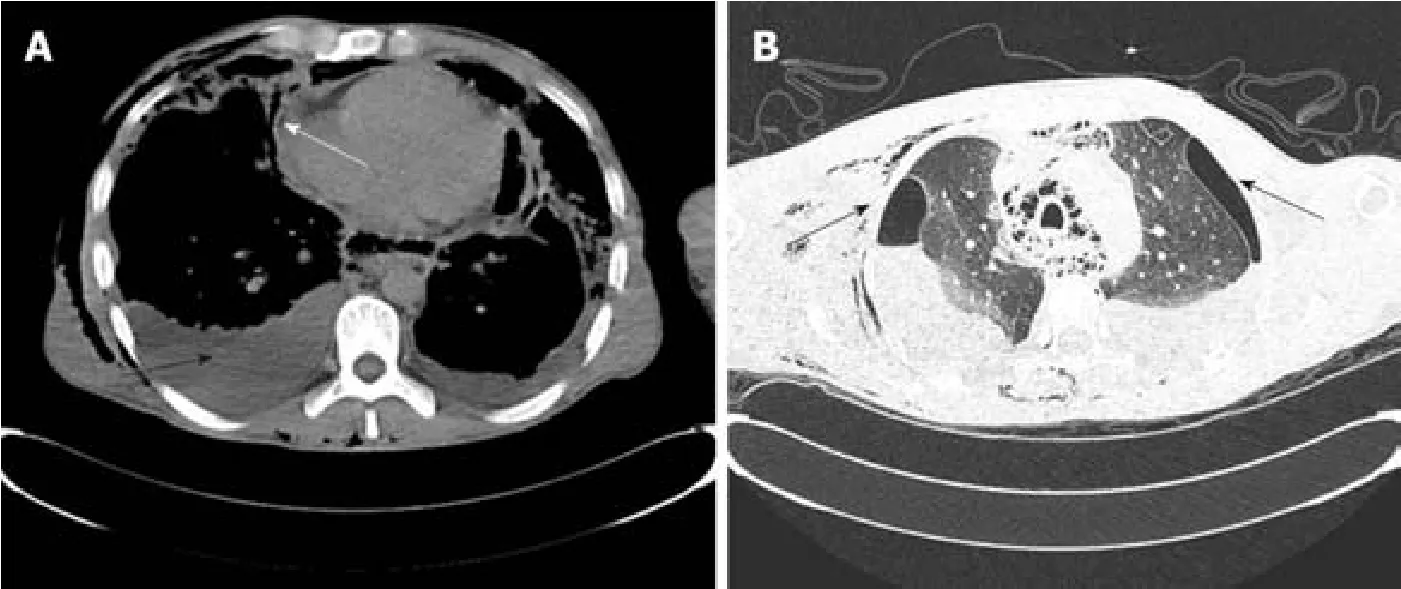
Figure 3 Transverse computed tomography scan of the cardiothoracic region.
CONCLUSION
Odontogenic infection can cause serious multi-space infections in oral and maxillofacial head and neck regions, which can cause several LTCs.As shown in the case reported herein, despite current medical advances, when a patient develops LTCs, the risk of death is high.The prevention of early odontogenic diseases is more meaningful than the treatment of late odontogenic multi-space infections.It is very important to treat the various stages of dental diseases, such as pulp diseases,periapical diseases, and periodontal diseases, effectively and promptly.Furthermore,it is also important to raise awareness of oral health care in remote mountainous areas of China.
 World Journal of Clinical Cases2019年23期
World Journal of Clinical Cases2019年23期
- World Journal of Clinical Cases的其它文章
- Pure squamous cell carcinoma of the gallbladder locally invading the liver and abdominal cavity:A case report and review of the literature
- Management of massive fistula bleeding after endoscopic ultrasound-guided pancreatic pseudocyst drainage using hemostatic forceps:A case report
- Bouveret syndrome:A case report
- Left armpit subcutaneous metastasis of gastric cancer:A case report
- Rigid esophagoscopy combined with angle endoscopy for treatment of superior mediastinal foreign bodies penetrating into the esophagus caused by neck trauma:A case report
- Mixed serous-neuroendocrine neoplasm of the pancreas:A case report and review of the literature