
Pure squamous cell carcinoma of the gallbladder locally invading the liver and abdominal cavity:A case report and review of the literature
2019-04-22 09:01:46ShanJinLuZhangYuanFengWeiHaiJunZhangChengYanWangHongZouJianMingHuJinFangJiangLiJuanPang
World Journal of Clinical Cases 2019年23期
Shan Jin, Lu Zhang, Yuan-Feng Wei, Hai-Jun Zhang, Cheng-Yan Wang, Hong Zou, Jian-Ming Hu,Jin-Fang Jiang, Li-Juan Pang
Shan Jin, Lu Zhang, Yuan-Feng Wei, Hai-Jun Zhang, Cheng-Yan Wang, Hong Zou, Jian-Ming Hu,Jin-Fang Jiang, Li-Juan Pang, Department of Pathology, the First Affiliated Hospital to Shihezi University School of Medicine and Shihezi University School of Medicine, Shihezi 832002,Xinjiang Uygur Autonomous Region, China
Shan Jin, Lu Zhang, Yuan-Feng Wei, Hai-Jun Zhang, Cheng-Yan Wang, Hong Zou, Jian-Ming Hu,Jin-Fang Jiang, Li-Juan Pang, Key Laboratory of Xinjiang Endemic and Ethnic Diseases(Ministry of Education), Shihezi University School of Medicine, Shihezi 832002, Xinjiang Uygur Autonomous Region, China
Abstract
Key words: Gallbladder; Squamous cell carcinoma; Squamous metaplasia;Cholecystectomy; Case report
INTRODUCTION
Gallbladder carcinoma (GBC) is a common type of cancer in the gastrointestinal tract,and adenocarcinoma (AC) is the most common type of gallbladder cancer[1].Squamous cell carcinoma (SCC) is a rare subtype and is responsible for only 2%-3% of gallbladder malignancies[2,3].Due to its rapid development, the majority of patients with gallbladder SCC (GBSCC) initially present with an advanced stage of the disease and hence a poor prognosis[1].Although patients underwent surgical interventions,the 5-year survival rate remained at approximately 1%.The large majority of SCCs are invasive carcinoma entity, often invading the entire gallbladder wall.It had been speculated that adenosquamous carcinomas (ASCs)/SCCs are more aggressive than ordinary gallbladder ACs.It has been testified that the squamous component of GBCs proliferates at a higher rate than the glandular component.However, despite their high proliferation rate, these tumors appeared to less frequently present with lymph node metastasis than gallbladder ACs.Their aggressive biological behavior has been attributed to their potential for direct extension and early invasion into the liver and neighboring organs, such as the stomach, duodenum, and transverse colon.Generally,SCC is aggressive, with infiltration into the liver, and rarely metastasizes to lymph nodes[4].The clinicopathological and biological features of SCC remain to be fully elucidated[5,6], owing to its uncommon occurrence.The majority of currently available data only described individual case reports or series analyses of trivial cases.Therefore, it is imperative to describe the clinicopathological and biological features of SCC[5,6].To improve our understanding of SCC of the gallbladder, we conducted a retrospective case study and review of the literature[6].
CASE PRESENTATION
Chief complaints
A 64-year-old man presented with symptoms of constantly worsening right upper quadrant distension and pain for 1 d.
History of present illness
The patient’s symptoms started a month ago with symptoms of right upper quadrant distension and pain, which had worsened the last 48 h.
History of past illness
The patient did not have a previous medical history.
Personal and family history
The patient denied any personal or family history.
Imaging examinations
Ultrasonography (USG) of the abdomen showed a 5.8 cm × 4.5 cm heterogeneous mass localized in both the gallbladder and liver and a gallbladder with remarkably thickened wall, indicating a malignancy.Computed tomography (CT) and contrastenhanced CT of the liver revealed infiltration of GBC into the adjacent liver, with enlarged retroperitoneal lymph nodes (Figure 1).
The patient underwent radical cholecystectomy for GBC.The gallbladder was intraoperatively observed to adhere tightly to the greater omentum.Moreover,miliary lesions were observed in a portion of the omentum.Neoplastic entities were present at the bottom of the gallbladder, which had invaded the V hepatic segments of the liver.
The gallbladder and a part of the liver tissue were surgically resected (dimension of 13 mm × 5 mm × 8 mm).The gallbladder contained dark green bile.The thickness of the gallbladder wall was approximately 0.2-0.3 cm, and the size of the tumor near the neck of the gallbladder was approximately 5 cm × 4 cm × 6 cm.Part of the mass was grey and soft, and the neoplastic section of the tumor revealed purulent necrosis.The boundaries of the mass and surrounding liver tissue were vague (Figure 2).
Pathological findings
Hematoxylin and eosin staining:For paraffin-embedded tissue specimens,consecutive 3-5 μm thick sections were cut and used for histological analysis[7].Hematoxylin and eosin staining revealed moderately differentiated SCC.The tumor cells invaded the full-thickness of the serosa and approached the surrounding adipose tissue.Part of the tumor also infiltrated the liver tissue.Lymph nodes in the hepatic duodenal ligament were examined, and resected lymph nodes were negative for carcinoma metastasis (Figure 3).
Immunohistochemical staining:Immunohistochemical analysis showed strong staining for AE1/3 and CK5/6 in the tumor.Staining for CK19, CK7, and CAM5.2 was positive in the cytoplasm, and P40 and Ki-67 were positive in the nucleus.In contrast, the expression of hepatocyte marker and AFP was not detected (Figure 4).
FINAL DIAGNOSIS
The final pathological diagnosis was moderately differentiated SCC of the gallbladder.
TREATMENT
Due to the patient’s poor physical condition, systemic chemotherapy was not administered.
OUTCOME AND FOLLOW-UP
After five months, the patient was re-admitted to the hospital owing to fever (Table 1).A space-occupying lesion in the right posterior aspect of the first hepatic portal region was observed by abdominal USG, and considered metastatic cancer (Figure 5).Reexamination of CT and magnetic resonance cholangiopancreatography (MRCP)revealed postoperative changes in the GBC and multiple metastases in the liver and abdominal cavity (Figure 6).
DISCUSSION
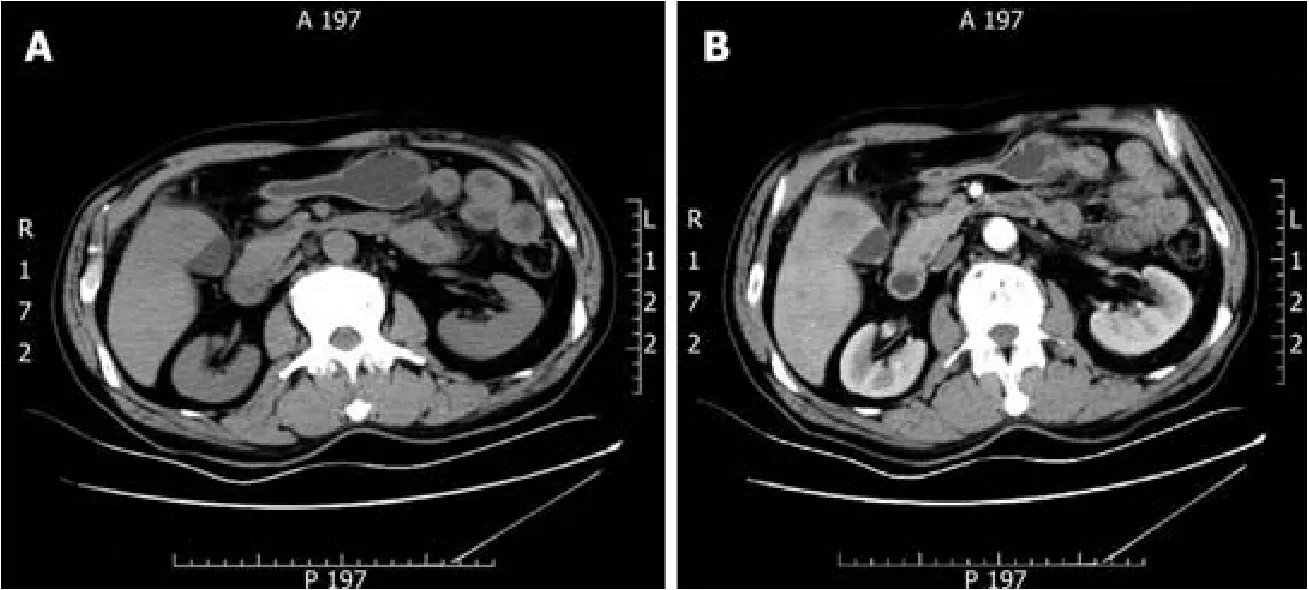
Figure 1 Gallbladder carcinoma infiltrating the adjacent liver, with enlarged retroperitoneal lymph nodes.
GBC is one of the most aggressive malignancies of the gastrointestinal tract[1].GBC includes several subtypes, including AC, SCC, and ASC.Particularly, SCC has a very low incidence rate and represents only 2%-3% of all GBC cases.The progression and overall prognosis of SCC appear to be worse than those of AC and ASC[4,8,9].ASC of the gallbladder is also rare, and its incidence rate is only 7%-10.6%.ASC includes squamous cells and glandular components.The squamous components that may explain the complex biological behavior and poor prognosis show greater capacities of proliferation and local invasion than the glandular components.Lymphatic metastasis and hematogenous metastasis are the principal types of tumor metastasis.
In clinical practice, pain occurs in 66% of patients, and is the most significant symptom.In patients with GBC, the detection of a palpable mass in the right upper quadrant is not specific, but could be a crucial hint that indicates the presence of a malignancy.Some patients may present with a tumor in the right hypochondrial region.However, it could be clinically misdiagnosed as abscess of the gallbladder.USG is the preferred method for diagnosis, and suspected cases can be diagnosed by CT, percutaneous transhepatic cholangiography, MRCP, and fine needle aspiration[4].SCC of the gallbladder has a very poor prognosis, and the involvement of the serosa and lymphatic metastasis are the most important prognostic factors.The size of tumors at diagnosis is the most significant determinant of survival.Therefore, it is especially important to improve the survival index, thus providing useful strategies for early diagnosis and prevention of SCC of the gallbladder[1].
Studies have shown that surgical resection has been considered as the cornerstone of treatment for many years, and complete resection is associated with increased survival[10,11].However, most patients died approximately 6 mo after diagnosis without radical surgery[4].Currently, cholecystectomy, hepatectomy, and lymphadenectomy contribute to patient’s recovery.Some studies demonstrated that the 5-year survival rate may still be low owing to systemic failure.Weatherallet al[11]have confirmed that although patients with SCC of the gallbladder have a larger tumor size and higher possibility of involvement of adjacent organs, complete resection is possible[12].However, there is limited information on the optimal treatment for SCC of the gallbladder.Therefore, physicians have been striving to optimize assisted therapy and improve survival.After surgical resection, the majority of physicians offer adjuvant chemotherapy using 5-fluorouracil.The benefits of the best adjuvant therapy or accompanying chemoradiotherapy remain controversial.
Various hypotheses have been proposed for the etiology of gallbladder SCC,including:(1) Ectopic squamous epithelium with malignant transformation[1]; (2)Metaplastic squamous epithelium with malignant transformation which describes the evolution of metaplasia-dysplasia-carcinoma in progressive development[1,13].The gallbladder may trigger differentiation of glandular cells into squamous cells due to chronic irritation from gallstones.Thereafter, the squamous metaplastic cells may undergo malignant transformation into tumor cells[4,8,13-16]; and (3) Adenocarcinoma with squamous metaplasia.Here, squamous cell elements of mixed ASC of the gallbladder undergo excessive growth and eventually replace all the adenocarcinoma components, resulting in SCC development[4,8,13-16].
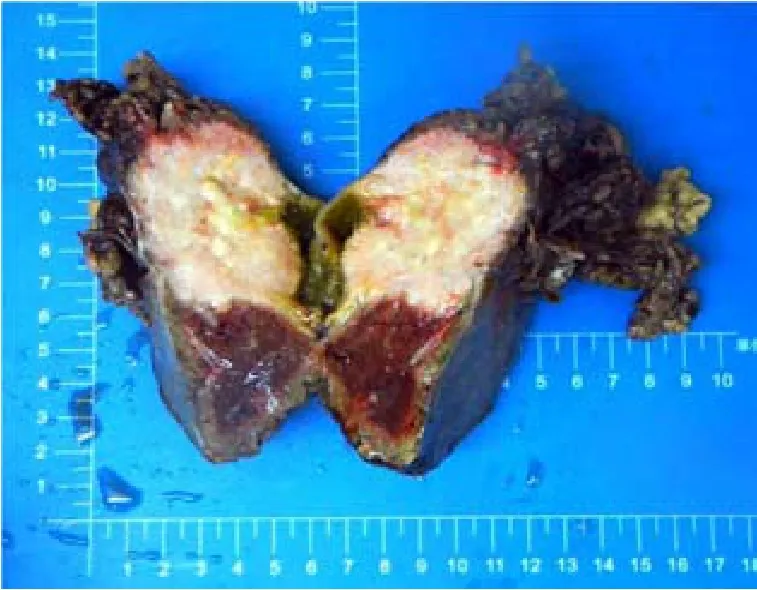
Figure 2 Gross morphology of a 5 cm × 4 cm × 6 cm tumor seen near the gallbladder neck and liver tissue.
The molecular mechanisms for the occurrence and progression of SCC remain unclear.Further studies are needed to determine the etiopathogenetic and molecular differences between this histologic type and conventional adenocarcinomas.Therefore, it is essential to investigate the malignant biological behavior and clinicopathological characteristics of GBSCC.According to studies, CD109 may be associated with the development and clinicopathological characteristics of SCC.CD109 is a glycosylphosphatidylinositol-anchored cell-surface glycoprotein that negatively regulates transforming growth factor-β (TGF-β) signaling as a novel TGF-β co-receptor[17-22].CD109 is a member of the α2-macroglobulin/C3, C4, C5 family of thioester-containing proteins[21,22].CD109 could be a potential biological marker for SCC of the gallbladder[23,24].Furthermore, a higher level expression of the CD109 protein was also reported in SCCs of other organs[24-27].TGF-β is a multipotent cytokine implicated in many physiological processes and regulates a wide variety of cellular processes including cell proliferation, differentiation, adhesion, extracellular matrix deposition, wound healing, and inflammation[18,28-30].TGF-β signal transduction maintains the homeostasis of epithelial cells[24,31], and defective TGF-β signaling may lead to cellular hyper-proliferation, reduced apoptosis, and increased genomic instability[24,32].The transducing factor of the TGF-β signaling pathway is commonly downregulated in human SCCs[23,24].CD109 is a co-receptor of TGF-β1 and increases the binding of TGF-β1 to its receptor[24,33].CD109 is associated with caveolin-1, which can promote the localization of TGF-β receptors in degraded cavities[24,34].Therefore,CD109 regulates TGF-β signaling and enhances TGF-β receptor endocytosis actively.CD109 upregulation in SCC of the gallbladder potentially inhibits TGF-β signal transduction and subsequently promotes SCC progression.In summary, CD109 may be involved in the pathogenesis of gallbladder SCC and serves as a novel target for intervention[24].
Recent findings demonstrate that the clinicopathological features of SC remain to be well recognized.Consequently, the therapeutic interventions remain to be fully elucidated.Although biomarkers for predicting the prognosis of GBSCC have been recognized, they still lack clinical applicability currently.Therefore, it is vital to record the biological and clinicopathological characteristics of GBSCC.
CONCLUSION
Only scarce reports of SCC of the gallbladder have been reported; GBSCC is a rare subtype, and it has a poor prognosis.The squamous components that may explain the complex biological behavior and poor prognosis show greater capacities of proliferation and local invasion in GBC.Surgical resection has been considered as the basis of treatment for years, and complete resection is associated with increased survival.CD109 may be involved in the pathogenesis of gallbladder SCC and serves as a novel target for intervention.
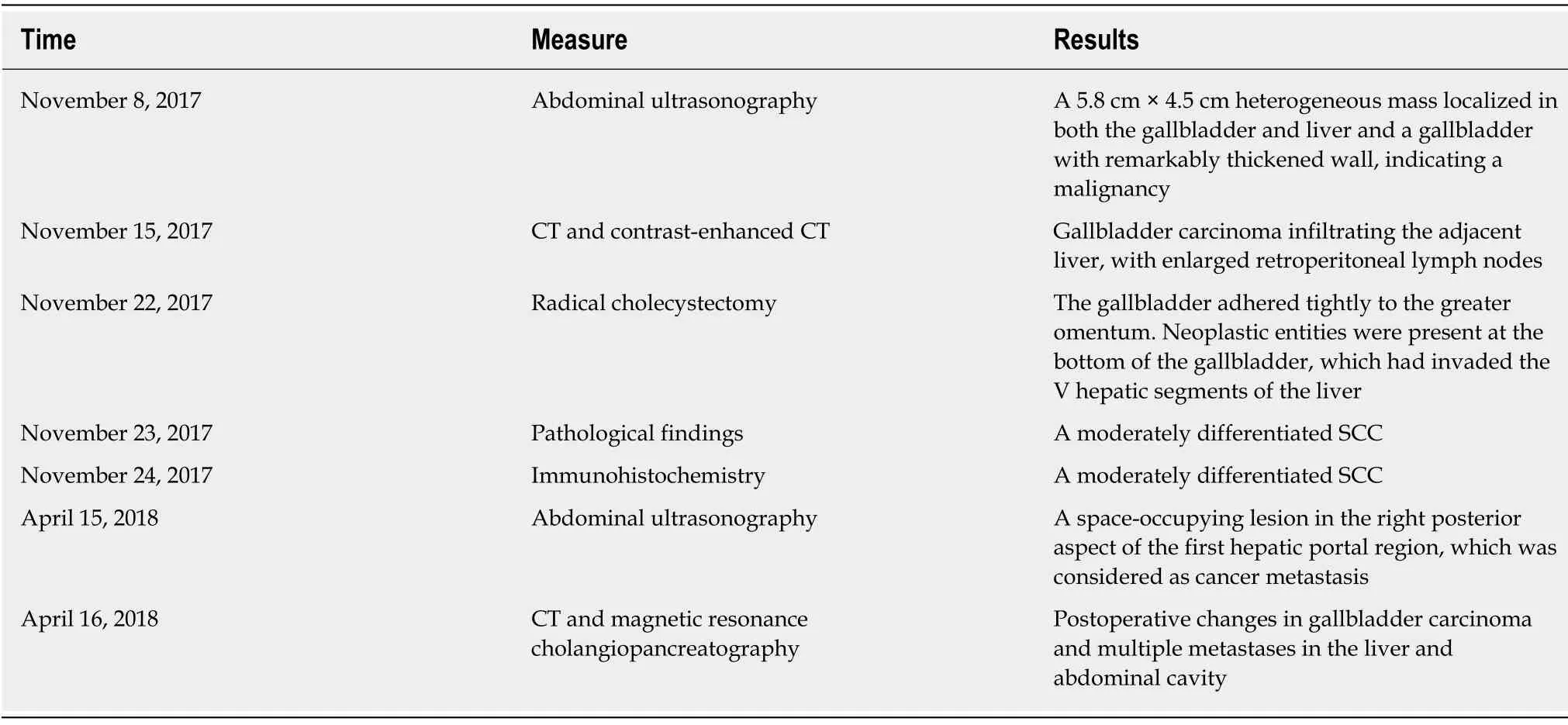
Table 1 Timeline
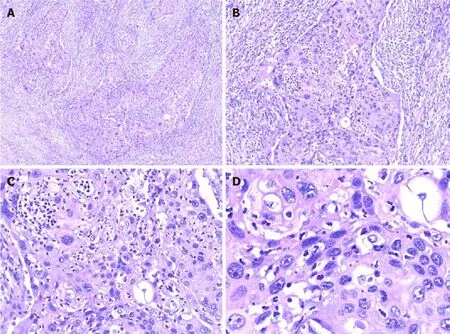
Figure 3 Hematoxylin and eosin staining of tumor cells.
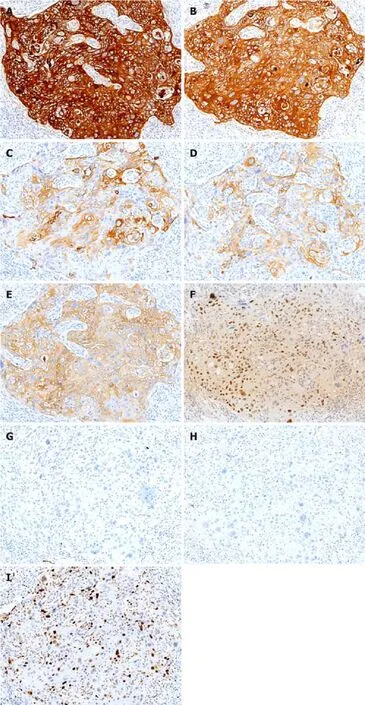
Figure 4 Immunohistochemical staining shows tumor cells in gallbladder squamous cell carcinoma (×100).

Figure 5 Abdominal ultrasonography revealed a space-occupying lesion in the right posterior aspect of the first hepatic portal region, which was considered as cancer metastasis.

Figure 6 Postoperative changes in gallbladder carcinoma and multiple metastases in the liver and abdominal cavity.
 World Journal of Clinical Cases2019年23期
World Journal of Clinical Cases2019年23期
- World Journal of Clinical Cases的其它文章
- Management of massive fistula bleeding after endoscopic ultrasound-guided pancreatic pseudocyst drainage using hemostatic forceps:A case report
- Fatal complications in a patient with severe multi-space infections in the oral and maxillofacial head and neck regions:A case report
- Bouveret syndrome:A case report
- Left armpit subcutaneous metastasis of gastric cancer:A case report
- Rigid esophagoscopy combined with angle endoscopy for treatment of superior mediastinal foreign bodies penetrating into the esophagus caused by neck trauma:A case report
- Mixed serous-neuroendocrine neoplasm of the pancreas:A case report and review of the literature