
Resection of recurrent third branchial cleft fistulas assisted by flexible pharyngotomy
2019-04-22 09:00:50XiaoQiongDingXinZhuLingLiXuFengZhiChunHuang
World Journal of Clinical Cases 2019年23期
Xiao-Qiong Ding, Xin Zhu, Ling Li, Xu Feng, Zhi-Chun Huang
Xiao-Qiong Ding, Xin Zhu, Ling Li, Xu Feng, Zhi-Chun Huang, Department of Otolaryngology Head and Neck Surgery, Zhongda Hospital Southeast University, Nanjing 210000, Jiangsu Province, China
Abstract
Key words: Branchial cleft fistula; Resection; Fiber-optic pharyngoscopy; Pyriform sinus fistula; Guidewire
INTRODUCTION
Branchial cleft anomalies are rare entities that represent about 30% of all congenital neck masses, including branchial cleft cysts, fistulas, and sinuses.Anomalies of the third and fourth branchial clefts make up 3%-10% of all branchial cleft anomalies[1-3].Despite their lesser rate of occurrence, the third and fourth branchial cleft anomalies are important causes of recurrent neck abscesses.Treatment of fistulas arising from the third branchial cleft includes endoscopic cauterization or open cervical fistulectomy[4-8].A number of scholars have recommended complete excision of the anomaly and selective neck dissection for recurrent cases[4,9,10].Others have also advocated simple endoscopic cauterization/ablation of the site of the branchial cleft fistula in the pharynx[11,12].Both approaches are associated with recurrence rates of 14%-18%, and possibly greater rates when the fistula has been treated operatively beforehand[4,12].Recurrences may be multifactorial and related to incomplete resection of all of the anatomical elements of the fistula.Histologically, the internal lining of a branchial cleft fistula consists of a squamous cell epithelial extension from the pyriform sinus, thereby requiring complete excision; ongoing secretions from the submucosal glands in the tract can continue to induce infection or form a cyst.
Here, we attempted to incorporate our clinical experience into a study of 12 adult patients who had recurrent third branchial cleft fistulas treated from January 2013 to December 2017.Our proposed approach involved transoral intubation of the fistulous opening into the pharynx with the aid of flexible fiber-optic pharyngoscopy,combined with fistulectomy with opening of the fibrous portion of the tract.
MATERIALS AND METHODS
The study protocol was approved by the Ethics Committee of the Zhongda Hospital,Southeast University (Nanjing, China), and conducted in accordance with the 1975 Declaration of Helsinki.All patients also signed the written informed consent form.In the present study, 12 adult patients (age, 20-58 years) who were diagnosed with a recurrent third branchial cleft fistula with an internal opening into the pyriform sinus underwent operative treatment.The resected tissues were postoperatively confirmed by pathological examinations.
The patients’ data were providedviaICD-10 codes for branchial cleft fistulas.Input data included patients’ demographic characteristics, clinical presentation,management, surgery, complications, outcome, follow-up, and recurrences.Patients’clinical data are given in Table 1.
Surgical procedure
After a cervical incision excising the external opening, the fistula was sharply dissected circumferentially down to the lateral edge of the thyroid cartilage.The upper lateral third of the thyroid cartilage was resected; during this partial resection of the thyroid cartilage, the superior horn of the thyroid cartilage was disconnected to prevent damage to the superior laryngeal nerve; this procedure markedly facilitated a full exposure of the mucosa of the pyriform sinus.Assisted by transoral pharyngoscopy with a fiber-optic endoscope containing a working port, as well as allowing insufflation of air to better expose the pyriform sinus, the fistulous opening into the pyriform sinus was identified, and a yellow zebra guidewire was inserted into the pyriform sinus.The yellow zebra guidewire was then located in the neck incision, and the opening of the fistula into the pharynx was easily identified as assisted by the guidewire.This opening was fully excised, and the mucosa was sutured in two layers with absorbable suture.In patients with a recurrent branchial cleft fistula, the guidewire would not be able to be passed into the cervical incision due to blocking its retrograde passage.In this case, the scar tissue needed to be resected so that the guidewire could be further passed retrogradely into the cervical wound (Figures 1 and 2).In two patients, the ipsilateral lobe of the thyroid gland was resected if the thyroid tissue was infected or if the thyroid was intimately adherent to the fistula.
RESULTS
We managed 12 adult patients with branchial cleft fistulas.No recurrences of the fistulas were observed during the 13-60 mo follow-up period.All fistulas were fully resected without any complications, such as parapharyngeal abscess, wound infection, injury or dysfunction of the recurrent laryngeal or superior laryngeal nerves, or recurrent pharyngeal fistulas.All of the internal openings of the fistulas in the pharynx were found by oral barium radiography, and easily identified during flexible fiber-optic pharyngoscopy.Laryngeal endoscopy and voice analysis were taken pre-operatively as well as on the 14th d post-operatively.Vocal cord movements did not change.The characters of voice for jitter, shimmer, and normalized noise energy were all within normal limits.Due to pharyngeal and laryngeal edema, the examinations were not carried out during early post-operation.
DISCUSSION
Attempts made at cervical fistulectomy of fistulas related to the third branchial cleft are associated with a high recurrence rate.Similarly, endoscopic cauterization of the sinus tract opening in the pyriform sinus has been conducted by using monopolar electrocautery, chemocauterization using trichloroacetic acid, or application of fibrin glue or silver nitrate.In a large systematic review, recurrence rates have been described as high as 14% for complete excision and 18% for cauterization alone[4].The average percentage of successful endoscopy was only about 75%, as reviewed by a number of scholars[12].Several scholars, however, attempted to implement fistulectomy for the third branchial anomalies, with fistulous openings into the pyriform sinusviaan anterior neck incision, dissection of the sinus tract, as well as ligation at the opening into the pyriform sinus[1,10,13].
We believe that the high recurrence rate of prior attempts at complete resection of a third branchial cleft fistula is related to an incomplete closure of the fistulous opening into the pyriform sinus and/or incomplete resection of the fistula tract.Incomplete closure of the opening into the pyriform sinus by cauterization/ablation permits bacterial flora of the pharynx to enter into the sinus tract.In contrast, fistulectomy without complete excision of the distal-most tract of the fistula and its internal opening into the pharynx may lead to recurrence and recurrent neck abscesses.
A number of scholars recommended that complete resection of both tracts of the fistula and the internal opening should be performed to prevent recurrence[14,15].A previous study reported that selective neck dissection for cases of recurrent branchial cleft fistulas may decrease the recurrence rate[9].In the present study, the proposedprocedure was based on a modified method to resect the entire fistula tract for patients who have failed in a previous surgery.Although the proposed approach is a bit more invasive because it involves resection of the partial lateral thyroid cartilage, it prevents leaving a short segment of the fistula tract near the opening into the pyriform sinus, which may lead to recurrence of the fistula and recurrent cervical abscesses.The proposed approach is highly appropriate for patients who had prior attempts at fistulectomy, in whom segments of the fistula tract persist, typically near the fistulous opening into the pharynx.Using the proposed approach, any remaining tract of the fistula and the communicating internal opening into the pharynx can be found and resected with the aid of a retrograde guidewire placedviaflexible fiberoptic pharyngoscopy.

Table 1 Characteristics of 12 adult patients with recurrent third branchial cleft fistulas
The localization and resection of the opening into the pyriform sinus are of great importance[1].Failure to localize the internal opening into the pharynx has been a common cause of recurrent disease and repeated infection.The use of a colored dye(e.g., methylene blue or external prograde passage of a guidewire from the cervical opening of the fistula) has been reported to facilitate the tracing of the fistula tract and the internal opening into the pharynx at the time of fistulectomy[7].We believe,however, that application of a colored dye can be problematic if the dye gets outside the tract and stains the surrounding tissue, thereby obscuring visualization of the tract.Similarly, when placed prograde into the cervical opening of the fistula, the guidewire does not always reach the internal opening and can perforate the tract of the fistula.Using the proposed approach, resection of the entire superior edge of the thyroid cartilage readily exposes the mucosa of the pyriform sinus.Moreover, flexible fiber-optic pharyngoscopy can be used with a working port aided by insufflation of air to better expose the opening into the pyriform sinus.In addition, retrograde placement of the yellow zebra guidewire into the opening of the fistula is easy and allows the guidewire to be observed in the cervical incision, ensuring the ability to fully excise the internal opening of the fistula using the combined therapy.In all 12 cases, the internal openings and the communicating fistulous tracts were successfully excised using the yellow zebra guidewire.Although direct laryngoscopy can be used to identify and possibly cannulate the opening into the pyriform sinus, it is challenging to place the guidewire into the fistulous tract because the pyriform sinus tends to collapse.In contrast, with the flexible fiber-optic pharyngoscopy, this maneuver accompanied by the visualization of the actual entry point of the fistula is notably easier.Furthermore, the soft head of the yellow zebra guidewire minimizes the possibility of the guidewire, perforating the tract of the fistula.
In conclusion, based on our clinical experience, the fistulas in adults arising from the third branchial cleft with an internal opening into the pyriform sinus can be effectively treated by a combination of transcervical fistulectomy with the removal of the partial thyroid cartilage assisted by flexible fiber-optic pharyngoscopy.This involves insufflation retrograde placement of a soft-tipped guidewireviathe pharyngeal opening, particularly for recurrent fistulas after prior attempts at operative treatment.However, a precise conclusion requires further studies with more cases, control groups, and long-term follow-ups.
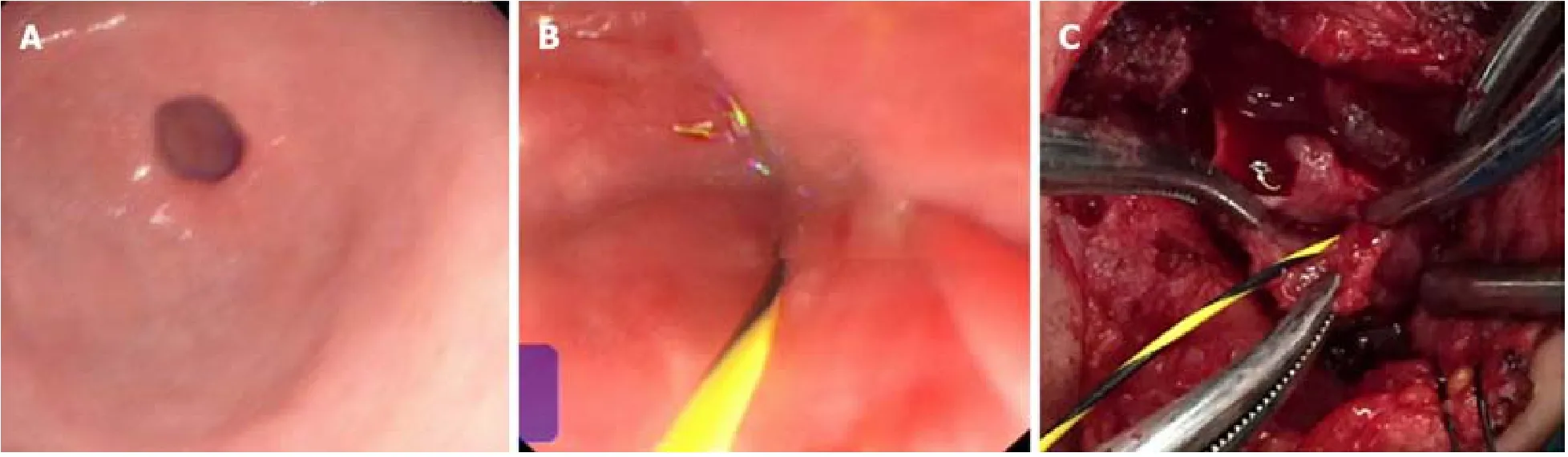
Figure 1 Resection of the third branchial cleft fistula with the help of flexible fiber-optic pharyngoscopy.

Figure 2 Resection of part of the thyroid cartilage and the inner opening was located by flexible fiber-optic pharyngoscopy.
ARTICLE HIGHLIGHTS
Research background
According to the reports, endoscopic cauterization and open cervical fistulectomy are used to treat third branchial cleft fistulas.Both of them are associated with high recurrence rates.Incomplete resection of all anatomic elements of the fistula may be the main cause of recurrence.
Research motivation
A combined therapy was designed to completely resect the fistula.
Research objectives
Here, 12 adult patients who were diagnosed with recurrent third branchial cleft fistulas were included.The patients were treated by endoscopic cauterization or open cervical fistulectomy before, and the fistulas were observed for recurrence at least once.
Research methods
The fistula was traced near the thyroid cartilage, and partial thyroid cartilage was resected to expose the pyriform fossa more clearly.The scar close to the pyriform fossa was eased, and the guidewire was inserted into the pyriform sinus to the fistula by flexible fiber-optic pharyngoscopy, which was then located in the neck incision.All anatomical elements of the fistula could be resected.
Research results
Twelve recurrent third branchial cleft fistulas were completely ablated by the combined method,and no recurrence was found during the 13-60 mo follow-up period.
Research conclusions
In this study, the combined method could expose the hole fistula more clearly and ablate all of the elements of the fistula more easily.Partial resection of the thyroid cartilage could expose the pyriform sinus clearly, and the inner opening could be found from the neck incision.Flexible fiber-optic pharyngoscope could help to locate the inner opening of the pharynx.
Research perspectives
The combined method may be a good way to ablate the third branchial cleft fistulas completely,especially for recurrent fistulas.Also, further studies with more cases, control groups, and longterm follow-ups are needed to make precise conclusions.
 World Journal of Clinical Cases2019年23期
World Journal of Clinical Cases2019年23期
- World Journal of Clinical Cases的其它文章
- Pure squamous cell carcinoma of the gallbladder locally invading the liver and abdominal cavity:A case report and review of the literature
- Management of massive fistula bleeding after endoscopic ultrasound-guided pancreatic pseudocyst drainage using hemostatic forceps:A case report
- Fatal complications in a patient with severe multi-space infections in the oral and maxillofacial head and neck regions:A case report
- Bouveret syndrome:A case report
- Left armpit subcutaneous metastasis of gastric cancer:A case report
- Rigid esophagoscopy combined with angle endoscopy for treatment of superior mediastinal foreign bodies penetrating into the esophagus caused by neck trauma:A case report