
Spontaneous resolution of traumatic cataract after removal of a ferrous intravitreal foreign body using external magnetic extraction through a pars plana incision
2021-05-15 02:51:10ZhiTaoSuZheXuPanPanYeJianMaLiZhangZhiQingChenJiJianLinXiaoYunFangYaoWang
Zhi-Tao Su, Zhe Xu, Pan-Pan Ye, Jian Ma, Li Zhang, Zhi-Qing Chen, Ji-Jian Lin,Xiao-Yun Fang, Yao Wang
Eye Center, Second Affiliated Hospital, School of Medicine,Zhejiang University, Hangzhou 310009, Zhejiang Province,China
Dear Editor,
I am Dr. Zhi-Tao Su, from the Eye Center, Second
Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China. I write to present a case of spontaneous resolution of a traumatic cataract resulted in good visual rehabilitation after removal of a ferrous intravitreal foreign body (IVFB).
Among patients with a posterior segment intraocular foreign body (IOFB) and a traumatic cataract, visual rehabilitation poses a unique challenge to ophthalmic surgeons. There is an increasing trend toward performing pars plana vitrectomy(PPV) and simultaneous cataract extraction in the management of these patients[1]. One study reported spontaneous resolution of a traumatic cataract after removal of an intralenticular foreign body[2], another study also reported lens preservation,which remaining localized opacity, after IOFB removal by PPV[3]. The external approach to the removal of a metallic IOFB remains to be a viable treatment option in select cases[4].Herein, we describe a case of traumatic cataract caused by a small ferrous IVFB, in which good visual rehabilitation was achieved without traumatic cataract surgery after removal of the IVFB through a pars plana incision using an external magnet. All procedures conformed to the Declaration of Helsinki, and written informed consent was obtained from the participant.
A 44-year-old healthy man was referred to our Ophthalmology Department because of decreased visual acuity in his left eye for 2d. The patient had suffered a penetrating trauma to his left eye while hammering metal without safety glasses 2d before.On presentation, the best corrected visual acuity (BCVA)was 20/20 in his right eye and 20/200 in his left eye. The intraocular pressure (IOP) was 16 mm Hg in his right eye and 13 mm Hg in his left eye. A slit lamp examination revealed a 2-mm self-sealing midperipheral corneal penetrating wound at the 5 o’clock position in the patient’s left eye. There was a mild inflammatory response in the anterior chamber. Pupil dilation revealed peripheral anterior and posterior capsular ruptures,with subcapsular opacity involving the visual axis (Figure 1A-1C). A scanning laser ophthalmoscopic image showed a dense shadow in the middle and inferotemporal visual field that was caused by the traumatic cataract (Figure 1D). A small metallic-like foreign body suspended in the vitreous at the 5 o’clock position, without significant vitreous hemorrhage and retinal injury was confirmed by B-scan ultrasonography and orbital computed tomography (Figure 1E, 1F). This IVFB, 1.0 mm in width and 2.5 mm in length, was successfully removed by external magnetic extraction through a pars plana incision at the 5 o’clock position. Postoperatively, the patient received 0.5% levofloxacin eye drops and 1% prednisolone acetate eye drops 4 times a day for 1wk, 1% pranoprofen eye drops 4 times a day for 4wk, and 0.5 g levofloxacin tablet a day for 4d. The patient was followed up 1, 3d, 2wk, 3, 6, and 12mo after the surgery. If necessary, traumatic cataract removal by phacoemulsification and intraocular lens implantation were planned.
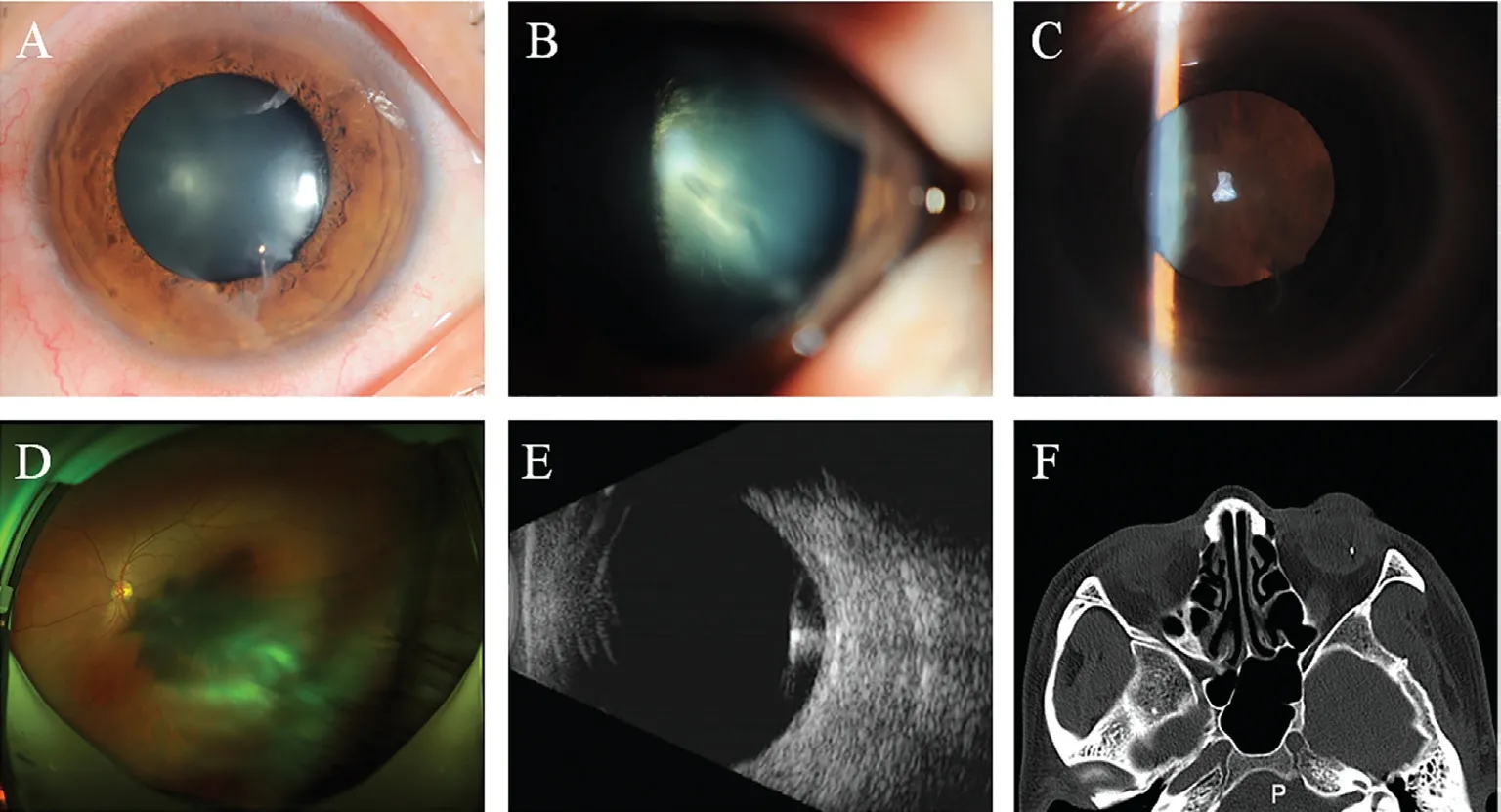
Figure 1 Examination after injury An anterior segment photograph revealed a 2-mm self-sealing midperipheral corneal penetrating wound at the 5 o’clock position, with anterior capsular rupture (A), posterior capsular rupture (B), and significant subcapsular opacity involving the visual axis (C). A scanning laser ophthalmoscopic image showed a dense shadow caused by the traumatic cataract (D). A small metallic-like foreign body suspended in the vitreous without retinal injury was confirmed by B-scan ultrasonography (E) and orbital computed tomography (F).
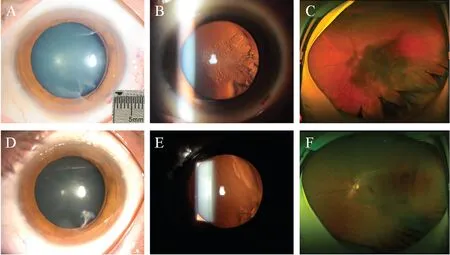
Figure 2 Examination after removal of the IVFB and topical steroids application A 1×2.5 mm2 sized metallic foreign body was successfully removed by external magnetic extraction through a pars plana incision (A). At the follow-up of 2wk after the surgery, the traumatic cataract had partially resolved (A, B), the range and density of the shadow reduced (C). At the follow-up of 3mo after the surgery, the traumatic cataract had mostly resolved, a midperipheral corneal scar (D) and peripheral localized lens opacity (E) were observed. A scanning laser ophthalmoscopic image showed a slight temporal shadow (F).
At the follow-up of 2wk after the surgery, the BCVA had improved to 20/125, the traumatic cataract had partially resolved (Figure 2A, 2B), the range and density of the shadow reduced (Figure 2C), and there were no signs of endophthalmitis or retinal detachment. At the follow-up of 3mo after the surgery, the BCVA was 20/20. A slit lamp examination revealed a midperipheral corneal scar at the 5 o’clock position,with no anterior chamber inflammation. The visual axis was clear under a normal pupil. Pupil dilation revealed peripheral localized lens opacity, without visual axis involvement (Figure 2D, 2E). A scanning laser ophthalmoscopic image showed a slight temporal shadow (Figure 2F). A fundus examination revealed no obvious abnormality.The prognosis of traumatic eye injuries associated with IOFBs varies greatly depending on a number of factors, which include the time between trauma and IOFB extraction, initial visual acuity, entrance wound location, nature of IOFB, location of IOFB, preoperative retinal detachment, presence of intraocular hemorrhage, presence of endophthalmitis, and primary surgical repair combined with IOFB removal and the occurrence of postoperative complications[5]. PPV is the most common surgical approach for the removal of a posterior segment IOFB, as it provides direct viewing and controlled surgery[6].The aim of the treatment is to restore ocular integrity and to obtain a good visual outcome. The time to perform a PPV is depended on several factors, including the presence or absence of clinical endophthalmitis, the associated eye injuries, and the availability of well trained operating room personnel. In case of suspected endophthalmitis, extraction of an IOFB should be performed immediately. Otherwise it can be delayed for a few days until corneal edema resolves and allows a better visualization during vitrectomy, intraocular inflammation is controlled, and suprachoroidal hemorrhage liquefies and thus can be drained if necessary. These processes usually take between 3 and 14d[7-8]. However, in selected patients with small ferrous foreign bodies positioned in the vitreous and no retinal injury, a good visual outcome can be achieved by removal of the IVFB by external magnetic extraction through a pars plana incision[9].
We described the case of a 44-year-old healthy man with a traumatic cataract involving the visual axis caused by a small metallic-like IVFB in his left eye. The IVFB was removed by external magnetic extraction through a pars plana incision.Spontaneous resolution of the traumatic cataract was observed.At the last follow-up 12mo after the removal of the IVFB,BCVA improved to 20/20, stable localized lens opacity, not involving the visual axis, was found, and a fundus examination showed no obvious abnormality.
Lenticular injury as a result of an IOFB may occur if the foreign body passes through the lens. Removal of an IOFB in the presence of a traumatic cataract and associated retinal pathology is difficult. Under such circumstances, cataract extraction is often necessary to enable clear visualization of the posterior segment. Important advances in microsurgical and vitreoretinal instrumentation and techniques (e.g., wide angle viewing systems, high-speed cutters, and improved intraocular instrumentation) have improved the outcomes of these types of ocular injuries.
In cases of clear lens damage and extensive cortical material in the anterior chamber, which may cause increased IOP or a severe inflammatory reaction, lens removal is performed.However, a minor injury to the lens may result in localized nonprogressive lens opacity that does not require surgery. In these cases, epithelial cells may regenerate at the site of the injury and restore capsular continuity, thus limiting the free passage of ions and fluid that can result in progressive cataract formation[10].
In the present case, a small metallic-like IVFB was identified by B-scan ultrasonography and orbital computed tomography,and no signs of endophthalmitis, vitreous hemorrhage, or retinal injury were found. In such cases, removal of the IVFB using an external approach is an easy and a viable treatment option. Removal of the posterior hyaloid, an important surgical goal, was difficult in this relatively young patient. There was also a potential drop of this IVFB on the macula.
In the absence of lens material in the anterior chamber in the presence of a traumatic cataract, some literature states that it is better to treat the eye with topical steroids to control inflammation firstly. In the present case, a slit lamp examination revealed a mild inflammatory reaction in the anterior chamber and no cortical material in the chamber. The patient’s IOP was normal. Small peripheral anterior and posterior capsular ruptures were observed. Although the traumatic cataract interfered with the visual axis, considering the size and location of the capsular ruptures and the mild nature of the inflammatory reaction, in addition to the potential possibility of restoration of capsular continuity and spontaneous resolution of the traumatic cataract, the patient was treated with topical antibiotic and steroids to control the inflammation after the removal of the IVFB, and lens extraction was deferred. During the first 3mo follow-up after removal of the IVFB by external approach, the traumatic cataract was mostly resolved. The visual axis was clear under normal pupil and BCVA improved to 20/20. After pupil dilation, temporal localized lens opacity was found. There were no postoperative complications, such as secondary glaucoma or retinal detachment. At the last followup of 12mo after the surgery, localized lens opacity remained stable and BCVA was 20/20. A fundus examination revealed no obvious abnormality.
To the best of our knowledge, this is the first case of good visual rehabilitation without cataract and vitrectomy surgery in a patient with a penetrating eye injury, accompanied by an IVFB and a traumatic cataract. This case emphasizes the need for clinical education in terms of the management of an IVFB. When determining the need for a surgical intervention or conservative management in such cases, patient-related factors, the size and location of the IOFB, the location and extent of lenticular involvement, and associated injuries should be considered to obtain a good visual outcome.
ACKNOWLEDGEMENTS
Foundations:Supported by the National Natural Science Foundation of China (No.81800877); the Natural Science Foundation of Zhejiang Province (No.LY15H120001;No.LQ17H120008).
Conflicts of Interest: Su ZT,None;Xu Z,None;Ye PP,None;Ma J,None;Zhang L,None;Chen ZQ,None;Lin JJ,None;Fang XY,None;Wang Y,None.
 International Journal of Ophthalmology2021年5期
International Journal of Ophthalmology2021年5期
- International Journal of Ophthalmology的其它文章
- Comprehensive evaluation of intravitreal conbercept versus half-dose photodynamic therapy for chronic central serous chorioretinopathy
- Protective effects of upregulated HO-1 gene against the apoptosis of human retinal pigment epithelial cells in vitro
- An unusual case report of Burkholderia cepacia endophthalmitis
- Glaucoma secondary to trabecular meshwork precipitates: a case report of Grant’s syndrome
- Histological observation in pachyvessels in a patient with choroidal melanoma
- Clinical characteristics and prognostic factors for visual outcome in 669 patients with intraocular foreign bodies