
Glaucoma secondary to trabecular meshwork precipitates: a case report of Grant’s syndrome
2021-05-15 02:51:10YaHuiWeiTianTianRuiLinZhuMeiLi
Ya-Hui Wei, Tian Tian, Rui-Lin Zhu, Mei Li
Department of Ophthalmology, Peking University First Hospital, Beijing 100034, China
Dear Editor,
We write to report a case of glaucoma secondary to trabecular meshwork (TM) precipitates. Secondary glaucoma is a common complication of uveitis, which usually presented as elevated intraocular pressure (IOP)with inflammatory signs, such as ciliary congestion, anterior chamber glare and cells and so on. Grant’s syndrome is a rare cause of secondary glaucoma, with the TM precipitates as the only inflammation sign sometimes[1]. As other inflammatory signs usually were absent or minimal, it is easy to be misdiagnosed as primary open angle glaucoma (POAG).
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for images and other clinical information to be reported in the journal.
A 68-year-old Chinese female patient presented to our hospital, complaining of bilateral blurred vision for four months duration and an occasional ocular halo earlier. She had been diagnosed with POAG elsewhere and was treated with levobunolol, brinzolamide and brimonidine for two months with poor therapeutic efficacy. The patient denied other systemic symptoms or medical history.
On examination, her best corrected visual acuity was 20/20 in each eye. The IOP was 36 mm Hg in the right eye and 33 mm Hg in the left eye, with central corneal thickness of 536 and 540 μm,respectively. Slit-lamp examination of each eye revealed a quiet conjunctiva with clear cornea. No cells or flare were observed in the anterior chamber, nor in the vitreous.Funduscopic examination was normal in both eyes and the cup-to-disc ratios were 0.3. Visual fields and optic disc optical coherence tomography were normal in both eyes. Under gonioscopy, peripheral anterior synechia (PAS) was noted at 4:00-7:00, and in other segments in both eyes, scattered PAS with a few round translucence gelatinous deposits overlying the TM were observed (Figure 1). Ultrasound biomicroscopy of both eyes also revealed multiple discrete nodules overlying the TM (Figure 2).
Systemic evaluations were performed, including serum levels of antinuclear antibody, antineutrophil cytoplasmic antibody,rheumatoid factor, human leukocyte antigen B27, lysozyme,soluble interleukin two receptor, calcium, gamma-globulin,Krebs von den Lungen-6; tests for syphilis, tuberculosis;tests of creatinine, urea nitrogen, aspartate aminotransferase,alanine aminotransferase, and alkaline phosphatase levels;computed tomography images of the chest, abdomen, and pelvis; and all results had unremarkable results. Only a slightly elevated angiotensin converting enzyme (ACE; 60.7 kU/L;reference value: 56.7 kU/L) was observed. Rheumatologic and respiratory consultations were obtained and after a review of manifestations and examinations, no systemic diagnosis was rendered.
The patient was then diagnosed with Grant’s syndrome. After ten days of the treatment with topical prednisolone acetate 1% four times daily, 2% carteolol hydrochloride twice daily,and 0.2% brimonidine three times daily, the IOP in each eye decreased to normal level without any anti-glaucoma treatment, and precipitates on the TM vanished. Usage of topical prednisolone acetate was then tapered. After more than two years without any medical treatment, her IOP has remained within normal limits.
Grant’s syndrome was first described, and named, by Chandler and Grant in 1968[1]. By far, only 16 cases were reported[2-3],and two other cases occurred after argon laser trabeculoplasty[4]as well as intravitreal injection of bevacizumab and ranibizumab[5].All the cases until now were Caucasians or blacks. As far as we know, our case is the first report of Grant’s syndrome in an Asian.

Figure 1 Gonioscopic photograph showing trabecular meshwork precipitates (white arrows) and peripheral anterior synechia (black arrows).
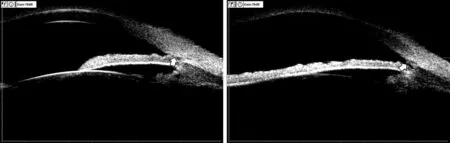
Figure 2 Ultrasound biomicroscopy of precipitates overlying the trabecular meshwork (white arrows).
The primary presentation of Grant’s syndrome is that of elevated IOP accompanied by TM precipitates with or without light anterior chamber flare and cells[1]. The syndrome is diagnosed based on clinical manifestations. In this case, TM precipitates were the only inflammatory presentations without other inflammation signs, which met the characteristics of Grant’s syndrome. We speculated that her sensation of blurred vision might arise from retinal function impairment caused by prolonged elevated IOP, and occasional halos might reveal transient mild corneal edema.
Sarcoidosis, rheumatoid arthritis (RA) and ankylosing spondylitis (AS) have been reported to be associated with Grant’s syndrome. As this patient had elevated ACE,sarcoidosis needs to be considered in differential diagnosis.According to revised diagnosis criteria of ocular sarcoidosis[6],in addition to TM precipitates, other ocular inflammation signs are essential to diagnose probable ocular sarcoidosis.Previous reports of ocular sarcoidosis with TM nodules also had other ocular inflammatory signs[7-10]. This patient only had bilateral TM precipitates, an elevated serum ACE level and other negative tests, which did not support probable ocular sarcoidosis. It is worth noting that the possibility of developing ocular sarcoidosis in the future cannot be ruled out, and we will continue to follow this patient to ascertain if any new abnormalities appear in the future. As she denied joints pain and all other immunology tests were at normal levels, RA and AS were also excluded.
Scleritis, chronic uveitis and Posner-Schlossman syndrome(PSS) have also been reported to accompany Grant’s syndrome[2]. However, these diseases usually had other obvious inflammation signs, such as ciliary congestion,anterior chamber cells, keratic precipitates. These diagnoses were excluded in this case because of the absent inflammatory signs in the eye.
Typical gonioscopic findings in Grant’s syndrome is TM precipitates and scattered irregular PAS[2]. Long-standing TM precipitates can prompt development of PAS. Patients can be misdiagnosed with primary angle-closure glaucoma (PACG),especially those patients with a shallow anterior chamber.In PACG, PAS first appears superiorly and nasally, whereas inflammatory PAS is observed in areas where TM precipitates have been present and tend to distribute in all segments of the chamber angle. In this case, a large area of PAS was observed inferiorly, and additional scattered areas of PAS with overlying precipitates were also noted as well, differentiating this presentation of PAS from that of PACG.
Grant’s syndrome patients have also been reported to be sensitive to glucocorticoids[2]. Our patient was treated with topical corticoids, to which she responded well, as evidenced by a decrease in IOP, and elimination of TM precipitates,further confirming in this case a diagnosis of Grant’s syndrome.
In conclusion, cases presenting only with elevated IOP and TM precipitates could be diagnosed as Grant’s syndrome. The possibility of developing ocular sarcoidosis in the future is not ruled out. It is easy to be misdiagnosed as every finding with the exception of TM precipitates suggested primary glaucoma.
ACKNOWLEDGEMENTS
Conflicts of Interest: Wei YH,None;Tian T,None;Zhu RL,None;Li M,None.
 International Journal of Ophthalmology2021年5期
International Journal of Ophthalmology2021年5期
- International Journal of Ophthalmology的其它文章
- Comprehensive evaluation of intravitreal conbercept versus half-dose photodynamic therapy for chronic central serous chorioretinopathy
- Protective effects of upregulated HO-1 gene against the apoptosis of human retinal pigment epithelial cells in vitro
- An unusual case report of Burkholderia cepacia endophthalmitis
- Spontaneous resolution of traumatic cataract after removal of a ferrous intravitreal foreign body using external magnetic extraction through a pars plana incision
- Histological observation in pachyvessels in a patient with choroidal melanoma
- Clinical characteristics and prognostic factors for visual outcome in 669 patients with intraocular foreign bodies