
Blastic Plasmacytoid Dendritic Cell Neoplasm:A Case Report
2019-08-06 13:05:36JianHuDanDanMaoHouMinLiJianZhongZhangJiangJin
國際皮膚性病學(xué)雜志 2019年2期
Jian Hu, Dan-Dan Mao, Hou-Min Li, Jian-Zhong Zhang, Jiang Jin?
Department of Dermatology, Peking University People’s Hospital, Beijing 100044, China.
Introduction
Blastic plasmacytoid dendritic cell neoplasm(BPDCN)is a rare, aggressive, and deadly hematologic malignancy derived from the precursor of plasmacytoid dendritic cells(pDCs).1BPDCN is a newly described type of tumor that affects hematopoietic and lymphoid tissues; it was categorized by the World Health Organization (WHO)in 2008 as the“acute myeloid leukemia(AML)and related precursor neoplasms” group.2This cancer can occur at any age, but most patients happen to be older adults. It typically involves the skin and rapidly progresses to a leukemia phase.1–3The diagnosis of BPDCN is made on the basis of the observation of a blastic or plasmacytoid morphology, expression of CD4/CD56/CD123 or other markers restricted to pDCs, and lack of expression of lymphoid or myeloid lineage-associated antigens.4Chemotherapies used to treat BPDCN have resulted in frequent relapses and quite poor overall survival rates.Stem cell transplantation may offer a chance for prolonged remission and possible cure, but the rate of relapse with this treatment still remains high.3–5
BPDCN is a rare hematological malignancy,and may be misdiagnosed or missed in diagnosis because of its rareness in dermatological clinics;here we report a case of BPDCN to improve the knowledge of such disease for dermatologists.
Case report
A 62-year-old male presented with a five-month history of violaceous papules on the right temple and a five-month history of multiple infiltrated erythemas on the chest with no itching or pain (Fig. 1A and 1B). The patient had no history of other medical issues except for hypertension.The laboratory examination showed that his peripheral white blood cell count was 9.97×109cells/L. The cell count(1.22×109cells/L)and ratio(12.2%)of monocytes were above normal range, whereas the cell count (0) and ratio (0) of eosinophils were below normal range. Test results for urine occult blood were positive. No enlarged axilla lymph nodes or enlarged retroperitoneal lymph nodes were found by ultrasound or spiral computed tomography tests.A histopathological examination of the lesions revealed a dermal patchy infiltration of lymphoid cells with irregular nuclei of varied sizes. Some of the lymphoid cells displayed bright or pale plasma. We also observed mitoses and extravasation of erythrocytes(Fig. 2A and 2B). Immunohistochemistry analyses produced positive results for CD4, CD56, CD123 (Fig. 3A–3C), and ki67 (30%–40% of tumor cells) and negative results for CD2, CD3, CD5, CD7, CD8, CD10, CD20,GrB, TIA-1, PAX-5, TDT, and Bcl-6. The patient also underwent a bone marrow trephine biopsy.In addition to erythroid cells, granulocytic cells, and megakaryocytic cells, the bone marrow biopsy slice analysis showed lymphoid cells (Fig. 4), which were positive for CD4,CD43, CD56, and ki67 (60%), partly positive for CD3,CD5, CD38, CD68, and TIA-1, and negative for CD10,CD20, PAX5, MPO, and Bcl-6. On the basis of these findings, the patient was diagnosed with BPDCN.
He was administered a chemotherapy of CHOP(cyclophosphamide, doxorubicin, vincristine,and prednisone), and recommended to undergo an allogeneic transplantation. However, the patient refused the allogeneic transplantation, and was lost for follow-up by the time of this writing.
Discussion
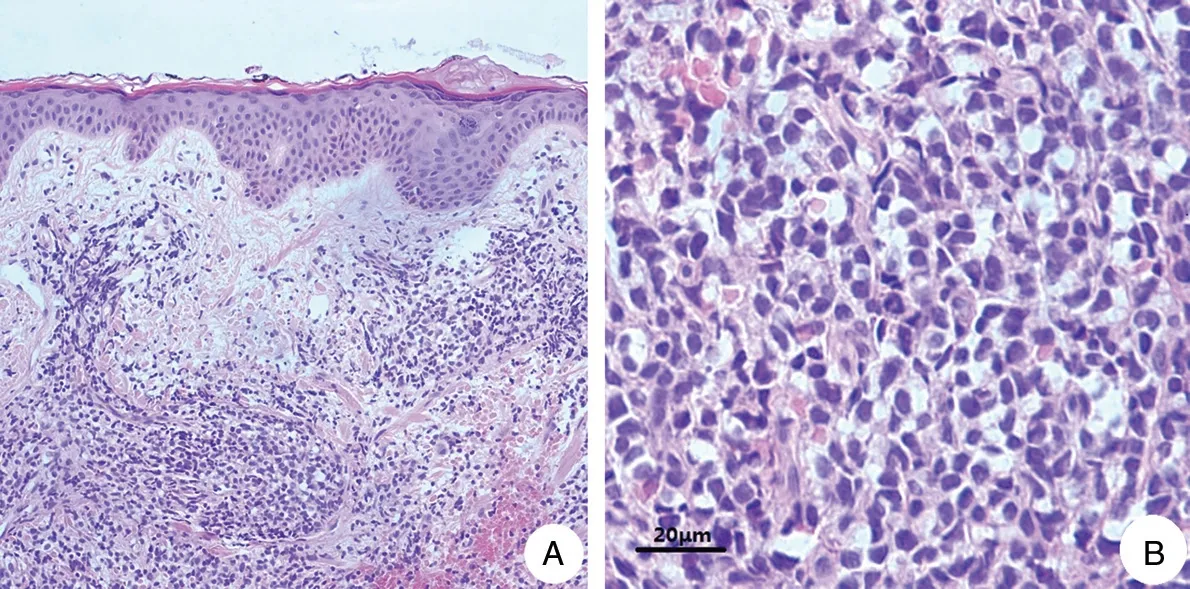
Figure 2. Pathological features of skin biopsy.Representative images of hematoxylin and eosin-stained sections from the patient’s skin biopsy.(A)Focal infiltration of lymphoid cells in the dermis(H&E,×200).(B)Lymphoid cells with irregular nuclei of varied sizes;some display bright or pale plasma. Mitoses and extravasation of erythrocytes are also visible (H&E, ×400).

Figure 3. Representative images of neoplastic lymphoid cells subjected to immunohistochemical staining of CD4(A),CD56(B),and CD123(C)(magnification: ×200).
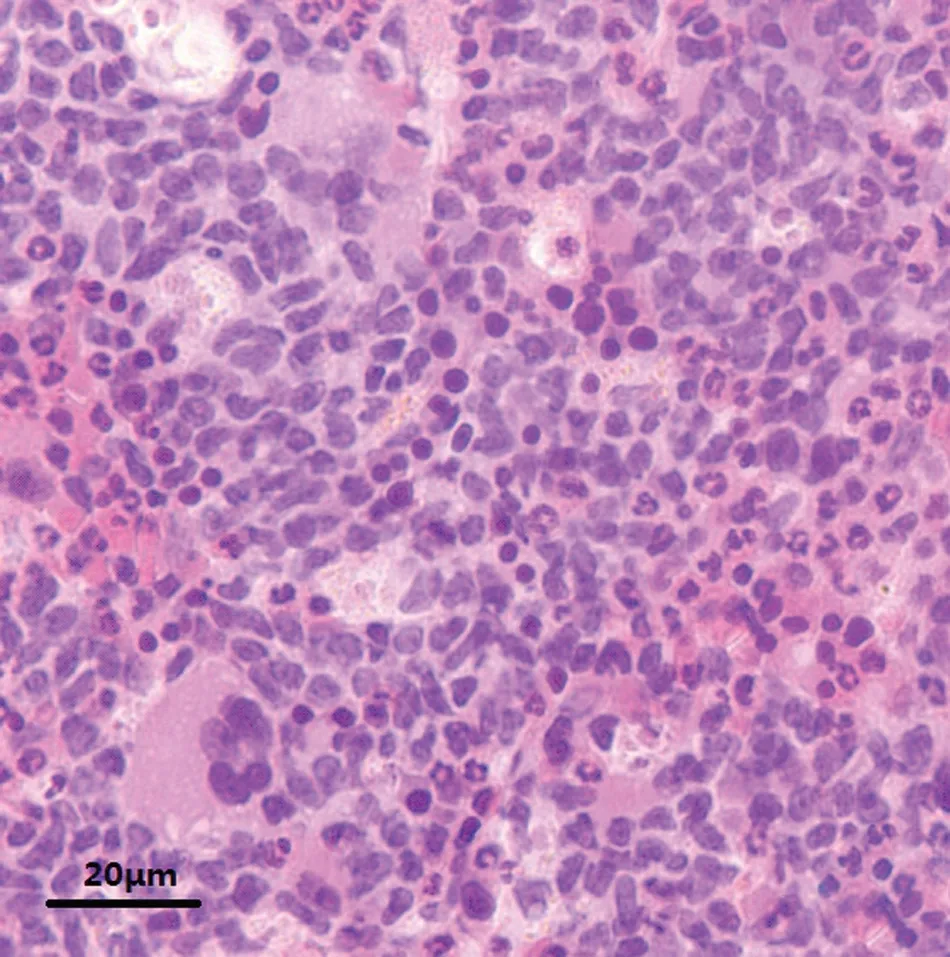
Figure 4. Pathological features of a bone marrow trephine biopsy.Representative image of a hematoxylin and eosin-stained section from the patient’s bone marrow trephine biopsy. Erythroid cells,granulocytic cells,megakaryocytic cells,and medium-sized lymphoid cells are visible (magnification: ×400).
The overall incidence of BPDCN is extremely low; it accounts for only 0.7%of cutaneous lymphomas.6In 85%of BPDCN cases,the initial presentation involves the skin,and the lesions typically present as solitary or multiple papules, plaques, or tumors that are either bruise-like or erythematous.7,8Pathological and immunohistochemistry manifestations are key findings for the diagnosis of BPDCN. Specifically, in BPDCN cases, the tumor cells mainly infiltrate the dermis, but the epidermis is usually not involved, and a grenz zone can be detected. In later phases, the tumor cells frequently extend into the subcutaneous layer but usually spare the adnexal structures.7The tumor cells are medium-sized blast cells,and their nuclei are irregular with evenly dispersed chromatin and more than one nucleoli. Additionally,their cytoplasm is scant without granules and is difficult to distinguish, and mitoses are occasionally observed.3–9BPDCN tumor cells show positive expression of CD4,CD56, and CD123 by immunohistochemistry, and, in some cases, can show weakly positive expression of CD4 and CD56.Blood dendritic cell antigens(BDCA)2 and 4,CD2AP, CD45RA, TCL1, and CLA markers are also coexpressed in these tumor cells.In contrast,T-cell markers,B-cell markers, lysozyme, and myeloperoxidase are typically not expressed.3Thus, based on the expression patterns of these markers, BPDCN can be differentiated from cutaneous T-cell lymphoma, NK-cell malignancies expressing a CD4 or CD56 immunophenotype, myeloid and dendritic cell neoplasms, and reactive hyperplasia of pDCs not exhibiting CD56.
Effective therapy has not been established for BPDCN.Regimens derived from the management of more common hematological malignancies have been used as initial therapy,and stem cell transplantation has been utilized as a consolidative therapy; however, the outcomes are generally poor. Specific targeted agents may offer a prospective future therapy for BPDCN.3–5
- 國際皮膚性病學(xué)雜志的其它文章
- Spitz Nevus with Specific Dermoscopic Features
- Subcutaneous Panniculitis-Like T-Cell Lymphoma: A Case Report
- Cutaneous Rosai–Dorfman Disease Presenting with Multiple Nodules on the Thighs and Buttocks
- Oculocutaneous Albinism with Squamous Cell Carcinoma, Bowen’s Disease and Actinic Keratosis: A Case Report
- Successful Treatment of Synovitis, Acne,Pustulosis, Hyperostosis and Osteitis Syndrome with Thalidomide: A Case Report
- Characteristics of Cutaneous and Subcutaneous Infectious Granuloma at a Signal Center in China:A Five-Year Retrospective Study