
Oculocutaneous Albinism with Squamous Cell Carcinoma, Bowen’s Disease and Actinic Keratosis: A Case Report
2019-08-06 13:05:34QiZhangJinFaDouHuiQianYu
國際皮膚性病學雜志 2019年2期
Qi Zhang, Jin-Fa Dou, Hui-Qian Yu,?
1Postgraduate Training Base in Henan Provincial People’s Hospital of Jinzhou Medical University, Zhengzhou, Henan 450003,China, 2Department of Dermatology, Henan Provincial People’s Hospital, Zhengzhou, Henan 450003, China.
Introduction
Oculocutaneous albinism(OCA)is an autosomal recessive disorder characterized by defects in melanin synthesis that affect the skin, eyes, ears, and hair to varying degrees.Because of the melanin deficiency, albino patients are at high risk for sun-induced skin cancers.Herein,we report a rare case of an OCA type 4 combined with a progressive carcinogenesis for precancerous(actinic keratosis,AK),in situ(Bowen’s disease),and invasive status of squamous cell carcinoma (SCC).
Case report
A 60-year-old Chinese man with an 11-year history of multiple skin plagues was referred to Department of Dermatology, Henan Provincial People’s Hospital. We learned by tracing the medical history that the patient initially observed scattered erythema on the extensible sides of his upper limbs after sun exposure.Over a period of years, the skin lesions slowly increased in size and number,and involved the face,auricle,chest,and back.He had had white hair, white skin, photosensitivity, and photophobia since childhood.However,no family history of albinism was recorded. Furthermore, the patient’s parents denied having a relative marriage.
Physical examination revealed a fair-skinned man with marked nystagmus and decreased visual acuity. His hair was originally white, while the images showed a temporary hair colorant. His irises were pale brown,and the papillaries appeared pink. He had multiple keratotic papular and plaque lesions of 2mm to 4cm,which were round to oval, and surrounded by erythematous zones. Moreover, a porcelain-white maculae atrophicae was observed on the dorsum of the nose,accompanied by facial telangiectasia (Fig. 1A and 1B).No obvious abnormalities were found in laboratory tests.
Clinical and laboratory results suggested some types of OCA. We performed mutation analysis for candidate genes of OCA.The results showed homozygous mutations of c.478G>C,p.D160H in the SLC45A2 gene,and these findings led to the final diagnosis of OCA4 (Fig. 1C).
A keratotic plaque measuring 2cm ×1cm was observed on the right auricle, and was pathologically diagnosed as SCC (Fig. 2A and 2B). Scaly keratotic erythema was observed on the forearms, and it was pathologically diagnosed as AK (Fig. 2C and 2D). Furthermore, a partially keratotic erythema measuring 3cm × 2cm occurred on his right side of back that was diagnosed as Bowen’s disease (Fig. 2E and 2F).
A diagnosis of OCA4 with SCC, Bowen’s disease, and AK was made. We recommended reduction of UV radiation exposure and wearing UV-protective clothing and sunglasses. He was treated with oral etretinate,tretinoin cream, urea ointment, and cryotherapy with liquid nitrogen in some large lesions. The patient was followed up for one year: the erythematous zones on the back mostly vanished gradually, and the plaques on the bilateral forearm were thinner and partially vanished.No new lesions were observed and no obvious abnormality was found in laboratory examinations.
Discussion
OCA is an autosomal recessive disorder of melanocyte differentiation caused by defects in the pathway of melanin biosynthesis,secondary to defects in melanosome biogenesis or function, or by dysregulation of intracellular transport and localization of proteins essential for melanin production.1Classic OCA is divided into eight types,namely, OCA1A, OCA1B, and OCA2–OCA7. This phenotype series is caused by homozygous or compound heterozygous pathogenic variants in TYR,OCA2,TYRP1,SLC45A2, SLC24A5, and C10 or f11.2-3
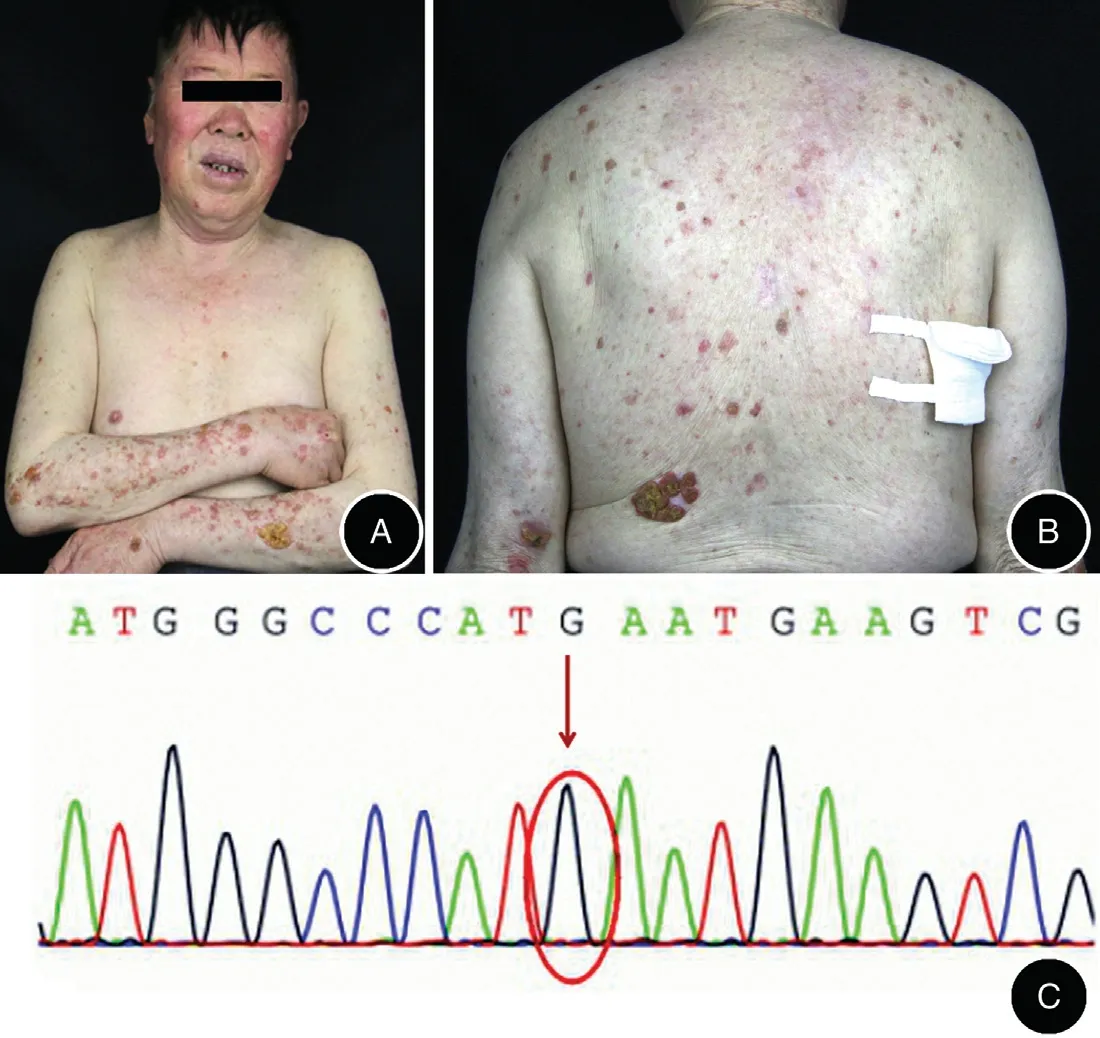
Figure 1. Clinical presentation of the patient with gene sequencing result.(A and B)Multiple keratotic papular and plaque lesions of 2mm to 4 cm in size,which involved the face,auricle,chest,extensible sides of the upper limbs and back.(C)Homozygous mutations of c.478G>C,p.D160H in the SLC45A2 gene. The arrow indicates the position of the mutation.
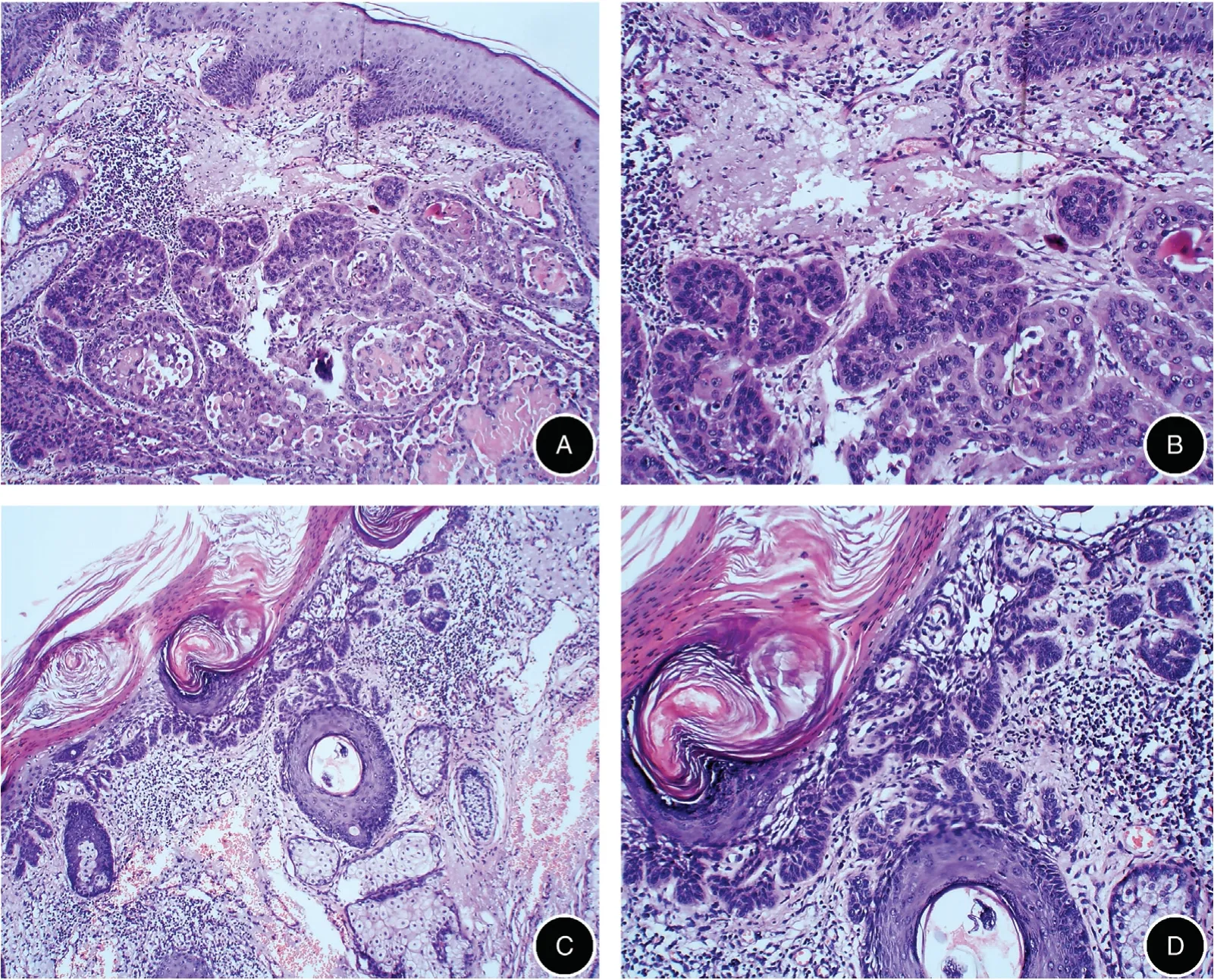
Figure 2. Histopathological results of biopsy specimens.(A and B)H&E staining of a keratotic plaque on the right side of auricle showed a large amount of squamous cell mass grew invasively into the dermis,the cells had obvious atypia.Note the keratin pearl and mitotic count(A:×100,B:×200).(C and D)H&E staining of scaly keratotic erythemas on the forearms showed hyperkeratosis and parakeratosis.Some basal cells showed bud-type hyperplasia inside the dermis.Note the presence in the superficial layer of the dermis of solar elastosis and inflammatory cells infiltrate(C:×100,D:×200).(E and F)H&E staining of a partially keratotic erythema on the right side of back showed hyperkeratosis,acanthosis cell layer thickening, with the disorganized epidermal cells. Note more heterocyst and mitotic count (E: ×100, F: ×200).
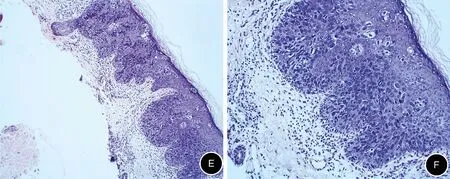
Figure 2. (Continued).
The clinical features of different OCA subtypes are similar; consequently, making a differential diagnosis for OCA subtyping is challenging. Qiu et al.4showed that OCA1 is the most common subtype in the cohort of Chinese population followed by OCA2, OCA4, and OCA3. Our patient was diagnosed with OCA4, and his mutation was c.478G>C,p.D160H in the SLC45A2 gene,which was first discovered in a Chinese case of OCA type 4 in 2008.5
Because of their melanin deficiency, albino patients are highly sensitive to actinic damage(UV light exposure).Skin pigmentation degree is inversely correlated with the risk of sun-induced skin cancers.6The cutaneous problems that occur in OCA patients are sunburns,basal cell carcinoma,malignant melanoma,dysplastic nevus syndrome,7and,the most important and most common of all, AKs that are predisposed to SCC.AKs are a clinical manifestation of UV radiation (most commonly UV-B radiation)-induced neoplastic transformation of keratinocytes. Moreover, UV-B radiation causes thymidine dimer formation in DNA and RNA,thereby resulting in mutations that lead to neoplastic changes in keratinocytes.7
Treatment of AKs and skin cancers, including surgery,radiotherapy, cryotherapy with liquid nitrogen, photodynamic, retinoic acid, and other drugs, is important.Nevertheless, skin cancer prevention is an even more important long-term goal.This goal can be accomplished only by avoiding sun exposure and/or by using sun protection methods.Regular examination of all albinos for early detection and treatment of various malignant lesions is important. Furthermore, genetic counseling could be adopted. Physicians should maintain a high index of suspicion in this vulnerable population.
- 國際皮膚性病學雜志的其它文章
- Blastic Plasmacytoid Dendritic Cell Neoplasm:A Case Report
- Spitz Nevus with Specific Dermoscopic Features
- Subcutaneous Panniculitis-Like T-Cell Lymphoma: A Case Report
- Cutaneous Rosai–Dorfman Disease Presenting with Multiple Nodules on the Thighs and Buttocks
- Successful Treatment of Synovitis, Acne,Pustulosis, Hyperostosis and Osteitis Syndrome with Thalidomide: A Case Report
- Characteristics of Cutaneous and Subcutaneous Infectious Granuloma at a Signal Center in China:A Five-Year Retrospective Study