
Spitz Nevus with Specific Dermoscopic Features
2019-08-06 13:05:36ZhaoRuiLiuandJieLiu
國際皮膚性病學(xué)雜志 2019年2期
Zhao-Rui Liu and Jie Liu?
Department of Dermatology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, China.
Introduction
Spitz nevus is recognized as a benign or indolent melanocyte proliferation that most commonly develops in children and young adults.In some cases,atypical Spitz nevus may mimic a malignant melanocytic neoplasm. To differentiate Spitz nevus from melanoma, thorough examinations are needed. Dermoscopy has emerged as an important tool in the evaluation of patients with lesions suspected as Spitz nevi,but there have not been many cases reported in China that used dermoscopic analysis. Here,we report a case of a five-year-old boy with a Spitz nevus on his face, describing its clinical manifestations, histopathological characteristics,and,most notably,its specific patterns of dermoscopy.
Case report
On September 7, 2017, a five-year-old Chinese boy presented with a red nodule on his left cheek. Two years ago,the lesion had started as a 2mm flat brown nevus.Six months ago,the lesion had increased rapidly in extension and become a nodule of 8mm×6mm. The boy was otherwise healthy,with no history of trauma,sunburn,or exposure to radiation.His medical history was unremarkable, and no such lesions had been found in other family members.
Physical examination revealed a reddish-brown domeshaped nodule of 8mm×6mm with a sharply demarcated,symmetrical border on his left cheek (Fig. 1A).
Dermoscopic examination demonstrated a globular pattern and starburst pattern. Additionally, a homogeneous pink color, chrysalis structures, and reticular depigmentation were also observed (Fig. 1B).
Histopathology revealed hyperkeratosis and focal parakeratosis,confluent nests with peripheral clefts composed of spindle cells, and epithelioid cells at the dermalepidermal junction. There were clusters of spindle cells,lymphocyte infiltration, and melanocytes in the papillary dermis. Kamino bodies were absent (Fig. 1C). Immunohistochemical staining revealed that the majority of epithelioid cells were S100-positive and melan-A-positive(Fig. 2A and 2B), while a subset of epithelioid cells were HMB-45-positive in a stratified staining pattern at the dermal-epidermal junction, with few positive cells in the deep dermis (Fig. 2C). Based on all the above findings, a diagnosis of Spitz nevus was confirmed.
The boy was in regular clinical and dermoscopic observation after the complete excision of the lesion for histopathology. A follow-up study six months later showed a clear excised margin, and no recurrence was detected.
Discussion
Spitz nevi, which display benign clinical behaviors, were first identified in 1948 by Sophie Spitz, who referred to them as “melanomas of childhood.”1Most Spitz nevi present as solitary, well-circumscribed, hairless, firm,symmetrical, and dome-shaped papules/nodules on the face or lower extremities,although the occurrence of Spitz nevi on arca has also been reported.2The color tends to vary from nonpigmented to red/pink to brown pigmentation, depending on the melanin content and distribution,and the surface may be smooth or verrucous. The lesions are usually less than 2cm in diameter, typically occur in young patients, and tend to have a rapid growth phase followed by a static phase. Common misdiagnoses for Spitz nevi lesions include wart, pyogenic granuloma,dermatofibroma, or juvenile xanthogranuloma.

Figure 1. Clinical manifestations, dermoscopy, and histopathology of the patient. (A) Physical examination showed a reddish-brown domeshaped nodule of 8mm×6mm on the boy’s left cheek. (B) Dermoscopic examination demonstrated a globular pattern, starburst pattern,homogeneous pink color, chrysalis structures, and reticular depigmentation. (C) Histopathology revealed hyperkeratosis and focal parakeratosis, confluent nests with peripheral clefts composed of spindle cells and epithelioid cells, clusters of spindle cells, lymphocyte infiltration, and melanocytes in the papillary dermis.
The dermoscopic findings of Spitz nevi depend on the type, that is, whether they are pigmented or not. In nonpigmented Spitz nevi,five patterns have been identified:(1)homogeneous pink color, (2) dotted vascular pattern, (3)starburst vascular pattern, (4) reticular depigmentation,and(5)chrysalis structures.3Pigmented Spitz nevi typically exhibit four patterns: (1) starburst pattern, (2) globular pattern, (3) multicomponent, and (4) homogeneous.4“Starburst pattern”refers to central blue-black pigmentation with regular radial projections at the periphery,whereas globular patterns are described as having central blue-black pigmentation and large, brown-black, regular globules regularly distributed at the periphery. However,atypical Spitz nevi demonstrate multicomponent and nonspecific patterns on dermoscopy, and cases with atypical patterns may be indistinguishable from melanoma.In a recent review of the dermoscopic features of 896 Spitz nevi, the starburst pattern was the most frequently observed dermoscopic pattern (50.6%), followed by the pattern of dotted vessels(19.3%),and the globular pattern(17%). A multicomponent/atypical pattern characterized 9.0% of the Spitz nevi.5Dermoscopic pattern changes were also observed in different stages of Spitz nevi.Emiroglu et al.6reported that the transformation from globular and starburst patterns to a homogeneous pattern was the most frequent pattern change. Dermoscopy revealed a sequential evolution from a globular pattern to a starburst pattern and then to a homogeneous pattern,or from a globular pattern directly to a homogeneous pattern in most lesions.
The present case showed concurrent pigmented and nonpigmented features under dermoscopy, which has rarely been described in reported cases. The observed pigmented features include a globular pattern and starburst pattern,and the observed nonpigmented features include a homogeneous pink color, chrysalis structures,and reticular depigmentation. Dermoscopy improves the clinical recognition of Spitz nevi, but a morphological overlap between Spitz nevi and spitzoid melanoma does exist.To reach a consensus,the International Dermoscopy Society management guidelines of Spitz nevi mainly depend on dermoscopic patterns.5According to these guidelines, dermoscopically asymmetric lesions with spitzoid features (both flat/raised and nodular) should be excised to rule out melanoma. Dermoscopically symmetric spitzoid nodules should also be excised or closely monitored,irrespective of age,to rule out atypical Spitz tumors. Dermoscopically symmetric, flat spitzoid lesions should be managed according to the age of the patient.Finally,the histopathological diagnosis of atypical Spitz tumor should warrant wide excision but not a sentinel lymph node biopsy.
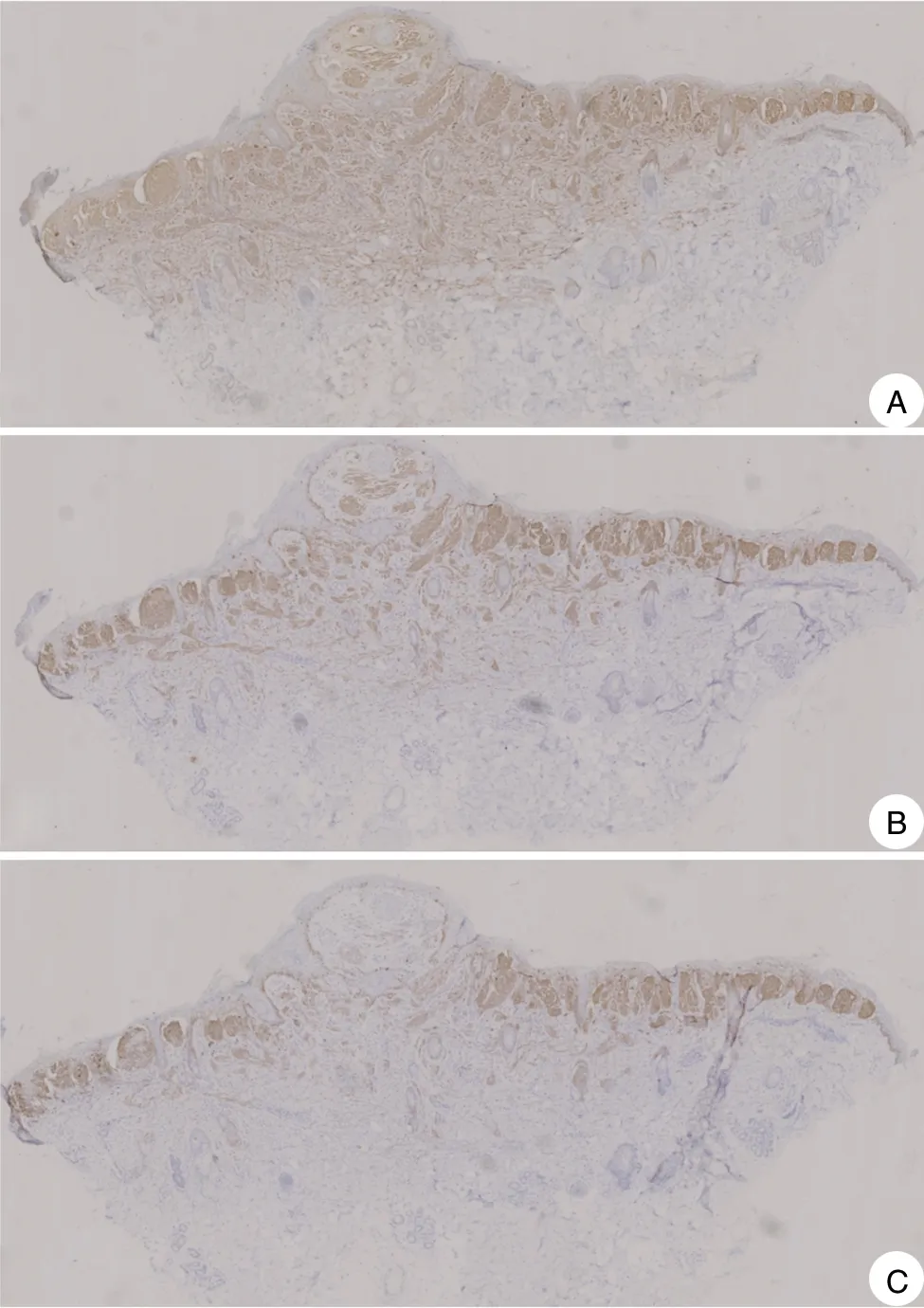
Figure 2. Immunohistochemical staining results of the lesion. (A)The majority of epithelioid cells were S100-positive in a diffuse staining pattern. (B) The majority of epithelioid cells were melan-Apositive. (C) Partial epithelioid cells were HMB-45-positive in a stratified staining pattern with fewer positive cells in the deep dermis.
Although dermoscopy is an appropriate and helpful method for diagnosing Spitz nevus,histopathological and immunohistochemical examinations are still needed to rule out malignancy, especially for uncommon or atypical dermoscopic patterns.
The management of Spitz nevus is still controversial.Age is one of the most important factors because the incidence of malignant melanoma increases with age. According to dermoscopic morphology of Spitz naevi and management guidelines by 2017 British Association of Dermatologists,5surgical excision should be reserved for suspicious lesions in children at 12 years of age and older and for all suspicious neoplasms with an atypical pattern when malignant melanoma cannot be excluded in children of all ages. Clinical and dermoscopic follow-up should be continued until these neoplasms maintain typical features of common nevi or disappear.
In conclusion, the reported case showed uncommon dermoscopic patterns containing concurrent pigmented and nonpigmented features,which may be a new clue for recognizing Spitz nevus under dermoscopy.While dermoscopy plays an important role in the differential diagnosis of Spitz nevus and melanoma, it is still necessary to perform a biopsy or excision for cases with suspicious clinical manifestations or atypical dermoscopic patterns.
Acknowledgements
This work was supported by the Beijing Natural Science Foundation (No. 7182127) and the Milstein Medical Asian American Partnership Foundation Research Project Award in Skin Disease.
- 國際皮膚性病學(xué)雜志的其它文章
- Blastic Plasmacytoid Dendritic Cell Neoplasm:A Case Report
- Subcutaneous Panniculitis-Like T-Cell Lymphoma: A Case Report
- Cutaneous Rosai–Dorfman Disease Presenting with Multiple Nodules on the Thighs and Buttocks
- Oculocutaneous Albinism with Squamous Cell Carcinoma, Bowen’s Disease and Actinic Keratosis: A Case Report
- Successful Treatment of Synovitis, Acne,Pustulosis, Hyperostosis and Osteitis Syndrome with Thalidomide: A Case Report
- Characteristics of Cutaneous and Subcutaneous Infectious Granuloma at a Signal Center in China:A Five-Year Retrospective Study