
Efficacy of thoracoscopic anatomical segmentectomy for small pulmonary nodules
2020-06-17 05:54:02HuiLiYangLiuBaoCunLingBoHu
World Journal of Clinical Cases 2020年11期
Hui Li, Yang Liu, Bao-Cun Ling, Bo Hu
Hui Li, Yang Liu, Bao-Cun Ling, Bo Hu, Cardiothoracic Surgery Department, Zibo Hospital, 960 Hospital of PLA, Zibo 255300, Shandong Province, China
Abstract
Key words: Thoracoscopy; Small pulmonary nodules; Anatomical segmentectomy;Clinical efficacy; Lobectomy
INTRODUCTION
Small pulmonary nodules are tissue shadows surrounded by gas-containing lung tissues with a diameter of 5-10 mm in clinical imaging. They are generally round and can be single or multiple. Various factors contribute to the formation of nodules:Benign nodules are usually caused by inflammation, tuberculosis, bleeding,etc.;malignant nodules are primary lung cancer or lung metastasis of malignant tumors[1].Epidemiology suggests that the incidence of small pulmonary nodules has increased in recent years with declining air quality[2].
Thoracoscopic lobectomy has been widely adopted since its first clinical application for the liver in 1993. The safety and efficacy of this surgical method have been proven in treating small pulmonary nodules, which is less invasive with rapid postoperative recovery[3]. To further improve the safety and reduce operative trauma of clinical surgery, some researchers suggest that a lobe can be divided into segments, and therefore more normal tissues can be preserved during segment resection and operative injury can be reduced, which is called anatomical segmentectomy[4].
Currently, thoracoscopic segmentectomy in China is still at the exploratory stage with limited application. To further evaluate the efficacy of this surgical method for small pulmonary nodules, this study retrospectively analyzed the medical records of 86 patients with small pulmonary nodules treated at our hospital.
MATERIALS AND METHODS
Baseline characteristics
The medical records of 86 patients with small pulmonary nodules treated at our hospital between August 2016 and October 2019 were reviewed. All cases met the diagnosis and treatment standards of “Chinese Expert Consensus on the Diagnosis and Treatment of Pulmonary nodules”[5]. The inclusion criteria were: (1) No serious cardio-cerebrovascular disease; (2) No human immunodeficiency virus, immune deficiency, or coagulation dysfunction; (3) No other malignant tumor or a previous history of lymphoma; (4) Normal mental and intellectual assessment results and no mental disorder or low intelligence; (5) The patient was informed of the study and consented to medical records usage; (6) Suspected malignant lesions on preoperative examination; (7) Enhanced computed tomography scan showing tumor diameter ≤ 2 cm; and (8) Distant metastasis excluded by positron emission tomography/computed tomography. The exclusion criteria were: (1) Insufficient clinical records; (2)Combined with serious infection; (3) Combined with multiple organ failure and massive hemorrhage; and (4) Number of met inclusion criteria < 8. According to the surgical option, patients who underwent thoracoscopic segmentectomy were included in an observation group (46 cases) and patients who underwent thoracoscopic lobectomy were included in a reference group (40 cases). The baseline characteristics of the two groups showed no significant difference (P> 0.05) (Table 1).
Surgical methods
The patient was placed in the lateral decubitus position under general anesthesia with single-lung ventilation by double-lumen endotracheal tube intubation. A 1-cm skin incision was made along the anterior axillary line in the 7thor 8thintercostal space(observation port), a 3-cm incision was made along the anterior axillary line in the 4th-5thintercostal space (working port), and another incision was made along the posterior axillary line in the 7thintercostal space (accessory working port). The scope was inserted through the observation port and apparatus was inserted through the working port. Lesion was detected by the scope. Segmentectomy was initially planned in 48 patients and pathological biopsy was obtained through wedge resection. Patients with benign lesions underwent segmentectomy. Biopsies and frozen pathological sections of the 10th, 11th, and 13thgroups of lymph nodes were further obtained and examined in patients with malignant lesions and 2 patients with positive diagnosis switched to lobectomy. Therefore, segmentectomy was finally performed in 46 patients. The resected segments were based on lesion location (left superior lobe: 3 cases of apico-posterior segment, 4 of anterior segment, 3 of lingular segment, and 2 of posterior segment; right inferior lobe: 4 cases of basal segment and 5 of dorsal segment; left inferior lobe: 6 cases of basal segment and 7 of dorsal segment; right superior lobe: 4 cases of apical segment, 3 of posterior segment, and 5 of anterior segment).A total of 40 patients underwent lobectomy and the resected parts were based on lesion location (12 cases of left upper lobe, 11 of left lower lobe, 9 of right upper lobe, and 8 of right lower lobe).
Observational indexes
Venous blood samples were taken from patients with positive pathological diagnosis at the 1stmo postoperatively. Serum was obtained after centrifugation and tested for serum carbohydrate antigen 19-9 (CA19-9), CA125, neuron-specific enolase, and squamous cell carcinoma antigen.
Spirometer (Fukuda Sangyo, St-75) was used to measure the percentage of forced vital capacity (FVC%), the percentage of forced expiratory volume in the first second(FEV1%), and the FEV1/FVC ratio (FEV1/FVC) before and 6 mo after operation.
Postoperative pain condition was assessed using the visual analogue scale (VAS).
Drainage volume, the number of resected lymph nodes, treatment cost, hospital stay, intraoperative bleeding volume, drainage time, and postoperative complications were recorded.
Statistical analysis
Data analyses were carried out with SPSS 23.0. Measurement data are presented as the mean ± SD and were analyzed byttest; enumeration data are expressed as percentages and were analyzed byχ2test.P< 0.05 indicated that the difference was statistically significant.
RESULTS
Comparison of serum tumor markers in patients with malignant lesions
In the reference group, 37 cases were malignant and 3 were benign; in the observation group, 35 cases were malignant and 11 were benign. Based on data shown in Table 2,no significance difference was observed in serum tumor markers between the two groups (P> 0.05).
Comparison of intraoperative bleeding volume, the number of resected lymph nodes, and drainage volume
Intraoperative bleeding and drainage volume were both significantly lower in the observation group (P< 0.05). No significant difference was observed in the number of resected lymph nodes between the two groups (P> 0.05, Table 3).
Comparison of hospital stay, treatment cost, drainage time, and visual analogue scale score
Hospital stay and drainage time were significantly shorter and VAS score was significantly lower in the observation group (P< 0.05). No significant difference was found in treatment cost (P> 0.05, Table 4).
Comparison of postoperative lung function

Table 1 Baseline characteristics, n (%)
Based on data shown in Table 5, no significant difference was observed in preoperative lung function index between the two groups (P> 0.05). Postoperative lung function index declined to certain extent in both groups, but FEV1%, FVC%, and FEV1/FVC were significantly higher in the observation group (P< 0.05).
Comparison of complications
Table 6 suggests that the incidence of complications was significantly lower in the observation group (P< 0.05).
DISCUSSION
Small pulmonary nodules are common manifestations of pulmonary lesions in clinical diagnosis, which generally refer to pulmonary nodules of 5-10 mm. Various factors may contribute to the formation of nodules, including inflammation, tuberculosis,primary tumor, and metastatic tumor[6-8]. Although clinical studies have shown that small pulmonary nodules have a relatively low tendency to turn malignant, the nodules should be handled carefully once observed. Epidemiology suggests that with declining air quality, the incidence of small pulmonary nodules has increased in recent years, which has become a typical lung lesion with an increasing malignancy rate[2].
Middle and lower thoracic wedge resection is primarily applied in previous clinical treatment, but in patients with extensive lesions (e.g., pulmonary bullae and pulmonary cyst), this method cannot completely resect the lesions, and in patients with deep lesions, this method may cause adverse events like vascular lesions.Moreover, since this operation is not anatomical resection, malignant lesion has a great risk of recurrence after operation and therefore, the application of this surgical method is limited[9]. Lobectomy, as another surgical option, has been widely applied in treating small pulmonary nodules, and especially in terms of malignant lesions, it can control disease progression and prolong patient survival[10]. In patients with malignant small pulmonary nodules who received lobectomy, the 5-year survival rate can reach over 80%[11]. Compared with conventional thoracotomy, thoracoscopic lobectomy can be operated through only 3 small incisions, which greatly reduces the risk of postoperative complications and has gradually replaced conventional thoracotomy, becoming the primary surgical treatment for small pulmonary nodules[12-14]. However, research now indicates that although lobectomy shows good therapeutic effects, it resects part of the normal lung tissues, resulting in impaired lung function, more surgical injury, and slower recovery, so the surgical method can be further improved[15].
In terms of pulmonary anatomy, the definition of pulmonary segment was first introduced in 1889, further refining the definition of pulmonary lobe in order to facilitate accurate localization in clinical diagnosis and treatment[16]. Thoracoscopic hepatic segmentectomy was initially applied in Italy, and the thoracoscopic segmentectomy was gradually introduced into other developed countries to treat small pulmonary nodules, which achieved satisfactory results. The application of anatomical pulmonary segmentectomy in China is relatively late and limited. Based on current theories, segmentectomy can preserve more normal lung tissues with less injury and impact on lung function while treating small pulmonary nodules. When meeting surgical indications, segmentectomy can achieve the same effect as lobectomy for lymph node resection[17]. The current consensual surgical signs include: (1)Nodules located at the peripheral 1/3 of the pulmonary field, with a diameter ≤ 2 cm;(2) If malignant, the tumor should be non-small cell cancer with tumor stage of T1N0M0; (3) Distant metastasis excluded by lymph node biopsy; and (4) Cardiopulmonary function tolerant of surgery[18]. Generally, in treating malignant small pulmonary nodules, if no lymph node metastasis is present, segmentectomy can achieve the same therapeutic effect as lobectomy. But if lymph node metastasisoccurs, lobectomy should be applied rather than segmentectomy in case of recurrence.Therefore, a preoperative pathological biopsy of lymph nodes for patients with the malignant lesion is of critical importance[19].

Table 2 Comparison of serum tumor markers in patients with malignant lesions (mean ± SD)
In this retrospective study, no significant difference was observed in serum tumor markers (CA125, CA19-9, squamous cell carcinoma antigen, and neuron-specific enolase), the number of resected lymph nodes, and treatment cost between observation and reference groups (P> 0.05), indicating that the two surgical methods can achieve the same therapeutic effects with similar cost for both benign and malignant small pulmonary nodules. However, in the segmentectomy group, hospital stay and drainage time were significantly shorter (P< 0.05) while intraoperative bleeding and drainage volume, VAS, and several postoperative lung function indexes were significantly higher (P <0.05), suggesting that segmentectomy can reduce surgical injury and hospital stay with less impact on lung function and fewer complications. Our results are in agreement with those of Ishikawaet al[20]who suggested that compared with lobectomy, segmentectomy is less invasive and preserves more normal lung tissues with less impact on lung function and more rapid postoperative recovery[20]. One limitation of the present study is the small number of patients. Only 86 cases were included and therefore the surgical and observational outcomes may be accidental. More cases are needed for subsequent studies.
Thoracoscopic pulmonary segmentectomy is an ideal surgical approach to treat small pulmonary nodules. Compared with thoracoscopic lobectomy, segmentectomy is associated with fewer complications, better postoperative lung function, and more rapid recovery and therefore can be a primary option for patients meeting surgical indications.

Table 3 Comparison of intraoperative bleeding volume, the number of resected lymph nodes, and drainage volume (mean ± SD)

Table 4 Comparison of hospital stay, treatment cost, drainage time, and visual analogue scale score (mean ± SD)
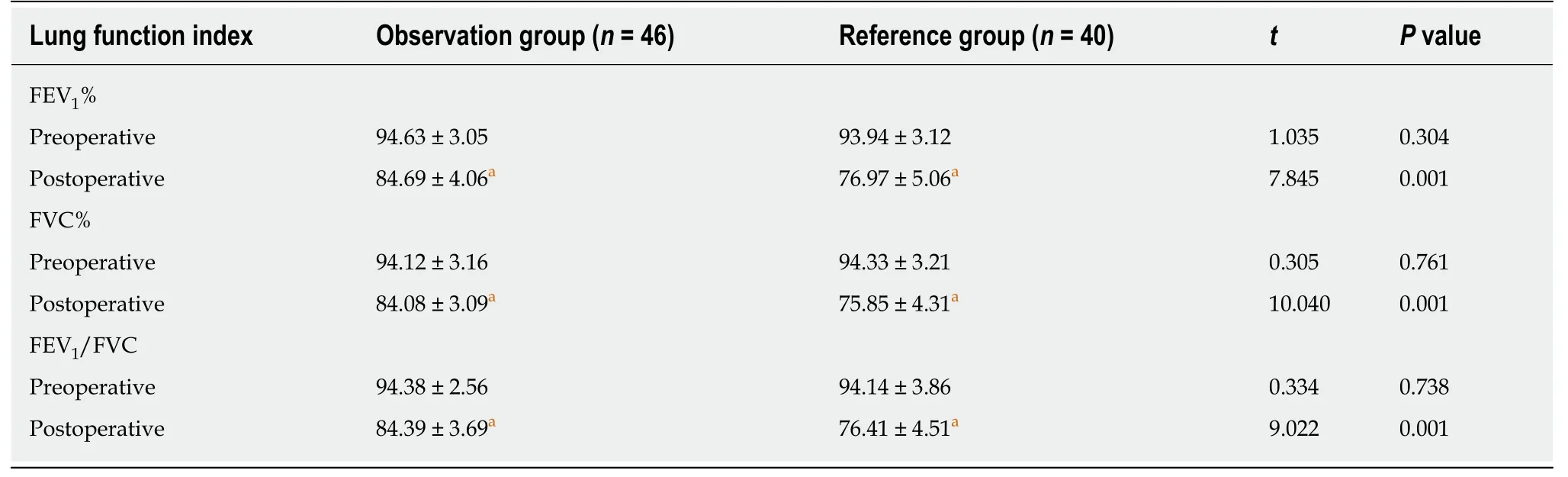
Table 5 Comparison of postoperative lung function (mean ± SD, %)

Table 6 Comparison of complications, n (%)
ARTICLE HIGHLIGHTS
Research background
Malignant nodules are primary lung cancer or lung metastasis of malignant tumors. Anatomical segmentectomy is a new surgical method.
Research motivation
Thoracoscopic segmentectomy in China is still at the exploratory stage.
Research objectives
To evaluate the availability and effectiveness of the procedure.
Research methods
Medical records of 86 patients with small pulmonary nodules treated at our hospital between August 2016 and October 2019 were retrospectively analyzed; 40 cases who underwent thoracoscopic lobectomy were set as a reference group, and 46 cases who underwent thoracoscopic anatomical segmentectomy were set as an observation group.
Research results
Intraoperative bleeding volume, drainage volume, drainage time, hospital stay, and visual analogue scale score were significantly lower in the observation group. The results of percentage of forced expiratory volume in the first second (FEV1%), the percentage of forced vital capacity(FVC%), and the FEV1/FVC ratio were significantly higher in the observation group.
Research conclusions
Thoracoscopic pulmonary segmentectomy is an ideal surgical approach to treat small pulmonary nodules.
Research perspectives
The authors will evaluate the overall situation of the patients to take the best surgical plan in the future.
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Macrophage activation syndrome as an initial presentation of systemic lupus erythematosus
- Optical coherence tomography guided treatment avoids stenting in an antiphospholipid syndrome patient: A case report
- Uterine incision dehiscence 3 mo after cesarean section causing massive bleeding: A case report
- Ataxia-telangiectasia complicated with Hodgkin's lymphoma: A case report
- Gastric pyloric gland adenoma resembling a submucosal tumor: A case report
- Reduced delay in diagnosis of odontogenic keratocysts with malignant transformation: A case report