
Effect of Governor Vessel-unblocking and mindrefreshing acupuncture plus functional training on neural development in infants with brain damage
2018-09-12 02:45:06LiuZhenhuan劉振寰ZhangMengtao張夢(mèng)桃LiYuxiu李玉秀YanXiaolan嚴(yán)曉嵐XieJieshan謝潔珊
Liu Zhen-huan (劉振寰), Zhang Meng-tao (張夢(mèng)桃), Li Yu-xiu (李玉秀), Yan Xiao-lan (嚴(yán)曉嵐), Xie Jie-shan (謝潔珊)
Abstract Objective: To observe the effect of Governor Vessel-unblocking and mind-refreshing acupuncture plus functional training on neural development in infants with brain damage and seek an effective method for early intervention of infantile brain damage.Methods: Eighty infants with brain injury were recruited and allocated to a treatment group and a control group by their visiting sequence, with 40 cases in each group. The control group received exercise training, 40 min each session and 6 sessions a week, and tuina treatment, 30 min each time and 6 times a week. Based on the treatment protocol for the control group, the treatment group additionally received Governor Vessel-unblocking and mind-refreshing acupuncture, 3 times a week and 10 sessions as a course at a 2-week interval. Before the treatment and after 14-week treatment, the gross motor function measure (GMFM) and developmental quotient (DQ) of Bejing Gesell developmental scale were used to evaluate the development of the infants.Results: After the treatment, the GMFM score and DQs of Gesell scale all increased by different levels in the two groups,and the intra-group differences were statistically significant (all P<0.05); the scores of the treatment group were superior to those of the control group, and the between-group differences were statistically significant (all P<0.05).Conclusion: Governor Vessel-unblocking and mind-refreshing acupuncture plus functional training can significantly promote the development of gross motor and cognitive functions in infants with brain damage, and it is an early and effective intervention for infantile brain damage.
Keywords: Acupuncture Therapy; Scalp Stimulation Areas; Tuina; Massage; Exercise Therapy; Brain Injuries; Child Development; Rehabilitation
Brain damage syndrome (BDS) refers to nonprogressive brain injuries that happen prior to, at or within 1 month after the birth due to various factors including intrauterine hypoxia, asphyxia neonatorum,hypoxic-ischemic encephalopathy (HIE), intracranial hemorrhage, premature birth, and low body weight(LBW), etc[1]. BDS is a transitional diagnosis often used for brain injury infants who are at a high risk yet cannot be diagnosed as cerebral palsy, mental retardation, or epilepsy[2]. With the development of perinatal and newborn intensive care techniques, the survival rate of LBW and premature infants has increased, but the accompanied infantile brain injury remains a significant problem[3-4]. Early detection, early diagnosis and early intervention will help to promote the development of motor function and intelligence of the infants, and reduce the incidence of cerebral palsy[5-7]. We took Governor Vessel-unblocking and mind-refreshing acupuncture plus functional training as early intervention to treat BDS infants and observed the effect of this treatment protocol on the neural development of the infants. The report is now given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnosis of brain injury referred to the Newborn Behaviors and Education for 0-3 Year-old Kids[1].
1.2 Inclusion criteria
Conforming to the above diagnostic criteria; aged 4-9 months; the guardian of the infant signed the informed consent form.
1.3 Exclusion criteria
Those with severe primary diseases involving cardiovascular system, liver, kidney or hematopoietic system; those in active stage of epilepsy; distance between the location of scalp acupoints or the needle tip after insertion and the edge of fontanel <1 cm;inherited metabolic diseases or progressive brain damages.
1.4 Dropout criteria
Those who failed to accomplish the intervention or observation; those who changed the intervention method halfway.
1.5 Statistical methods
The SPSS version 21.0 software was used for statistical analysis. Measurement data were expressed as mean ± standard deviation (±s). Intra-group comparisons were analyzed by paired t-test, while between-group comparisons were analyzed by independent sample t-test. Non-ranked enumeration data were processed by Chi-square test. P<0.05 was indicative of statistical significance.
1.6 General data
A total of 80 BDS infants were recruited from the inpatients admitted to the Department of Neurological Rehabilitation for Children, Nanhai Maternity and Children’s Hospital Affiliated to Guangzhou University of Chinese Medicine between January 2016 and December 2016. By following their visiting sequence,the patients were allocated to a treatment group and a control group, with 40 cases in each group. No patient dropped out in the treatment group while there were 6 dropouts in the control group (four asked for acupuncture-moxibustion treatment, one asked to be transferred to the outpatient for treatment of repetitive respiratory infection, and one returned to the local hospital for treatment due to the cost). As a result, 40 cases in the treatment group and 34 in the control group were enrolled for statistical analysis. The study process is shown in Figure 1. There were no significant differences in the general data between the two groups(all P>0.05), indicating the comparability (Table 1).
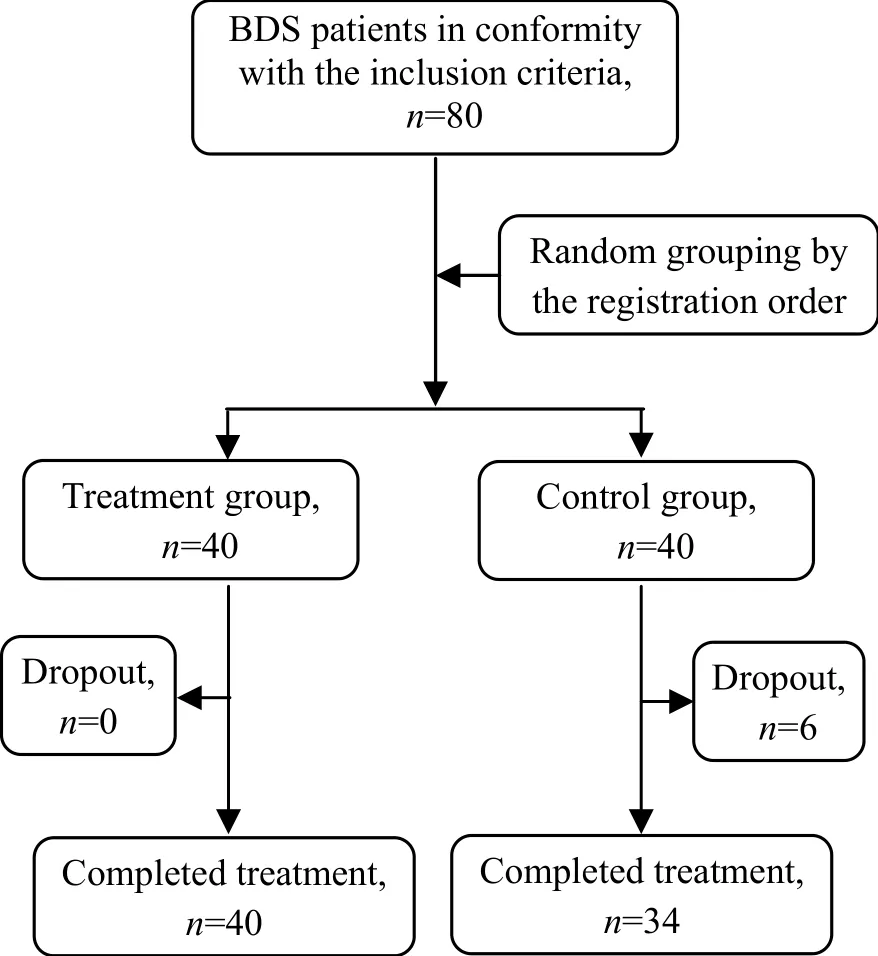
Figure 1. Flow chart of the study process

Table 1. Comparison of the general data
2 Treatment Methods
2.1 Control group
The control group was intervened by the early intervention training stipulated by our department,including kinesiotherapy and tuina.
Kinesiotherapy: Bobath therapy and Rood technique were taken as the major intervention, in combination with individualized training created by referring to the 3rd chapter of the Rehabilitation Atlas for Kid’s Motor Retardation[8]and by considering the kid’s real state of motor development, 40 min each session and 6 sessions a week for 14 weeks in total.
Tuina treatment: Well-directed tuina treatment was selected by referring to the 6th chapter of the Rehabilitation Atlas for Kid’s Motor Retardation and by considering the motor and intelligent development as well as the accompanied symptoms, 30 min each session and 6 sessions a week for 14 weeks in total.
2.2 Treatment group
In addition to the treatment for the control group,the treatment group received Governor Vesselunblocking and mind-refreshing acupuncture.
2.2.1 Scalp acupuncture for awakening mind
Points: Shenting (GV 24), Qianding (GV 21), Baihui(GV 20), Naohu (GV 17), Sishencong (EX-HN 1), Benshen(GB 13), and the Motor Area and Balance Area of Jiao’s scalp acupuncture.
Method: Disposable filiform needles of 0.30 mm in diameter and 25-40 mm in length were used. After sterilization, the needles were quickly punctured. Pointtoward-point needling was performed at Shenting(GV 24) with the needle tip towards Qianding (GV 21)and at Baihui (GV 20) with the needle tip towards Naohu (GV 17). The needles were retained for 30-60 min and the insertion holes were pressed by medical cotton balls for 3-5 min at the removal of needles. The treatment was performed 3 times a week with 10 times as 1 course at a 2-week interval for 3 courses in total.
2.2.2 Acupuncture for unblocking the Governor Vessel and reinforcing the kidney
Major points: Fengfu (GV 16), Shenzhu (GV 12),Zhiyang (GV 9), Jinsuo (GV 8), Yaoyangguan (GV 3) and Mingmen (GV 4).
Adjunct points: Pishu (BL 20) and Zusanli (ST 36) were added for spleen-stomach deficiency; Shenshu (BL 23),Sanyinjiao (SP 6) and Taixi (KI 3) were added for kidney essence insufficiency.
Method: Disposable filiform needles of 0.30 mm in diameter and 25-40 mm in length were used. After sterilization, needles were inserted in an ordinary way and remained for 5 min. The needles were not retained if the kid cried intensively. The treatment was performed 3 times a week with 10 times as 1 course at a 2-week interval for 3 courses in total.
3 Observation of Therapeutic Efficacy
3.1 Observation items
The following items were measured by professionals before and after the intervention.
3.1.1 Gross motor function measure (GMFM)
GMFM consists of 88 items which are classified into 5 dimensions: dimension A (lying and rolling), full score 51; dimension B (sitting), full score 39; dimension C(crawling and kneeling), full score 42; dimension D(standing), full score 39; dimension E (walking, running and jumping), full score 72. The percentage of each dimension = Total dimension score ÷ Full dimension score × 100%.
This study only measured dimension A, B and C due to the age of the enrolled subjects.
3.1.2 Beijing Gesell developmental scale
Gesell scale was used to evaluate the kid’s developmental quotient (DQ). This scale includes five dimensions: social adaptive, personal-social, gross motor, fine motor and language. The DQ was calculated by following the instructions by Gesell, including detection sequence, operation and tools, in combination with the daily activities, habits and capabilities of the kids. Beijing Gesell developmental scale is a version modified according to the development of Chinese kids, suitable for those aged 0-6 years.
3.2 Results
3.2.1 GMFM score
Before the treatment, there were no significant differences in the scores of GMFM dimension A, B and C between the two groups (all P>0.05), indicating the comparability. After 14-week treatment, the scores of GMFM dimension A, B and C increased significantly in both groups (all P<0.01), and there were significant differences in the scores between the two groups(P<0.05), showing that the development of gross motor function in the treatment group was better than that in the control group (Table 2).
3.2.2 DQ of Beijing Gesell developmental scale
Before the treatment, there were no significant differences in the DQ score of each dimension in Beijing Gesell developmental scale between the two groups (all P>0.05), indicating the comparability. After 14-week treatment, the DQ score of each dimension of Gesell developmental scale increased by different levels in the two groups (all P<0.01). There were significant differences in the DQ scores between the two groups after the intervention (all P<0.05), showing that the development of the kids in the treatment group was superior to that in the control group (Table 3).
Table 2. Comparison of the GMFM score (±s, point)
Note: Ⅰntra-group comparison, 1) t=7.348, P=0.000; 2) t=13.680, P=0.000; 3) t=6.002, P=0.000; 4) t=4.136, P=0.000; 5) t=7.467, P=0.000;6) t=4.251, P=0.000
?
Table 3. Comparison of the DQ scores in Beijing Gesell developmental scale (±s, point)

Table 3. Comparison of the DQ scores in Beijing Gesell developmental scale (±s, point)
Note: Compared with the control group at the same time point, 1) t=0.323, P=0.747; 2) t=0.326, P=0.744; 3) t=0.199, P=0.842; 4) t=0.417,P=0.677; 5) t=0.114, P=0.908; 6) t=2.600, P=0.011; 7) t=2.757, P=0.007; 8) t=2.679, P=0.009; 9) t=2.696, P=0.008; 10) t=2.426, P=0.017
Ⅰtem Treatment group (n=40) Control group (n=34)Before treatment After treatment t-value P-value Before treatmentAfter treatment t-value P-value Social adaptive 43.86±17.991) 61.43±15.646) 7.830 0.000 42.54±16.87 51.86±15.89 4.771 0.000 Personal-social 42.71±17.032) 61.90±16.287) 8.093 0.000 41.42±16.80 50.99±17.52 4.981 0.000 Gross motor 40.21±16.583) 57.98±16.338) 3.998 0.000 39.45±16.09 47.86±16.02 4.532 0.000 Fine motor 39.98±16.024) 58.11±16.479) 5.203 0.000 38.43±15.77 47.54±17.09 5.121 0.000 Language 40.54±15.775) 57.43±15.4510) 3.890 0.000 40.11±16.08 48.51±16.02 4.675 0.000
4 Discussion
BDS is a transitional diagnosis for infants after brain injury but before cerebral palsy or mental retardation[9].Before the development of this term, central coordination disturbance (CCD) was used to describe the early-stage symptom of brain injury-induced cerebral palsy[10]. The invention of this item avoids both missed diagnosis of cerebral palsy due to delayed symptoms and over-diagnosis of cerebral palsy, allowing the brain injury infants <1 year old to receive standardized diagnosis and treatment[11]. Brain tissues and neural function are gradually developing in infants,and the developing speed and plasticity of neural and motor functions before 2 years old are the highest[12]. In this stage, because of the immaturity and high plasticity of brain, the abnormal postures and movement are not fixed yet and early intervention can prevent the development of sequelae such as muscular atrophy,spasm, and deformed joints. Therefore, brain injury in perinatal stage should receive early intervention and rehabilitation. Early discover, early diagnosis and early intervention in those who are at a high risk are the key in reducing the occurrence of cerebral palsy[11]. In 1990s,a foreign study had proved the significance of early intervention in the prevention of residual disabilities after brain injury in infants[13]. Modern rehabilitation medicine has not brought up the training specifically for BDS. Currently, the early intervention mainly refers to the rehabilitation for early-stage cerebral palsy and relevant rehabilitation knowledge. In clinic, BDS is usually treated with comprehensive treatment consisting of Bobath, Vojta and Rood techniques for neural development, as well as acupuncture and tuina.
According to the clinical manifestations, BDS belongs to the scopes of Wu Chi (five types of retardation), Wu Ruan (five types of flaccidity) and Wu Ying (five types of stiffness). It mainly affects the brain, but is also closely related to the Governor Vessel, spleen and kidney[14].Traditional Chinese medicine holds that brain houses the primordial spirit. Brain connects with the five sense organs and Zang-fu organs via meridians and collaterals.The Governor Vessel is the sea of yang meridians and one of the predominant meridians in the meridian system. The collateral of Governor Vessel connects with the kidney and crosses the Meridian of Foot Yangming.It can integrate the prenatal and postnatal qi to adjust both the prenatal and the postnatal. Whether the meridian qi in the Governor Vessel is sufficient and smooth directly associates with the mental state of human body and the function of brain. Our previous studies found that Governor Vessel-unblocking and mind-refreshing acupuncture plus functional training promoted the development of brain parenchyma of brain injury kids[15-16], improved both gross and fine motor functions of cerebral palsy kids[17], and enhanced the development of intelligence and language[18-19].
Hence, the current study adopted Governor Vesselunblocking and mind-refreshing acupuncture in addition to functional training for early intervention of BDS kids. The results showed that the GMFM score and DQ scores in Beijing Gesell scale were significantly better in the treatment group than in the control group,indicating that Governor Vessel-unblocking and mind-refreshing acupuncture plus functional training should be superior to monotherapy of functional training in promoting the development of motor and cognitive functions in brain injury infants, and this method can be taken as an effective protocol for early intervention of BDS.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
Acknowledgments
This work was supported by Scientific Research Project of Traditional Chinese Medicine Bureau of Guangdong Province (廣東省中醫(yī)藥局科研課題, No.20151104).
Statement of Informed Consent
Ⅰnformed consent was obtained from the guardians of the recruited children in this study.
Received: 25 October 2017/Accepted: 29 November 2017
猜你喜歡
海南開(kāi)放大學(xué)學(xué)報(bào)(2021年4期)2022-01-24 13:13:22
Journal of Acupuncture and Tuina Science(2020年2期)2020-04-21 07:07:28
模具制造(2019年4期)2019-12-29 05:18:58
Journal of Acupuncture and Tuina Science(2018年3期)2018-06-28 09:27:58
海洋信息技術(shù)與應(yīng)用(2017年2期)2017-06-21 19:51:29
中國(guó)工程咨詢(xún)(2016年4期)2016-02-14 07:28:42
未來(lái)教育家(2014年1期)2014-03-20 22:39:40
中國(guó)中醫(yī)藥現(xiàn)代遠(yuǎn)程教育(2014年23期)2014-03-01 04:33:41
法人(2014年2期)2014-02-27 10:41:35
城市道橋與防洪(2013年6期)2013-03-11 15:17:10
 Journal of Acupuncture and Tuina Science2018年4期
Journal of Acupuncture and Tuina Science2018年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Modern quantum theories and experimental achievements motivate new exploration of acupuncture in traditional Chinese medicine
- Application and exploration of suspended magnetic moxibustion cup for obesity
- Therapeutic efficacy observation on acupuncture for persistent allergic rhinitis
- Correlation analysis on clinical effects of acupuncture for elderly patients with sensorineural deafness and ear distending sensation
- Effects of acupuncture on ovarian blood supply and pregnancy outcomes in patients receiving assisted reproduction
- Observation of therapeutic effects of point application at Shenque (CV 8) plus moxa-salt hot compress for prevention of gastrointestinal adverse reactions after chemotherapy for non-Hodgkin lymphoma