
Pulmonary Carcinosarcoma with Intracardiac Extension: a Case Report
2015-02-08 07:21:57YeqiSunPengChen2andQiangZhao
Chinese Medical Sciences Journal 2015年3期
Ye-qi Sun*, Peng Chen2, and Qiang Zhao
1Department of Pathology, First Affiliated Hospital,2Institute of Pharmacy and Pharmacology, University of South China, Hengyang, Hunan 421001, China
Pulmonary Carcinosarcoma with Intracardiac Extension: a Case Report
Ye-qi Sun1*, Peng Chen2, and Qiang Zhao1
1Department of Pathology, First Affiliated Hospital,2Institute of Pharmacy and Pharmacology, University of South China, Hengyang, Hunan 421001, China
pulmonary carcinosarcoma; epithelial-mesenchymal transition; cardiac mass; pneumonectomy
Chin Med Sci J 2015; 30(3):193-195
PRIMARY pulmonary sarcomatoid carcinoma (PSC) is a rare condition, approximately accounting for 0.1%-0.4% of all lung malignancies.1PSCs consist of5major histological variants according to 2004 WHO classification: pleomorphic carcinoma, spindle cell carcinoma, giant cell carcinoma, carcinosarcoma, and pulmonary blastoma.2PSC patients are predominantly male smokers with an average age of 65 years at diagnosis.3Carcinosarcoma is a biphasic tumor characterized by an admixture of both malignant epithelial and mesenchymal components as in well-defined carcinomas and sarcomas.4In this article, we reported a rare female case of pulmonary carcinosarcoma with intracardiac extension.
Though it is the second reported case of this condition,5it is the first happened in uncommon population (female, non-smokers) with very misleading and different symptoms. Cardiac and pulmonary surgeries were performed in succession due to negative preoperative examination and poor cardio-pulmonary function.
CASE DESCRIPTION
A 32-year-old Chinese woman who had no special medical and smoking history was hospitalized for increased dyspnea, chest congestion for over a week and sudden onset of cough and sputum. She was suspected of having atrial myxoma in echocardiography at other hospital. It seemed that her difficulty in breathing was triggered by this benign tumor. Complete physical examination in our hospital supported atrial myxoma, even though not responding to symptomatic therapy at the other hospital. At the first night after admission, she suffered from acute heart failure and was given emergency and effective cardiotonic treatment. Subsequent echocardiography showed spaceoccupying mass in cardiac and left pulmonary veins and cardiomegaly. Chest computed tomography (CT) revealed pulmonary edema and right lung lower lobe consolidation (Fig. 1). Follow-up transthoracic needle aspiration produced no positive result. All the findings suggested a benign cardiac tumor with pulmonary embolism.
Given the poor cardio-pulmonary function of this patient, we decided to remove the left atrial mass first. When the left atrium was opened via the right atrium wall and fossa ovalis, a 6 cm×5 cm×5 cm mass in the leftatrium was exposed and its tumor pedicle was located on inferior pulmonary vein. Mitral ring, atrial septum, and other connected pulmonary vessels were not involved. Resected lesions showed complete spindle cell component with extensive mucinous degeneration and low mitotic count. Since the resected tissues stained positive for Vim and negative for CK on immuohistochemical examination (Fig. 2), we concluded that the mass was originated from soft tissue and the potential of low-grade malignancy could not be ruled out.
One week later, when the state of her body had benefited from the first surgery, a 8 cm×6 cm×6 cm tumor at peripheral left lower lung was resected without involving surrounding tissues, which was positive for Vim and negative for CK. The resected tumor, along with satellite nodule and pulmonary interlobal lymph node, all showed a predominantly spindle cell component with mucinous degeneration and a few scattered bizarre cells. Furthermore, there was a small mount of definite moderately differentiated adenocarcinoma cells, which was supported by TTF1 (Fig. 3).
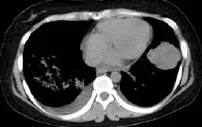
Figure 1. Chest CT showed pulmonary edema and right lung lower mass.

Figure 2. Pathological examination shows spindle cell component of cardiac tumor (A) and adenocarcinoma and mesenchymal component in lung lesion (B) (HE ×400).
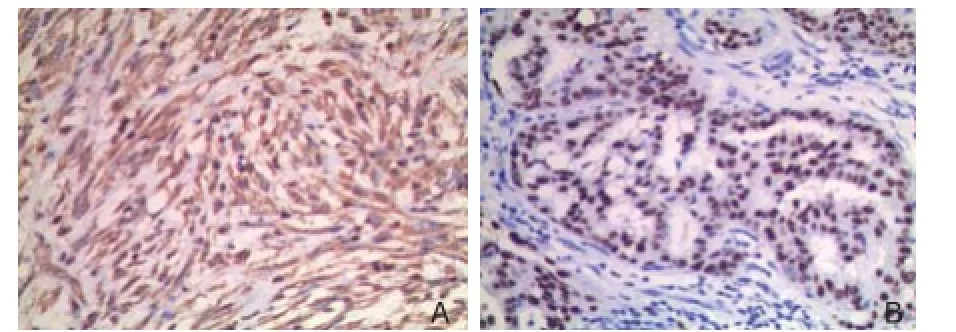
Figure 3. Pathological examination with immuohistochemical staining shows spindle cell component stained positive for vimentin (A) and accentuated pattern of nucleus of adenocarcinoma with immunohistochemical marker TTF1 (B) (×400).
The pathological analysis of the left atrial tumour and specimen of pneumonectomy confirmed the diagnosis of pulmonary carcinosarcoma with intracardiac extension. The sarcomatoid part was formed by fibrosarcoma with mucinous degeneration.
Terribly as expected, the patient died 2 months later due to multiple metastatic sites, including brain, spine, and contralateral lung.
DISCUSSION
Ng et al5reported the first case of primary PSC with intracardiac extension, a 53-year-old Chinese male smoker having arrhythmia and chest discomfort. His pulmonary mass was located in the peripheral right lower lobe. By contrast, this woman had never smoked, and presented with very confusing symptom of chest congestion, dyspnea and acute heart failure. In addition, the position of her lung tumor was in the left lung. Therefore, the diagnosis was not confirmed until both postoperative pathological analyses came out.
Epithelial-mesenchymal transition is the best explanation at present to the mechanism of carcinosarcoma, a complex series of physical and cellular events resulting in the loss of characteristic epithelial traits of carcinoma cells and acquisition of mesenchymal traits.4The primary lung lesion in this case was composed of both components, but in satellite nodule and metastatic lymph gland only mesenchymal part was noted. In addition, it was strange that no epithelial component was found in the heart tumor. Apparently, stromal component which originated in carcinoma showed more aggressive traits.
PSC presents as either a central or peripheral lesion, often in the upper lobe,2,6while the position of the first reported case was in the lower lobe.5Life expectancy of poorly differentiated PSC is generally thought to be shorter than that in patients with conventional non-small-cell carcinomas.7
In conclusion, even in unusual population (female, non-smokers), suspicion of pulmonary carcinosarcoma is still needed in the setting of chest congestion, poor cardiopulmonary function, cardiac mass and intrapulmonary lesion. Sometimes, it is useful to carry out the skin lung puncture for primary diagnosis of pulmonary peripheral tumor.5Unfortunately, the result of biopsy was negative in this case. We performed decisive cardiac tumor resection to improve deteriorating cardiopulmonary function and facilitate the following pneumonectomy. So it is wise to perform operation to alleviate symptoms instead of operation for correct diagnosis. Besides, the growthpattern and histopathological features of cardiac tumor could help to identify the source of the tumor.
1. Park JS, Lee Y, Han J, et al. Clinicopathologic outcomes of curative resection for sarcomatoid carcinoma of the lung. Oncology 2011; 81: 206-13.
2. Travis WD, Brambilla E, Muller-Hermelink HK, et al. Pathology and genetics of tumors of the lung, pleura, thymus and heart. In: World Health Organization classification of tumours. Lyon: IARC Press; 2004. p. 54-61.
3. Franks TJ, Galvin JR. Sarcomatoid carcinoma of the lung: histologic criteria and common lesion in the differential diagnosis. Arch Pahol Lab Med 2010; 134: 49-54.
4. Thomas VT, Hinson S, Konduri K. Epithelial–mesenchymal transition in pulmonary carcinosarcoma: case report and literature review. Therapeutic Advances in Medical Oncology 2011; 4: 31-7.
5. Ng SW, Lim CH, Wang CW, et al. Primary pulmonary sarcomoid carcinoma with intracardiac extension. J Thorac Carciovasc Surg 2006; 54: 416-9.
6. Pelosi G, Sonzogni A, De-pas T, et al. Pulmonary sarcomatoid carcinoma: a practical overview. Int J of Surg Pahthol 2010; 18: 103-20.
7. Chang YL, Lee YC, Shih JY, et al. Pulmonary pleomorphic (spindle) cell carcinoma: peculiar clinicopathologic manifestations different from ordinary non-small cell carcinoma. Lung Cancer 2001; 34: 91-7.
Received for publication June 12, 2014.
*Corresponding author Tel/Fax: 86-734-8578938, E-mail: liuliuqiqime@ 163.com
 Chinese Medical Sciences Journal2015年3期
Chinese Medical Sciences Journal2015年3期
- Chinese Medical Sciences Journal的其它文章
- Paraneoplastic Dermatomyositis Accompanying Nasopharyngeal Carcinoma
- Genetic Effects on Sensorineural Hearing Loss and Evidence-based Treatment for Sensorineural Hearing Loss
- Serum Myeloperoxidase Level in Systemic Lupus Erythematosus
- Postpartum Atypical Hemolytic Uremic Syndrome: an Unusual and Severe Complication Associated with IgA Nephropathy
- Double Roots of Mandibular Premolar in Full-mouth Periapical Films
- Cerebrospinal Fluid Biomarkers in Dementia Patients with Cerebral Amyloid Angiopathy