
Predictors of permanent pacemaker implantation following transcatheter aortic valve replacement-the search is still on!
2024-05-07 10:41:32SudeshPrajapathiAkshyayaPradhan
World Journal of Cardiology 2024年3期
Sudesh Prajapathi,Akshyaya Pradhan
Abstract Several anatomical,demographic,clinical,electrocardiographic,procedural,and valve-related variables can be used to predict the probability of developing conduction abnormalities after transcatheter aortic valve replacement (TAVR) that necessitate permanent pacemaker (PPM) implantation.These variables include calcifications around the device landing zone and in the mitral annulus;preexisting electrocardiographic abnormalities such as left and right bundle branch blocks (BBB),first-and second-degree atrioventricular blocks,as well as bifascicular and trifascicular blocks;male sex;diabetes mellitus (DM);hypertension;history of atrial fibrillation;renal failure;dementia;and use of self-expanding valves.The current study supports existing literature by demonstrating that type 2 DM and baseline right BBB are significant predictors of PPM implantation post-TAVR.Regardless of the side of the BBB,this study demonstrated,for the first time,a linear association between the incidence of PPM implantation post-TAVR and every 20 ms increase in baseline QRS duration (above 100 ms).After a 1-year follow-up,patients who received PPM post-TAVR had a higher rate of hospitalization for heart failure and nonfatal myocardial infarction.
Key Words: Bundle branch block;Self expanding aortic valve;Atrioventricular node;Diabetes mellitus;QRS duration
INTRODUCTION
High-grade atrioventricular (AV) block and new-onset left bundle branch block (BBB) are the most common conduction abnormalities that occur after transcatheter aortic valve replacement (TAVR).However,almost 50% of these may improve with the resolution of perivalvular edema and inflammation post-TAVR.Previous studies have demonstrated that approximately 60%-96% and 2%-7% of patients develop high-degree AV block within 24 and 48 h,respectively[1].At present,a trend toward early discharge from the hospital post-TAVR (median day 2) has led to an increase in the incidence of permanent pacemaker (PPM) implantation post-TAVR.However,the overall rates of PPM implantation within 30 d of TAVR have remained constant (11%) since 2012[2].Various anatomical,demographic,clinical,electrocardiographic,procedural,and valve-related factors contribute to post-TAVR conduction blocks and have been previously reported.The anatomical proximity of the bundle of His and AV nodes to the aortic valve (Figure 1) and the direct mechanical injury to this conduction system during valve deployment,along with individual variation in the anteroposterior positioning of the AV node and His bundle close to the AV valve,increase the risk of developing post-TAVR heart block[3].Mitral annular calcifications and calcifications near the device landing zone further increase this risk[4].In addition,pre-existing electrocardiographic abnormalities,such as right and left BBB,first-and second-degree AV blocks,as well as bifascicular and trifascicular blocks,increase the necessity for PPM implantation during or after the procedure.Anatomically,the left bundle is anterior and closer to the aortic annulus and is prone to injury during valve deployment;this makes pre-existing right BBB among the most significant risk factors[4],aside from the patients’ clinical and demographic traits.A study that analyzed 62083 patients who underwent TAVR from 2012 to 2017 reported that male sex,diabetes mellitus (DM),hypertension,history of atrial fibrillation (AF),renal dysfunction,and dementia were significant predictors of PPM implantation within 30 d post-TAVR[2,5].Both a history of AF and new-onset AF were found to be independently associated with an increased risk of PPM implantation post-TAVR.A meta-analysis revealed that new-onset AF is associated with mortality,stroke,major bleeding,PPM implantation,and longer in-hospital stay[6].The use of self-expandable valves (SEV) was also found to pose a higher risk of conduction abnormalities post-TAVR than the use of balloon-expandable valves (BEV).In previous studies,the incidence rate of new-onset left BBB was found to be higher in patients who received a self-expandable CoreValve (Medtronic Inc.,Minneapolis,MN,United States) (27%,range 9%-65%) than those who received the balloon-expandable Sapien valve (Edwards Lifesciences Inc.,Irvine,CA,United States) (11%,range 4%-18%)[4].However,there is a scarcity of data to compare new-generation SEVs with BEVs.A recent trial that compared the two valves demonstrated equivalence for primary valve-related efficacy endpoints of all-cause mortality,stroke,moderate or severe prosthetic valve regurgitation,and PPM implantation within 30 d post-TAVR[7].
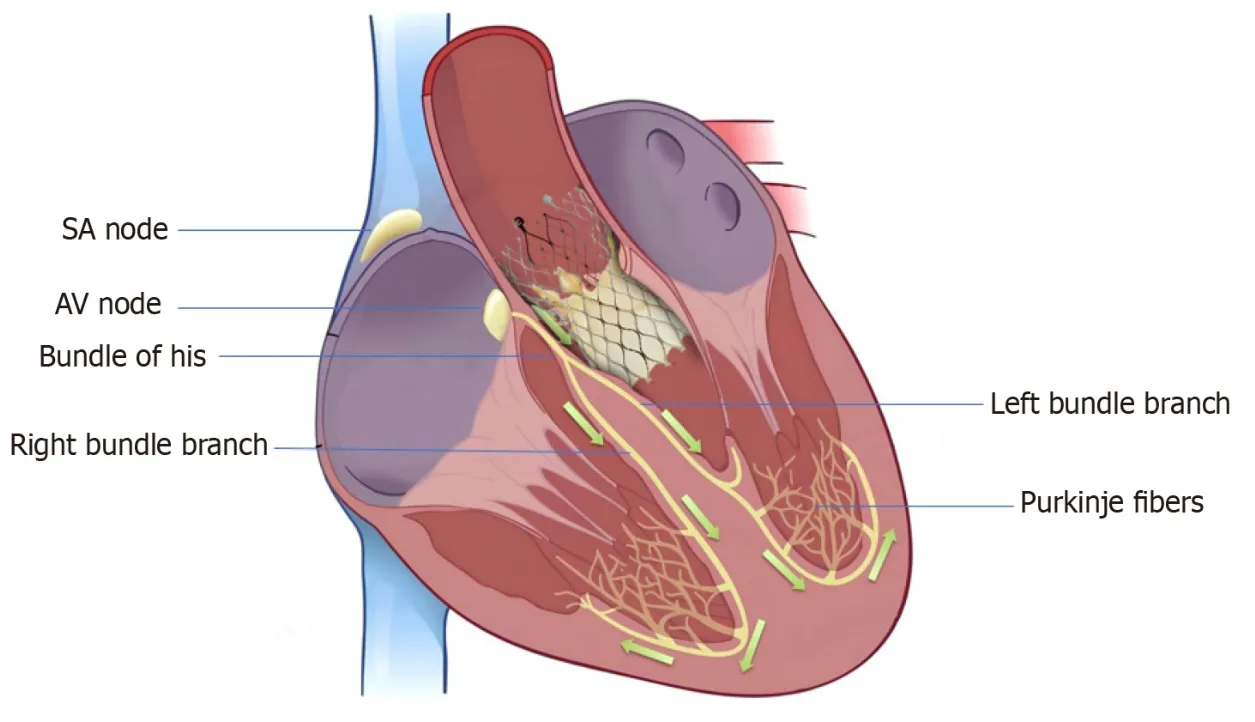
Figure 1 Anatomical proximity of the transcatheter aortic valve replacement valve to the cardiac conduction system. SA: Sino-atrial;AV: Atrio-ventricular.
Various procedural factors such as transapical access,balloon pre-and post-dilation,prosthesis oversizing (more than 15%-20%),and lower implantation depth also add to the risk (Figure 2)[4].
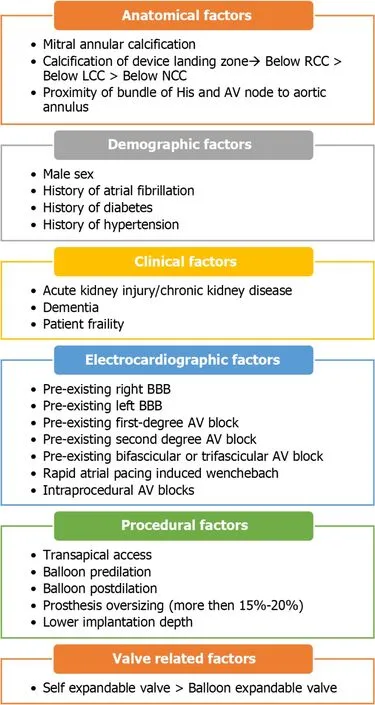
Figure 2 Predictors of permanent pacemaker implantation after transcatheter aortic valve replacement[1-5]. RCC: Right coronary cusp;LCC: Left coronary cusp;NCC: Non-coronary cusp;AV: Atrioventricular;BBB: Bundle branch block.
In a retrospective cohort study published in the journal by Nwaedozieet al[8],patients undergoing TAVR between 2012 and 2019,were followed for 1 year.The effect of baseline DM,supraventricular arrhythmia,and pre-existing nonspecific interventricular conduction delay (QRS duration > 120 ms without any right BBB or left BBB morphology) on the incidence of PPM implantation post-TAVR was analyzed[8].The study included 357 patients with a mean age of 80 years.Of these patients,57 (16%) required PPM implantation post-TAVR whereas the remainder did not.With the exception of type 2 DM,which predominated in the pacemaker group,baseline variables such as cardiac risk factors and valve type were similar across the two groups.In this study,the frequency of pacemaker implantation was significantly greater in individuals with pre-existing DM,pre-existing right BBB,QRS duration > 120 ms,and prolonged QTc interval.Furthermore,the incidence of pacemaker implantation continuously increased for every 20-ms increase in duration of baseline QRS segment (above 100 ms).A marginally significant finding was the association between preoperative supraventricular arrhythmia (AF,atrial flutter,junctional rhythm) and a higher incidence of PPM implantation.The association between DM and the risk of PPM implantation post-TAVR was also previously reported,although not extensively studied.The present study reported baseline DM as a significant predictor of pacemaker implantation post-TAVR [adjusted odds ratio (OR)=2.16].Furthermore,a previous study has reported that pre-existing right BBB and QRS duration > 120 ms predict the need for PPM implantation post-TAVR[4].However,this study vehemently indicated the increasing OR for the incidence of pacemaker implantation for every 20-ms increase in duration of QRS segment greater than 100 ms.No previous study has demonstrated such a collinear association between QRS duration and an increased risk of PPM implantation post-TAVR.Moreover,only a few studies in the literature have demonstrated the association of pre-existing nonspecific interventricular conduction delay,defined as QRS duration > 120 ms without any right BBB or left BBB morphology,with the risk of PPM implantation post-TAVR.Patients with a longer QTC interval had an OR of 2.94 for PPM placement compared with those with a normal QTc interval due to the collinearity between the QRS and QTc intervals.The authors reported that QTc intervals and PPM implantation did not significantly correlate after stratification by abnormal QRS intervals.In previous studies,a history of AF was found to be consistently associated with the incidence of PPM implantation post-TAVR.However,the present study reported that a history of supraventricular arrhythmia (composite of AF,atrial flutter,and junctional rhythm) is marginally associated with the risk of PPM implantation post-TAVR (P=0.54),which appears to be a novel finding in the existing literature.This finding in the present study seems to have been driven by a higher number of patients with AF than those with atrial flutter and junctional rhythm in the supraventricular arrhythmia group.Contrary to the existing literature,this study did not show a statistically significant increase in the risk of PPM implantation with SEVs compared with BEVs.The authors owe this to the long experience of operators with SEV in their institution.Additionally,manufacturer-assisted changes in SEV implantation techniques such as usage of cusp overlap technique and shallower implantation of TAVR valve in the left ventricular outflow tract possibly avoid the anatomical proximity with the conduction system during TAVR.The investigators reported a higher incidence of hospitalization for heart failure and nonfatal myocardial infarction (MI) at 1-year follow-up in the PPM cohort,with no difference in mortality.As this study is a retrospective review conducted in a single center,it might not accurately represent the situation in other geographical areas.Furthermore,the valves were not randomly assigned to the patients according to any predetermined criteria;rather,the assignment was decided by the multidisciplinary TAVR team.Although an equal distribution of valves in both groups was observed,the author claimed that this factor might not have affected the study results.This study supports the existing literature by demonstrating that type 2 DM and baseline right BBB are significant predictors of PPM implantation post-TAVR.For the first time,this study demonstrated a linear association between the incidence of PPM implantation post-TAVR and every 20-ms increase in duration of baseline QRS segment (above 100 ms).Thus,regardless of the side of BBB morphology,patients with a QRS duration above 100 ms are more likely to require permanent PPM implantation post-TAVR.The post-TAVR PPM cohort was also reported to have a higher rate of hospitalization for heart failure and nonfatal MI at 1-year follow-up,although no significant difference in mortality was observed.However,future studies are warranted to validate these findings,and the pathophysiological basis needs to be elucidated.
CONCLUSION
In summary,this study adds several unique predictors to the existing ones,such as a history of supraventricular arrhythmia and increased QRS duration above 100 ms.Interestingly,the use of SEV in this study did not result in a higher risk of PPM implantation compared with BEV,as previously reported.This could be due to manufacture-assisted changes in SEV implantation techniques,allowing shallow implantation depth.The present study supports the existing literature by demonstrating that type 2 DM and baseline right BBB are significant predictors of PPM implantation post-TAVR.
FOOTNOTES
Author contributions:Pradhan A devised the concept and performed the literature search;Prajapathi S prepared the first draft,and Pradhan A critically reviewed the draft;Prajapathi S prepared the final manuscript,and Pradhan A submitted it.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:India
ORCID number:Akshyaya Pradhan 0000-0002-2360-7580.
Corresponding Author's Membership in Professional Societies:American Heart Association;American College of Cardiology.
S-Editor:Li L
L-Editor:Webster JR
P-Editor:Zhao S
 World Journal of Cardiology2024年3期
World Journal of Cardiology2024年3期
- World Journal of Cardiology的其它文章
- Cardiovascular diseases in European ethnic minorities: Beyond the traditional cardiovascular risk factors
- Severe hypoxemia after radiofrequency ablation for atrial fibrillation in palliatively repaired tetralogy of Fallot: A case report
- Epicardial adipose tissue in obesity with heart failure with preserved ejection fraction: Cardiovascular magnetic resonance biomarker study
- Sex and racial disparities in non-alcoholic fatty liver disease-related cardiovascular events: National inpatient sample analysis (2019)
- Cardiac arrest,stony heart,and cardiopulmonary resuscitation: An updated revisit
- Interest of thoracic ultrasound after cardiac surgery or interventional cardiology