
Laparoscopic anatomical liver resection of segment 7 using a sandwich approach to the right hepatic vein (with video)
2024-05-03 09:15:44SongFengYuWeiChenZhangJunYu
Song-Feng Yu,Wei-Chen Zhang,Jun Yu
Department of Hepatobiliary and Pancreatic Surgery, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, China
Full laparoscopic liver resection has been performed widely since it was introduced in the early 1990s.It has been expanded from initial for partial resection of the anterolateral segments to non-restriction of area of the liver [1-3].Anatomical liver resection is considered to have potential superiority than non-anatomic resection in terms of tumor prognosis,thus it is more often recommended in the treatment of hepatocellular carcinoma [4,5].Recently,laparoscopic segmental liver resection according to the Couinaud classification has been widely performed due to its advantages in minimal invasiveness and tumor prognosis.
However,laparoscopic anatomical resection of segment 7(LapAR-S7) remains technically challenging because of the deep location of its anatomical landmarks such as right hepatic vein (RHV)and Glissonean pedicle of segment 7 (G7).Several approaches such as trans-parenchymal approach,Glissonean pedicle first approach and hepatic vein first approach for LapAR-S7 have been described [6-11].Notably,variations of portal and hepatic veins are very common in the liver.It is not rare that S7 may also has partial blood inflow from the right anterior Glissonean pedicle.This kind of variation was unfortunately not suitable for the reported approaches.Here we report a dorso-ventral sandwich approach to the RHV,which may provide a benefit for LapAR-S7 for such patients.
A 47-year-old man was referred to our department in March 2021 because a liver mass was found in his annual medical examination.The patient was asymptomatic and had nothing special in past history.Blood tests showed all normal except for positive hepatitis B surface antigen.HBV-DNA was not detectable.Serum alpha-fetoprotein was 3.1 ng/mL.Contrast computed tomography(CT) scan revealed a 4.3 × 4.0 cm solid mass with typical enhancement indicating diagnosis of hepatocellular carcinoma.The tumor was located in S7 and attached to the main trunk of RHV.After multidisciplinary team consultation,the patient received conventional transarterial chemoembolization (TACE) as initial therapy.One month later the patient was re-admitted for surgery evaluation.Repeated CT scan showed the tumor lacked enhancement but was sedimentated with iodipin.Further 3D reconstruction of liver revealed blood inflow to S7 was not only from G7 but was also from small branches of G8 (Fig.1).Dynamic watershed analysis for S7 revealed that only occlusion of both G7 and branches from G8 going to S7 can cover the whole tumor (Fig.2).
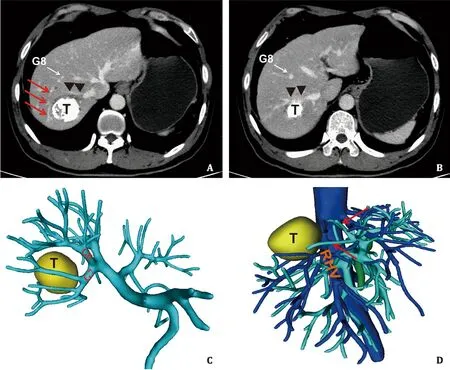
Fig.1. Contrast CT scan and 3D reconstruction of the liver showing the location of tumor and anatomical hepatic structures.A, B: CT showed the tumor was in segment 7 and attached to the RHV (black triangles),lacking enhancement but sedimentated with iodipin;the white arrow indicated G8;the red arrows indicated the branches of G8 going to segment 7.C, D: 3D reconstruction showed partial blood inflow of segment 7 came from G8 (red arrows).T: tumor;G8: Glissonean pedicle segment 8;RHV: right hepatic vein;CT: computed tomography.

Fig.2. Dynamic watershed analysis for segment 7.A: Simulating occlusion of G7 covered only part of the tumor;B: simulating additional occlusion of branches of G8 going to segment 7 covered the whole tumor.G7: Glissonean pedicle segment 7;G8: Glissonean pedicle segment 8.
The patient was placed in a modified left lateral position with the right arm suspended and pelvis and legs maintained in horizontal position.Two 12-mm and two 5-mm trocars were used and placed as shown in Fig.3.One of the 5-mm trocar was inserted through the ninth intercostal space on the right postaxillary line.
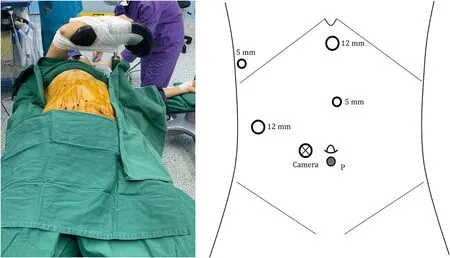
Fig.3. Body position and placement of the trocars.P: tourniquet for Pringle maneuver.
After the right hemiliver was completely mobilized,the hepatoduodenal ligament was encircled with a loop for Pringle maneuver.Intraoperative laparoscopic ultrasound was performed to identify RHV.Its running line,which was on the left side of the tumor,was marked along the lateral posterior surface of the liver.From dorsal side,the root of RHV was first exposed by dividing the short hepatic veins in a caudal-cranial direction along the anterior surface of the inferior vena cava.The caudate process was then divided and the Rouviere groove opened.The caudodorsal liver parenchymal was transected to approach the root of RHV and the posterior Glissonean pedicle.Then G7 was isolated and clamped.The ischemic demarcation line of S7 was marked on liver surface,whereas the S6/S7 boundary line was extended to connect the RHV line,which was secured as the true transection line.After dividing G7,the main trunk of RHV was continuously exposed from root to periphery by transecting the liver parenchymal between the RHV and the demarcation line on the dorsal side.
On ventral side,the superficial tissue was divided along the secured line and deeper transection was performed vertically towards RHV.Once RHV was exposed at the dorso-ventral transection confluence,liver parenchymal was further detached from the main trunk of RHV towards the root direction.The Glissonean branches from G8 were divided when visualized.To avoid the possible tumor dissemination due to the vaporization of ultrasonic device,scissor was used when dissecting RHV where it closely attached to the tumor.Finally,the resection of anatomic S7 containing the tumor with clear surgical margin was successfully achieved(Video S1).
The operative time was 339 min and total blood loss was about 200 mL.There was no intraoperative transfusion.Pathological examination only revealed massive necrotic tissue.No definite tumor cell residues could be found in the resected specimen.The patient was discharged on postoperative day 8 after an uneventful course.He received no adjuvant anticancer therapy but antiviral agents after operation and remained tumor free at 15 months follow-up.
Anatomical hepatectomy requires well recognition and exposure of landmarks such as hepatic veins and Glisonean pedicles during liver transection.According to the Couinaud classification,RHV and G7 are considered as anatomical landmarks for S7.Therefore,approaching to RHV or G7 is a key procedure for LapAR-S7.Lee et al.[9]performed laparoscopic hepatectomy in S7 with an RHV first lateral approach.Parenchymal transection started from the root of RHV and followed along RHV with ligating its small branches.It had limitation for accurate anatomical resection because the segmental pedicle was not clamped in advance.Giuliante et al.[11]reported an ultrasound-guided tans-parenchymal approach to segmental pedicle.They obtained ischemic demarcation of S7 after clamping it,thus seemed more anatomical.Similarly,Ome et al.[8]introduced an intrahepatic Glissonean approach at portal hilum,in which G7 was first approached and divided.The demarcation line of the ischemic S7 area then emerged.Liver transection was completely performed between RHV and the demarcation line only from the dorsal side.However,this approach was not feasible for all patients.In some patients,S7 may also have partial blood inflow from G8.The demarcation area after clamping G7 did not coincide with the actual area of S7,especially on ventral side of the liver.Recently,application of indocyanine green fluorescence staining is popular in liver surgery for many advantages including accurate anatomical hepatectomy [12].Injection to the segment portal vein achieves fluorescence staining for the target segment,but injection to each variant portal branch for target segment is not easy in certain patients.
In the present case,dynamic watershed analysis of S7 by mimicking division of G7 showed that only part of the tumor was involved in the ischemic area.Only occlusion of both G7 and branches from G8 going to S7 could cover the whole tumor.Therefore,we secured the projection line for RHV on liver surface by ultrasound at left-side of the tumor first.By combining of this line and the demarcation line after division of G7,we determined the transection line on the ventral and dorsal side respectively.This approach has benefit in sufficient surgical margin.Particularly,it can avoid possible split damage of the tumor compared to Ome’s approach.In cases of tumor attached to the main trunk of RHV,preoperative TACE makes the tumor necrotic and more solidified.Furthermore,using scissors other than ultrasonic device to detach the tumor may reduce risks of tumor dissemination.Exposure of RHV is another key procedure in our approach.The RHV was exposed in a sandwich approaching manner simultaneously from ventral and dorsal sides.Fully exposure of the RHV can reduce bleeding.Some branches of RHV draining adjacent segment can also be easily preserved.
In conclusion,the dorso-ventral sandwich approach to RHV for LapAR-S7 is safe and feasible,especially providing benefit in selected patients whose blood inflow of S7 is partially from G8.
Acknowledgments
The authors thank Dr.Alexander Bernikov for his contribution in the English audio narration in the video.
CRediT authorship contribution statement
Song-Feng Yu:Conceptualization,Formal analysis,Funding acquisition,Writing -original draft.Wei-Chen Zhang:Investigation,Writing -review &editing.Jun Yu:Conceptualization,Supervision,Writing -review &editing.
Funding
This study was supported by a grant from the Natural Science Foundation of Zhejiang Province (LY20H160023).
Ethical approval
Informed consent was obtained from the patient for publication of this report.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Supplementary materials
Supplementary material associated with this article can be found,in the online version,at doi:1 0.1016/j.hbpd.2022.09.008.
 Hepatobiliary & Pancreatic Diseases International2024年2期
Hepatobiliary & Pancreatic Diseases International2024年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Editors
- Information for Readers
- Meetings and Courses
- Liver transplantation and liver resection as alternative treatments for primary hepatobiliary and secondary liver tumors: Competitors or allies?
- Severe liver injury and clinical characteristics of occupational exposure to 2-amino-5-chloro-N,3-dimethylbenzamide: A case series
- Propensity score matching analysis for clinical impact of braided-type versus laser-cut-type covered self-expandable metal stents for endoscopic ultrasound-guided hepaticogastrostomy