
Safety and effi cacy of omalizumab for antihistamine-resistant chronic urticaria in children: a case series and literature review
2024-04-12 13:02:24WeiFangZhuChenWangJianJunQiaoLanJuanLi
World Journal of Pediatrics 2024年3期
Wei-Fang Zhu ·Chen Wang·Jian-Jun Qiao·Lan-Juan Li
Chronic urticaria (CU) is a common skin disease characterized by the occurrence of wheals,with or without angioedema,lasting more than 6 weeks.The prevalence of CU is about 0.7% [1],but higher in children,with an incidence of 1.38% [1].The occurrence of severe pruritus and unpredictable wheals may severely impact patients’ quality of life,cause psychological problems,including sleep disorders and depression,and lead to economic burden due to limitation on daily life and work [2,3].A standard-dose,second-generation H1-antihistamine (sgAHs) is the f irst-line therapy for patients with CU [4].However,more than one-third of CU patients are insuffi ciently responsive to H1-antihistamines,even with a dosage four times the standard dose (second line;off -label) [4,5].Therefore,add-on treatment should be considered.
Omalizumab is a humanized monoclonal anti-immunoglobulin E (IgE) antibody which is the f irst drug recommended as second-line treatment for CU patients (12 years and above) in the guidelines for treating CU [4,6].It binds to free IgE and lowers free IgE levels to downregulate FcεRI on basophils and mast cells [7].Despite its wide use in children aged 12 years and above who are refractory to H1-antihistamine,there is still doubt on its effi cacy and safety of dosage and relapse in children,especially those younger than 12 years.
This study reported a retrospective case series of pediatric CU patients aged less than 12 years and summarized the published clinical studies to analyze the effi cacy and safety of omalizumab for antihistamine-resistant pediatric CU patients,aiming to provide evidences for treatment pediatric CU patients.
This study was approved by Ethical Committee of the First Affi liated Hospital of Zhejiang University School of Medicine.We retrospectively reviewed all antihistamineresistant pediatric patients with CU under 12 who were admitted to our hospital between January 1,2022 and April 30,2023.All the patients had a diagnosis of chronic urticaria: the occurrence of wheals,with or without angioedema lasting longer than 6 weeks [4,6].Patients with autoinf lammatory diseases and other chronic diseases,in which urticaria may be a symptom,were excluded.
Antihistamine-resistant was defined as the followings: after a sufficient dose of H1-antihistamine treatment (a standard-dose or higher dose of second-generation H1-antihistamine treatment for at least 1 week),the symptoms were still uncontrolled,(wheal and pruritis had no improved).All the antihistamine-resistant children were treated with omalizumab after parental consent was obtained.We extracted all cases information from medical records.
Three antihistamine-resistant children with CU (100%female) aged from 6 to 9 years were included in this analysis.Table 1 shows demographic data,previous treatments and doses of treatments for the patients.The mean serum IgE level was 412.5 IU/mL (range 21.1-1130 IU/mL).Three patients were treated with omalizumab for more than two months at dosages of 150 mg or 300 mg once a month.Disease activity by the urticaria activity score over 7 days(UAS7) were monitored during the treatment.The reaction to omalizumab was def ined as complete (if the results indicated resolution,UAS7=0),partial (symptoms had improved,1 ≤ UAS7 ≤ 15),or no response (treatment failure,UAS7 ≥ 16).All patients achieved a complete response to omalizumab after 8 weeks.One patient had a chest pain after the f irst injection and remitted quickly with no abnormal testing results including electrocardiogram.No other adverse events (AE) were reported during the following treatment for all patients,which conf irmed a good safety prof ile of omalizumab for children.Two children experienced a complete regression of CU for 2-4 months,but the symptoms recurred after COVID-19 infection in December 2022.The other patient who had no COVID-19 infection still remained no recurrence 6 months after the f rist-course treatment,and they still showed a complete reaction to treatment without adverse reactions.Until the recent follow-up,these two recurred patients still had a regression for 2 to 3 months after the second-course treatment.
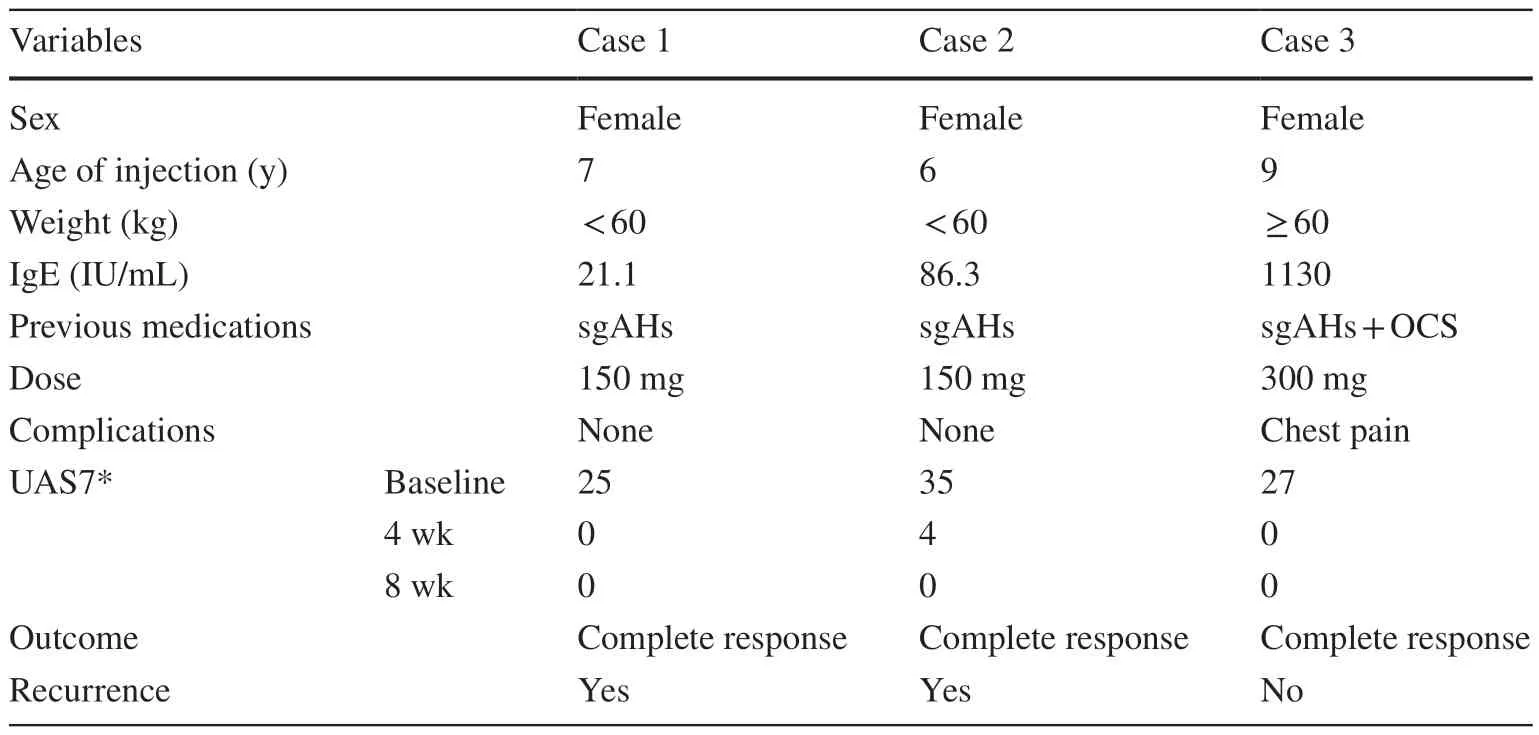
Table 1 Demographic and clinical data and response of patients to treatment included in our case series
Omalizumab is approved only for adolescents > 12 years.The use of omalizumab in children younger than 12 years is still considered off -label.Clinicians still lack experiences in the use of omalizumab in treating antihistamine-resistant CU in children particularly those under 12 years.
Therefore,we performed a literature search for relevant studies of pediatric chronic urticaria in PubMed,Embase,and Web of Science,with the following indexing words:(“children”) or (“pediatric”),(“chronic urticaria”) and(“Omalizumab”).We imposed neither language nor time restrictions.Finally,the database search identif ied 305 studies,and of these,18 articles reporting cases of omalizumab as a treatment for pediatric chronic urticaria fulf illed the inclusion criteria.The presentations,dose,safety,effi cacy and adverse events are summarized in Table 2 [8-25].
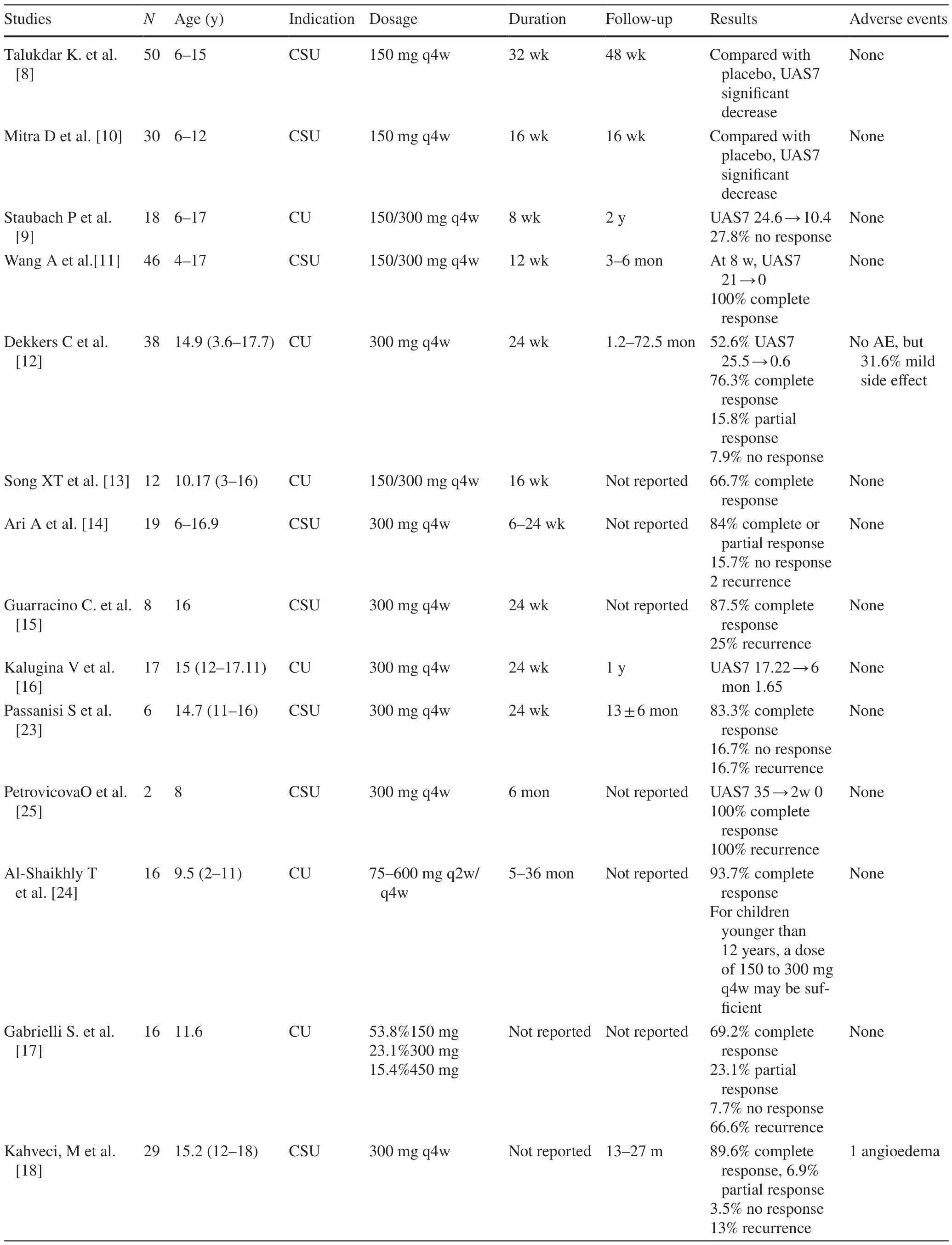
Table 2 A literature review of the studies investigating omalizumab in the treatment of CU
Two independent reviewers used standard templates and performed data extraction to report papers that were in support of or against the treatment of omalizumab for pediatric CU patients.We excluded the articles when the title,abstract,or full text were irrelevant to the investigated issue.Our outcome included adverse events and reaction to omalizumab,which was def ined as complete,partial,or no response.
Overall,345 children aged 2-18 years old with CU who had insuffi cient responses to antihistamines,even at four times the standard dose,were included.The treatment duration ranged from 8 weeks to 36 months,and the follow-up period without medication ranged from 1.2 months to 72.5 months.Results in Table 2 showed the evidence for the use of omalizumab 150 mg or 300 mg every 4 weeks in pediatric patients with CU.Regarding effi cacy,seven studies proved a signif icant decrease in disease activity by the UAS7.More than 80% of patients achieved complete or partial response after omalizumab treatment.The proportion of children showing no response to omalizumab ranged from 3.5 to 11.1%.
Well-controlled disease activity is the most frequent reason for discontinuation of omalizumab [12].Unfortunately,the relapse of CU was common,ranging from 10.9 to 100% after discontinuation.However,the patients still responded well to retreatment with omalizumab [15].The successful response to omalizumab led to a decrease in the use of oral corticosteroids (OCS) and antihistamine drugs while controlling disease activity [26].
In patients older than 12 years,no major adverse events occurred due to the use of omalizumab [27].Our review revealed that adverse events were rare with only sporadic cases of urticaria or angioedema.The events were mostly mild and did not result in discontinuation,which indicated good tolerance in pediatric patients.No major adverse events associated to omalizumab were reported in our review,which suggested that omalizumab could be a secure add-on therapeutic choice for pediatric CU patients.
The standard dosage of 300 mg every 4 weeks recommended in the guidelines for adolescents with CU is still suitable for patients younger than 12 years [4].However,Staubach et al.shared their outcome of the use in CU patients with 150 mg omalizumab every 4 weeks who achieved complete or partial response [21].Talukdar et al.and Mitra et al.attempted more intensive therapy and treated patients at a dose of 150 mg omalizumab every 4 weeks successfully [8,10].Al-Shaikhly et al.suggested that starting treatment for children younger than 12 years with a dose of 150 to 300 mg every 4 weeks may attain eff ective clinical response,and lower doses may be suitable for CU patients under 6 years [24].In our cases,two patients younger than 12 years achieved a complete response at a dose of 150 mg omalizumab every 4 weeks.The clinical response to omalizumab is dose dependent.For children younger than 12 years,multicenter doubleblind randomized controlled trials are required to further investigate the standard dose.
The overall percentage of adverse events was less than 10%.Dekkers et al.described that headache and fatigue were the most frequently reported side eff ects [12].In our case,only one patient reported transient chest pain that remitted quickly.Kahveci et al.and Cekic et al.described that adverse events were rare,with only sporadic cases of urticaria or angioedema [18,19].These events were mostly mild,with no major adverse events,which indicated good tolerance in the children.
Our review has several limitations.Firstly,the number of patients was small in our review.Secondly,the studies were mainly observational studies in our review,including retrospective studies and prospective studies,and were potentially subject to the reporting bias inherent to observation studies and case series.Double-blind randomized controlled trials are rare,suggesting a weakness of evidence.Finally,we reported outcomes on descriptive sentence instead of validated end points because of the heterogeneity of studies.
In conclusion,omalizumab is eff ective and safe in pediatric CU patients who are antihistamine resistant even in children younger than 12 years.A dosage of 150 mg/month should be considered for children,especially those younger than 12 years.
Author contributionsLLJ and ZWF designed the research;WC and ZWF performed the research;QJJ and WC analyzed the data;ZWF and QJJ wrote the paper.
FundingThe study was supported by a grant from Zhejiang Provincial Natural Science Foundation of China (LGF21H190004).
Data availabilityThe datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Conflict of interestThe authors have no conf lict of interest to report.
Ethical approvalThe study protocol was reviewed and approved by the First Affi liated Hospital,Zhejiang University School of Medicine Institutional Review Board.
Informed consentAll study participants,or their legal guardian,provided informed written consent prior to study enrollment.Written consent for publication of the cases’ details together with imaging have been obtained from parent or legal guardians.
 World Journal of Pediatrics2024年3期
World Journal of Pediatrics2024年3期
- World Journal of Pediatrics的其它文章
- Editors
- Information for Readers
- Instructions for Authors
- Diagnosis,treatment and prevention of severe acute respiratory syndrome coronavirus 2 infection in children: experts’ consensus statement updated for the Omicron variant
- Tribute to reviewers (January 1,2023 to December 31,2023)
- Mesenchymal stem cell-based TRAIL delivery inhibits the metastatic state of clinical therapy-resistant progressive neuroblastoma