
Clinical profile of medication-related emergencies among patients presenting to the emergency department: An observational study
2023-12-16 09:14:46SrilathaYagadiRameshBabuGugulothMathewsJacob
Journal of Acute Disease 2023年6期
Srilatha Yagadi, Ramesh Babu Guguloth, Mathews Jacob
1Department of Emergency Medicine, ESIC Medical College, Hyderabad, India
2Department of Emergency Medicine, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India
3Department of Emergency Medicine, Baptist Hospital Bangalore, India
ABSTRACT
KEYWORDS: Adverse drug event; Adverse drug reaction;Nonsteroidal anti-inflammatory drugs; Emergency department;Hospitalization; Patient safety
1.Introduction
From time immemorial human beings have resorted to herbal medications or synthetic preparations, which have been practiced in modern medicine, for the quick and sometimes emergency relief of various diseases.In pharmacology, a drug is a chemical substance of known structure, other than a nutrient of an essential dietary ingredient, and produces a biological effect when administered to a living organism[1].Pharmaceutical drugs may be used for a limited duration, or regularly for chronic disorders[2].
The Emergency Department (ED) physicians usually encounter drug-related emergencies due to drug overdose or adverse drug reactions (ADR).The problem is further complicated by the fact that many patients use multiple drugs due to various comorbidities.
The National Sample Survey Organisation’s report on morbidity for 2004 showed that medicines accounted for 81% of private healthcare expenditure in rural areas and 75% in urban areas.There are 60 000-80 000 estimated brands of drugs available on the market nationally,while the essential drug list in India contains just 348.A significant number of products in the market are either hazardous or irrational and useless[3].A prominent feature of the medicines market in India is that a large proportion of drugs consumed by people are procured through retail sales - an estimated 80%-85% compared to the dominant pattern of institutional sales in developed countries[3].
A drug-related emergency is an acute disorder[4].These emergencies include adverse drug reactions, drug intoxication, drug withdrawal,and drug interactions[3].World Health Organisation defines ADR as“a response to a drug that is noxious and unintended and occurs at doses normally used in man for the prophylaxis, diagnosis or therapy of disease, or for modification of physiological function”[5].Drugrelated adverse reactions can occur in any age group, which may be due to the patient’s noncompliance, interaction with other drugs,inappropriate medication, and inadequate dosing.These reactions if not identified and treated in time can lead to life-threatening emergencies[6].In the United States of America, it has been reported that ADRs due to prescription and over-the-counter drugs during the period 1966 to 1996 affected 6.7% of patients with 3.2% mortality[7].In North India, Singh et al.reported that the prevalence of ADR was 9.3%, which is lower than the global estimate[6].
It has been reported by Shepard et al.that the annual rate of ADRrelated deaths ranged from 0.08/100 000 to 0.12/100 000 and the rate increased significantly over time at a rate of 0.005 8/year in the USA[7].However, on reviewing the literature, we observed that there is not much data available on ADR-related mortality in India.
Apart from ADR, another major public health problem in India is poisoning and drug overdose which occurs either intentionally or accidentally.An overdose happens when the body is overwhelmed by a toxic amount of substance or a combination of substances.Sacak et al.in a study from South India observed that pesticides and prescription medicines were the most common agents causing poisoning[8].
Many studies do not encompass patients who are under the influence of substances and are treated at regional hospitals,primarily because such cases are typically associated with secondary and tertiary-level healthcare facilities.Consequently, research that yields data on these emergency cases in lower-level care hospitals is highly regarded by experts for offering a different perspective on acute poisoning[9-11].
Therefore, this study aims to determine the clinical profile of patients presenting with medication-related emergencies in the Emergency Department and assess the various factors associated with drug-related emergencies.
2.Patients and methods
This observational study was conducted from November 2018 to September 2020 in the tertiary care center and National Accreditation Board for Hospitals & Healthcare Providers-accredited teaching institution.
2.1.Inclusion and exclusion criteria
All the patients who presented to the emergency department were included in the study.Patients with a history of chronic drug abuse but without acute presentation are excluded from the study.
2.2.Data collection
Patients who presented with medication-related emergencies to ED were received according to triage score to respective zones (yellow,red).After stabilization, patients satisfied with inclusion criteria were included in the study and written informed consent was taken from patients or companions.
The severity of ADR is assessed based on the Hurwitz severity assessment scale of ADR[11].GCS at the time of presentation,source of medication were noted.The severity of ADR, type of drug overdose, requirement of advanced airway and vasopressors, and the outcome were also assessed.
2.3.Statistical analysis
IBM SPSS Statistics for Windows, version 22.0 (IBM Corp.,Armonk, NY, USA) was used.Data were presented as median and interquartile range (IQR) for quantitative variables, and frequencies and percentages (%) for qualitative variables.Chi-square test was used to analyze categorical variables, with a significance level set at P<0.05.
3.Results
A total of 138 patients were included, including 97 patients with adverse drug reaction and 41 with drug overdose.
ADR was the most common type of medication-related emergency,comprising 70.3% of the patients (97/138), while drug overdose accounted for 29.7% (n=41).Based on Naranjo Grading of ADR,there were 19 (19.6%) definite cases, 2 (2.1%) possible cases, and 76(78.4%) probable cases.Three cases were mild in the ADR group,81 cases were moderate, and 13 cases were severe.
One-third of the ADR occurred in the elderly above 60 years; while most patients with drug overdose were 21-40 years old (Table 1).The majority of ADRs were seen in females (56.7%) as compared to males (43.3%).And 87.8% in the drug overdose group were females.Most patients were hemodynamically stable and did not require vasopressors, or advanced airway in both two groups (Table 2).Most patients had GCS ranging from 13-15 in both two groups (Table 3).
Nonsteroidal anti-inflammatory drugs (NSAIDs) were the most used medicine in the drug overdose group (17/41, 41.5%), followed by antihistamines (13/41, 31.7%); while in the ADR group, antidiabetic medication was the most used medicine(34/97, 35.1%)followed by NSAIDs (22/97, 22.7%) (Table 4).Most medications were prescribed in the ADR group (93/97, 95.9%) followed by overthe-counter drug (OTC) (4.1%), while in the drug overdose group,most medications were OTC (25/41, 61.0%), followed by prescribed(14/41, 34.1%).The difference was significant (χ2=63.2, df=2,P<0.001).
Most patients in the ADR group were admitted to a ward (41/97,42.3%), and 39 (40.2%) patients were discharged.While in the drug overdose group, 82.9% of patients were admitted to ICU.The difference was significant (χ2=69.5, df=3, P<0.001) (Table 5).

Table 1.Age distribution (n, %).
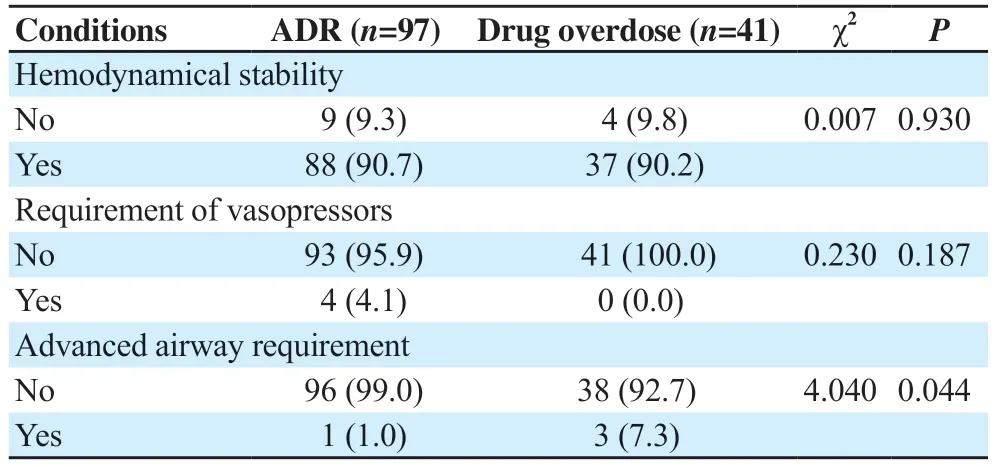
Table 2.Condition of patients at emergency room (n, %).

Table 3.GCS score.

Table 4.Use of medication (n, %).

Table 5.Outcome of patients (n, %).
4.Discussion
Medication-related emergencies are quite common and the effect is quite underestimated.Relative studies are still lacking and our study was conducted to investigate the clinical profile of patients with medication-related emergencies at a tertiary care hospital in South India.
Among all cases (n=138) in our study, ADR contributed to 70.3%(n=97), and drug overdose accounted for 29.7% (n=41).This is similar to a study by Laatikainen et al., which revealed much higher incidence of ADRs as (23.1%)[12].
In our study, we observed that ADR-related emergencies were more common in the 21-40 years (34%) and above 60 years (33%) groups.Younger patients are more prone to have antibiotics and NSAIDs,whereas, diabetes is common in those above 60 years with a higher need for anti-diabetic agents.This is in contrast to a study done by Schurig et al.in Germany, which reported median age as 74.5 years[13].In our study, most patients with drug overdose were 21-40 years old.Various reasons such as dysfunctional careers, marital abuse, and drug addiction contribute to drug overdose in the younger age group[14].
Our study revealed that the majority of ADRs were seen in females(56.7%) as compared to males (43.3%).The underlying reason can be explained by the difference in pharmacokinetics between males and females[15].This was similar to studies by Schurig et al.[13] and Girgin et al.[16].In India, incidence of suicides from poisoning is higher in males[14].We observed that 87.8% of the drug overdose group were females, which is in agreement with a study done by Z?hre et al.[17].
The majority (90%) of patients in both ADR and drug overdose groups were hemodynamically stable and 4% of the ADR group required vasopressors in our study.Advanced airway placement was required for 7.3% of the drug overdose group.Only a juvenile diabetic patient in the ADR group required advanced airway, who presented with hypoglycemia-induced status epilepticus.
We observed that the majority of our patients (80.4% in the ADR group and 92.7% in drug overdose group) had a GCS of ≥13.The low GCS seen in the remaining 7.8% was due to hypoglycemia and drug overdoses with central nervous system drugs (benzodiazepine and antiepileptics).
In our study, anti-diabetic medications (35%) (including insulin and oral antidiabetic agents) were the most common medications associated with ADR-related visits to the emergency, followed by NSAIDs.This was comparable to a study done by Dammalapati et al., which reported that hypoglycaemic agents and cerebral vasospasm drugs were the most common drugs associated with ADR-related visits[18].Jiang et al.found that NSAIDs were the second most common cause of ADR among patients admitted to intensive care[19].With regard to drug overdose, NSAIDs (41.5%)and antihistamines (31.7%) were the most common followed by benzodiazepines (24.4%).This was similar to a Turkish study done by Z?hre et al., which reported that antidepressants, analgesics,and psychotropic drugs were the most common class of medication associated with medication overdose[17].
According to the WHO causality assessment scale, 65% of reactions were categorized as “probable,” with the remaining 35% labeled as “possible.” Naranjo’s algorithm indicated 65.6% as “probable”and 34.4% as “possible.” The Modified Hartwig and Siegel scale identified 41.4% of reactions as “moderate level 4(a)” severity,while 30.6% were considered “mild level 1.” Approximately 30.8%of ADRs were deemed “definitely preventable” according to the modified Schumock and Thornton scale[20].Definite ADR could be attributed to anti-diabetic agents, chemotherapy, and anti-tuberculous drugs.Most of the other studies did not use the Naranjo algorithm for the ADR probability assessment.
In our study, 41.2% of patients in the ADR group were discharged from the emergency department, 42.3% were admitted to wards and 13.4% were admitted to the intensive care unit.This can be explained by the fact that the majority of ADRs in our study were due to antidiabetic medication and required intravenous dextrose infusion and dose adjustment of antidiabetic medication.Girgin et al.found that 35% of patients were admitted to ICU[16] and Schurig et al.observed that 11% of patients were treated on outpatient department basis[13].Among the drug overdose group, 82.9% were admitted to intensive care units and only 2.4% were discharged from the emergency department.This is in contrast to a study done by Zohre et al.[17] with 21% (out of 509) ICU admissions.
Most medications were prescribed in the ADR group (93/97,95.9%) followed by OTC (4.1%), while in the drug overdose group,most medications were OTC (25/41, 61.0%), followed by prescribed(14/41, 34.1%).The underlying disorders included depression,mood, anxiety, and epileptic disorders.Similar findings were shown in the study done by Sánchez-Sánchez et al.[21].Among the subjects,78.9% had a history of or were currently using over-the-counter(OTC) medications.The prevalence of OTC drug usage decreased with increasing age, with only 36.4% of individuals aged 71 or older using OTC drugs.Notably, analgesics were the most commonly consumed OTC drugs (49.1%), particularly among women, young adults with non-formal education, and individuals with low to medium socioeconomic status living in urban areas.It is imperative to implement measures aimed at promoting the safe use of OTC drugs to prevent potential adverse events resulting from inadequate knowledge regarding their usage.This can be explained by the fact that OTC drugs are more easily available in India compared to other countries.This finding stresses the need for stricter countrywide legislation to regulate the practice of issuing OTC drugs.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Data availability statement
The data supporting the findings of this study are available from the corresponding authors upon request.
Authors’ contributions
SY: conceptualization, formal analysis, resources, methodology;RBG: validation, formal analysis, writing-review; MJ: writing original draft, data curation, methodology, resources.
 Journal of Acute Disease2023年6期
Journal of Acute Disease2023年6期
- Journal of Acute Disease的其它文章
- Epidemiological characteristics and trends of animal bites in Neyshabur,Iran: A cross-sectional study
- COVID-19 mortality trends before and after the national vaccination program in Iran: A joinpoint regression analysis
- A public health perspective on dengue in Bangladesh in the twenty-first century
- Imipenem/cilastatin-induced acute eosinophilic pneumonia: A case report
- Neurological manifestations of COVID-19 infection: A case series
- Risk factors for development of pneumothorax in patients with COVID-19 at a government health facility in North India: An exploratory case-control study