
Right hepatectomy with a cholangiojejunostomy and hepaticojejunostomy for unilobar Caroli’s syndrome
2023-10-30 10:36:24DumindSusingheSivsuriySivgnesh
Dumind Susinghe ,,,Sivsuriy Sivgnesh ,
a Division of HPB Surgery, Department of Surgery, Faculty of Medicine, University of Colombo, Colombo, 0 080 0, Sri Lanka
b The University Surgical Unit, The National Hospital of Sri Lanka, Colombo, 0 080 0, Sri Lanka
Choledochal cysts are benign cystic dilatations of the extra- and intrahepatic bile ducts [ 1,2 ]. If untreated,their sequelae include recurrent cholangitis,secondary biliary cirrhosis,acute pancreatitis,and cholangiocarcinoma [ 3,4 ]. Todani et al. [5] classified choledochal cysts into 5 subtypes,of which type V is Caroli’s disease.The disease is either localized,where unilobar biliary dilatation,commonly in the left,is present,or diffuse,where the entire liver is involved. The surgical treatment of Caroli’s disease depends on the pattern of duct involvement and involves hemi-hepatectomy and liver transplantation. A partial hepatectomy is the best curative option in unilobar disease,providing long-term survival,free of symptoms and complications [4] . Caroli’s syndrome is defined as Caroli’s disease with congenital hepatic fibrosis [6] . Herein,we describe a patient with unilobar Caroli’s syndrome treated for septic complications,who subsequently had a right hepatectomy and complex bilioenteric anastomosis.
A 43-year-old female patient presented with clinical and biochemical features of acute cholangitis and elevated inflammatory markers. There was a history of cholangitic episodes which were managed with antibiotics at a local hospital over the preceding year. Contrast computed tomography (CT) abdomen showed a dilated common bile duct (CBD) with two calculi,dilated intrahepatic ducts,and early liver parenchymal disease with left lobar hypertrophy and central dot sign ( Fig. 1 A and 1 B). Her pancreas was normal,and no varices were noted. The acute cholangitis was managed with intravenous antibiotics,endoscopic sphincterotomy and stone extraction. Despite transient improvement,she became septic again and was diagnosed with segment VII liver abscess ( Fig. 1 C and 1 D). This was resolved after a prolonged period of percutaneous drainage ( Fig. 1 E) and antibiotic therapy for carbapenem sensitive coliforms grown from the pus. Magnetic resonance imaging (MRI) confirmed Caroli’s disease showing cystic dilatation of intrahepatic ducts predominantly in the right lobe,especially in segment VII ( Fig. 1 F),hepatolithiasis and a CBD diameter of 18 mm. The kidneys were normal. In view of the recurrent cholangitis complicated by abscess formation and potential long-term sequelae,she was prepared for surgery after the control of sepsis. Her clinical parameters and liver biochemistry indicated Child-Pugh A(score 5) with no evidence of portal hypertension and her renal functions were normal. She had a right hepatectomy with extrahepatic bile duct resection and a cholecystectomy. At surgery,the hepatic transection plane passed through a large cystic cavity in segment IV ( Fig. 2 A) that contained calculi. An extended right hepatic resection was avoided to preserve as much liver parenchyma as possible since the left liver though hypertrophied,showed features of early parenchymal disease ( Fig. 2 ). The residual wall of the cavity at the cut surface of the liver contained multiple openings communicating with the left intrahepatic bile duct system ( Fig. 2 B and 2 C). Reconstruction was done using a Roux-en-Y loop with a 20-cm long enterotomy anastomosed to the margins of the cavity creating a cholangiojejunostomy ( Fig. 2 D). An end-to-side left hepaticojejunostomy was performed downstream to the first anastomosis ( Fig. 3 ). Both anastomoses were done using interrupted 5-0 polydioxanone. In view of the previous carbapenem sensitive coliform isolated from the hepatic cyst,she was given imipenem intravenously for 5 days after surgery. Histopathology revealed large,cystic dilatations of intrahepatic and extrahepatic bile ducts compatible with Caroli’s disease and evidence of congenital hepatic fibrosis with cholestasis confirming Caroli’s syndrome. There was no evidence of cholangiocarcinoma. After an uneventful postoperative recovery,she remained clinically well with a normal CT abdomen and carbohydrate antigen 19-9 (CA19-9) level three years after surgery.
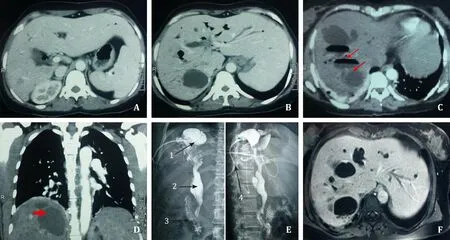
Fig. 1. Cross sectional imaging and percutaneous transhepatic cholangiography (PTC). A,B : Contrast CT abdomen showing Caroli’s disease involving right lobe and left lobular hypertrophy. C: MRI liver depicting Caroli’s disease with right lobe involvement. D,E: CT liver showing multiple fluid levels in biliary cavity suggestive of intrahepatic abscess formation. E: PTC and cholangiogram showing rest of the ectatic extrahepatic biliary tree (1: cystic enlargement of intrahepatic ducts; 2: ectatic extra hepatic bile ducts; 3:contrast in duodenum; 4: PTC catheter). F : MRI liver showing cystic dilatation of intrahepatic ducts. CT: computed tomography; MRI: magnetic resonance imaging.
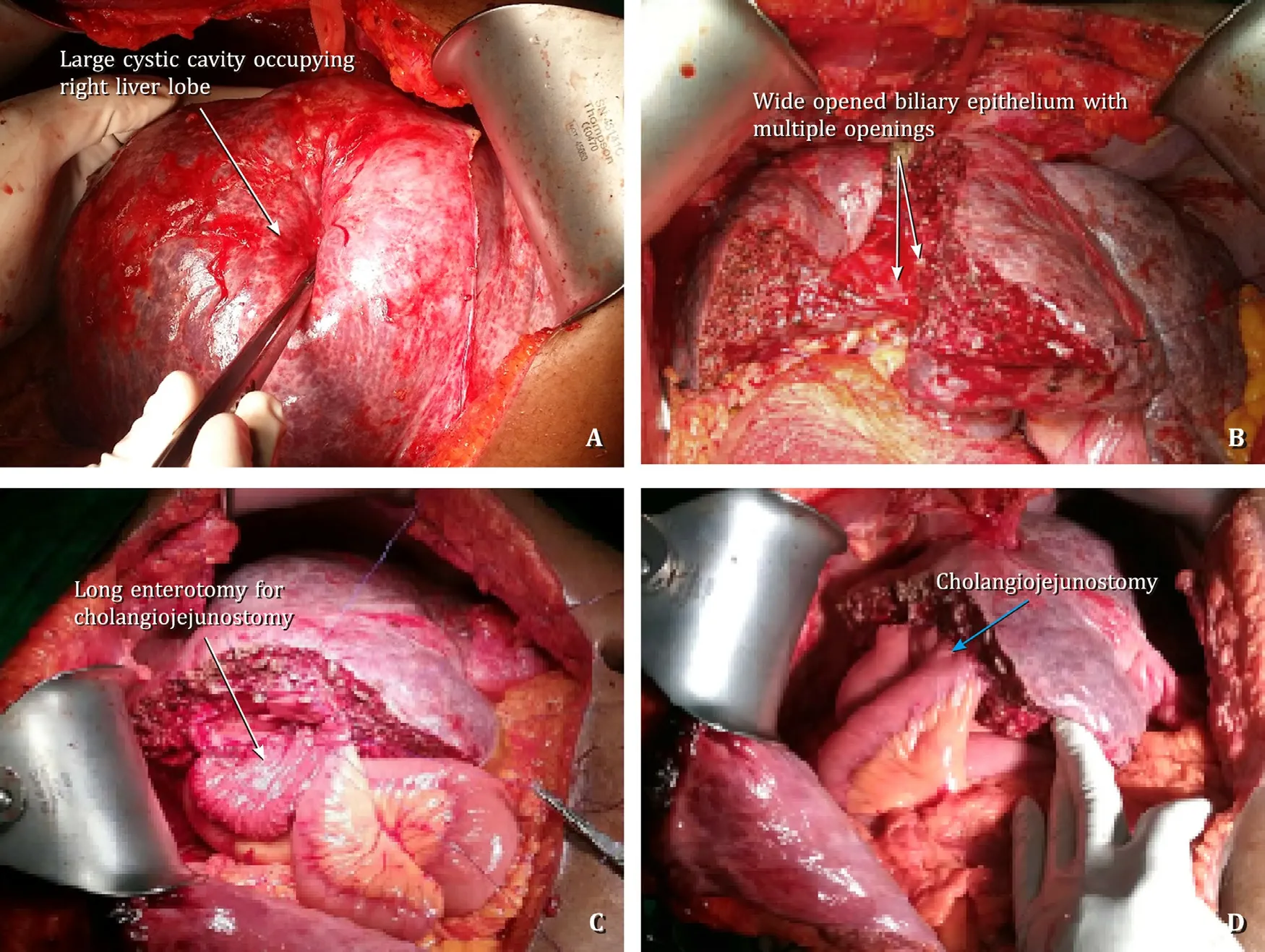
Fig. 2. Intraoperative images. A: Large cystic cavity involving right lobe of the liver. B: Cut surface of remnant left lobe with widely opened biliary epithelium. C: Intraoperative step of cholangiojejunostomy with 20-cm long enterotomy of jejunum. D: Cholangiojejunostomy and hepaticojejunostomy after establishment of bilioenteric anastomosis.
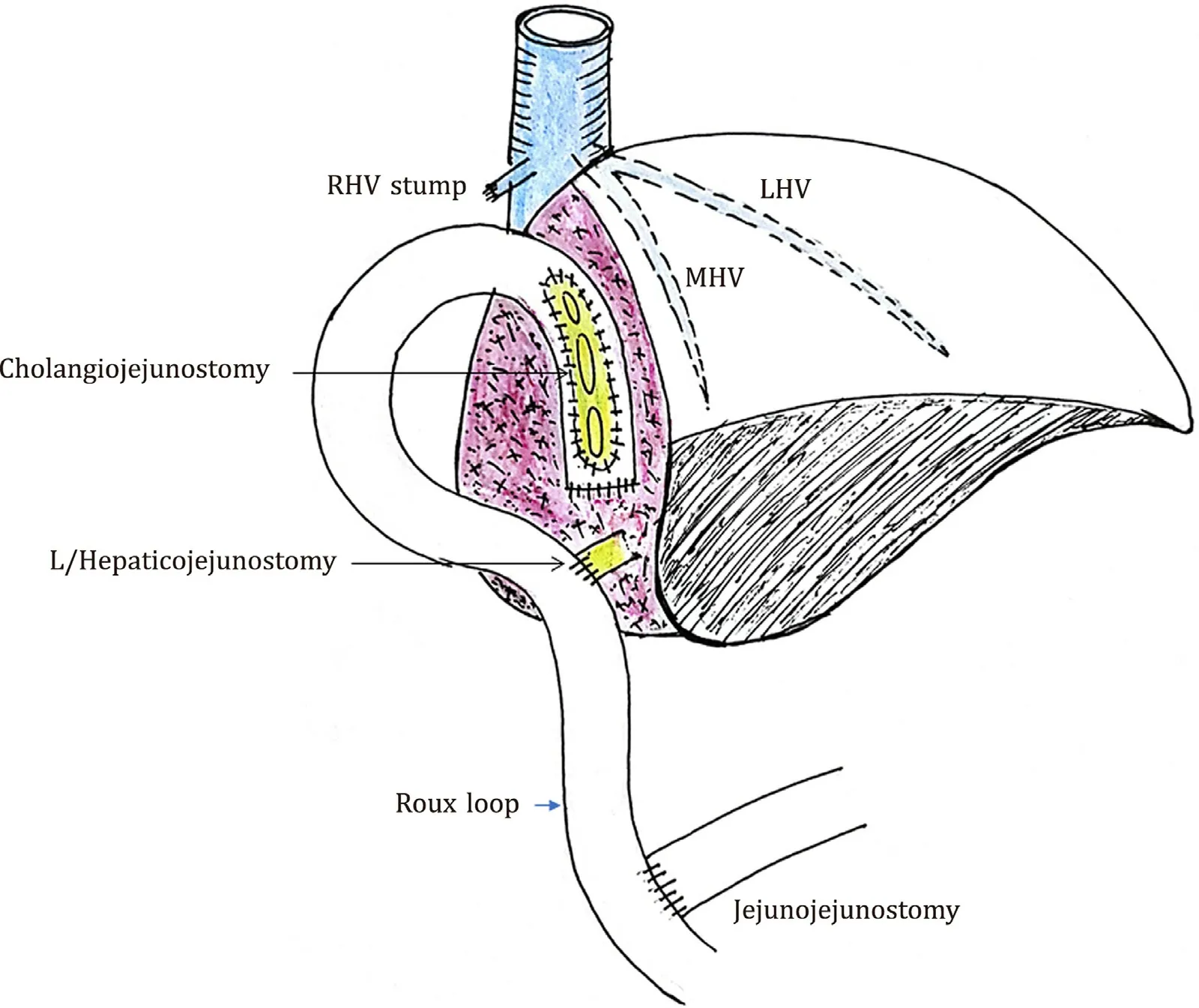
Fig. 3. Diagram of cholangiojejunostomy and hepaticojejunostomy procedure performed. RHV: right hepatic vein; MHV: middle hepatic vein; LHV: left hepatic vein.
Caroli’s syndrome is an autosomal recessive multi-cystic dilatation of intrahepatic bile ducts with congenital hepatic fibrosis associated with adult polycystic kidney disease [6] . In addition to the characteristics of recurrent cholangitis and hepatolithiasis in Caroli’s disease,Caroli’s syndrome progresses to portal hypertension.This usually occurs late in the course of the disease as manifested in our patient who had no features of portal hypertension though histology revealed congenital hepatic fibrosis.
Hemihepatectomy with or without a bilioenteric anastomosis remains the treatment of choice in unilobar Caroli’s disease in the absence of cirrhosis. Bilioenteric anastomoses following major resections usually involve the extrahepatic bile ducts,i.e.,the common hepatic,the left or right hepatic ducts. Anastomoses to the intrahepatic bile ducts or cholangiojejunostomies are uncommon and have largely been described in the context of the Longmire procedure for inoperable hilar cholangiocarcinomas [7–9] where following a left lobectomy,the intrahepatic ducts of segments II and III on the cut surface of the liver are anastomosed to a Roux-en-Y jejunal loop. Only one case of cholangiojejunostomy has been described after hepatectomy for Caroli’s disease [10] . Like other bilioenteric anastomoses,cholangiojejunostomies are susceptible to early bile leaks and late anastomotic strictures. The incidence of complications specific to this reconstruction is not known because of the negligible reports available but the rates of hepaticojejunostomies after hilar cholangiocarcinoma resections may provide references [ 9,11,12 ]. However,due to the wide anastomosis of the cholangiojejunostomy in this case,we believe that the likelihood of stricture formation and obstruction is low.
The large segment IV cyst required us to decide between an extended right hepatectomy and left hepaticojejunostomy or a right hepatectomy with an additional intrahepatic cholangiojejunostomy.We opted for the latter. The decision was influenced by the macroscopic appearance of early parenchymal liver disease and multiple openings into the cyst,and of ducts communicating to the left hepatic duct (LHD) system. This enabled hepatic parenchyma sparing and inclusion of all LHD communications within a single anastomosis,in addition to the main left hepaticojejunostomy,potentially minimizing the risk of bile leaks from the cut surface.
This case illustrates a safe and novel surgical strategy employed to manage a patient with unilobar Caroli’s syndrome,enabling safe and effective drainage with hepatic parenchyma sparing.
Acknowledgments
The authors acknowledge all ward staff who took care of our patient.
CRediT authorship contribution statement
DumindaSubasinghe:Conceptualization,Investigation,Visualization,Writing - original draft,Writing - review & editing.
SivasuriyaSivaganesh:Investigation,Writing - review & editing.
Funding
None.
Ethical approval
The consent was obtained from the patient for publication of this report.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2023年5期
Hepatobiliary & Pancreatic Diseases International2023年5期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Total three-dimensional laparoscopic radical resection for Bismuth type IV hilar cholangiocarcinoma
- A surgical technique using the gastroepiploic vein for portal inflow restoration in living donor liver transplantation in a patient with diffuse portomesenteric thrombosis
- Full laparoscopic anatomical liver segment VII resection with preferred Glissonean pedicle and dorsal hepatic approach
- Combined hepatic segment color rendering technique improves the outcome of anatomical hepatectomy in patients with hepatocellular carcinoma
- Targeting mitochondrial transcription factor A sensitizes pancreatic cancer cell to gemcitabine
- Pathogen detection in patients with perihilar cholangiocarcinoma:Implications for targeted perioperative antibiotic therapy