
The first experience of multi-gripper robot assisted percutaneous coronary intervention in complex coronary lesions
2023-09-24 06:12:22PanLILiangZHANGBoLIWeiPoCHENWeiShengCHENZhiFuGUOBiLiZHANG
Journal of Geriatric Cardiology 2023年8期
Pan LI ,Liang ZHANG ,Bo LI ,Wei-Po CHEN ,Wei-Sheng CHEN ,Zhi-Fu GUO,? ,Bi-Li ZHANG,?
1.Department of Cardiology,Changhai Hospital,Naval Medical University,Shanghai,China;2.Department of Cardiology,Shanghai 411 Hospital,China RongTong Medical Healthcare Group Co.Ltd.,Shanghai,China
With advances in the field of interventional cardiology,percutaneous coronary intervention (PCI) has become one of the main treatment methods for patients with coronary artery disease in clinical practice.[1]Routine interventional therapy is performed under fluoroscopic guidance,and interventional cardiologists are therefore often exposed to radiation.As a result,the risks of cancer,cataract,hair loss and loss of skin pigmentation will be significantly increased after long-term radiation exposure.[2-4]In addition,some measures to protect patients and operators from radiation exposure,such as lead clothes,bibs,and hats,were associated with elevated cervical and lumbar complications.
To solve the problems related to PCI,a variety of endovascular interventional robots have emerged in recent years.The well-known robot-assisted system for PCI,the CorPath GRX Robotic System (Corindus Inc,a Seimens Healthineers Company,Waltham,Massachusetts,USA),has been approved by the United States Food and Drug Administration and certified by the European Union Conformite Europeenne.[5]The CorPath GRX system is suitable for interventional therapy including coronary artery and peripheral blood vessels,which can significantly reduce the radiation exposure of interventional doctors and improving the accuracy of interventional manipulation.[6]However,the existing robotic-assisted systems have a common problem in that they cannot complete the entire endovascular procedure,such as rotating catheter and implanting the stent.Our research team has developed a novel universal endovascular interventional robot system (ALLVAS,Oppen,Shanghai,China).[7]The robot assisted PCI system consists of a master surgeon console and a robotic platform with four manipulators (Figure 1) that enables the operator to advance,retract and rotate guidewires,catheters,balloons,and stents,and complete the crossing action.Nevertheless,the utility of this robotic system in the interventional treatment of coronary lesions remains unknown.Herein,we report a case of a 65-year-old man with left main and three-vessel coronary artery disease who underwent successfully robotically assisted PCI.The case has been approved by the Ethics Committee at Changhai Hospital,Naval Medical University,Shanghai,China (CHEC-2021-166) and conducted in accordance with the principles established in the Declaration of Helsinki.
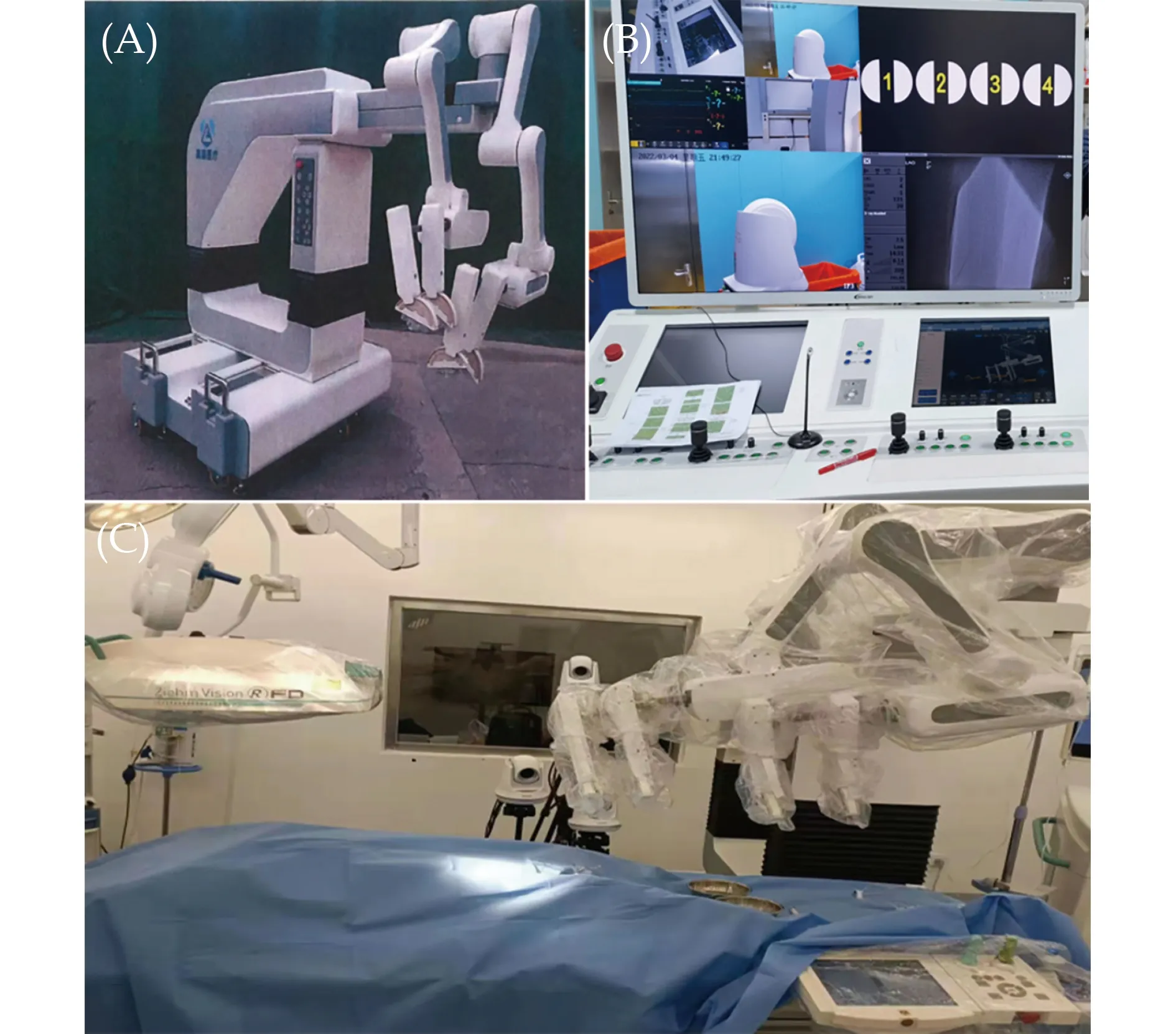
Figure 1 Robotic percutaneous coronary intervention platform.(A): The ALLVAS system with four manipulators;(B): robot control platform;and (C): overview of the ALLVAS system in the catheterization laboratory.
A 65-year-old man was admitted to our institution with a three-year history of chest pain.There were no accompanying symptoms such as palpitation,abdominal pain and dizziness.Physical examination revealed that the pulse was 76 beat/min,body temperature was 36.3 °C,and the measured blood pressure was 120/70 mmHg at resting conditions.His height was 172 cm,and weight was 70 kg.No additional heart sound or significant heart murmur was heard over the chest wall.The patient’s risk factors and past history included active tobacco use,hypertension for ten years,and diabetes mellitus for ten years and treatment with insulin.The patients had a history of PCI to the three-vessel disease,five years ago.He took aspirin and atorvastatin for a long time.Moreover,laboratory tests were unremarkable.Electrocardiography revealed sinus rhythm with mild ST-T changes.No significant abnormalities were found following chest Xray examination.Transthoracic echocardiography demonstrated left atrial enlargement with the left ventricular ejection fraction of 54%.
The patient was admitted to the Department of Cardiology to undergo coronary angiography and he signed an informed consent form before the procedure.The robot-assisted procedure is under our close observation and monitoring.If any risks present during the procedure,manual operation is undertaken immediately.The procedure was started by constructing the vascular access with a 6F sheath (Terumo) manually inserted into the right radial artery.Heparin (100 IU/kg) was given intravenously to maintain the activated clotting time between 250 s and 350 s.A 0.035 guidewire (Terumo) with a 5F TIG catheter (Outlook) was subsequently introduced (Figure 2A),and a 6F sheath was held by the first manipulator.The catheter and guidewire were controlled separately by the second and third manipulators,respectively.The guidewire was then withdrawn,and selective angiography was performed.Coronary angiography showed 50% localized stenosis at the end of the left main coronary artery,80% diffuse stenosis in the near-middle segment of the left anterior descending artery (LAD),70% diffuse stenosis in the proximal left circumflex artery (LCX),no obvious stenosis in the original proximal stent of the right coronary artery and 40%-50% stenosis in the distal part of the stent (Figure 2B).Intravascular ultrasound(Boston Scientific) was performed manually by the assistant operator and showed that the minimum lumen area of the LAD at the stenosis was 2.61 mm2,and the plaque burden was 76% (Figure 2C);the minimum lumen area of the LCX at the stenosis was 2.3 mm2,and the plaque burden was 85% (Figure 2D).After the measurement,the J-shape guidewire was reintroduced,and the 5F TIG catheter (Outlook) was withdrawn.A 6F EBU guiding catheter (Medtronic) was inserted into the 6F sheath along the guidewire and was held by the first manipulator.Then,Runthrough (TERUMO) and SION guidewires (Asahi)were introduced successively into the distal segment of LAD and LCX along the guiding catheter under the cooperation of the second and third manipulators.Then,the operating physician manually installed the pre-expanded balloon (2.5 mm × 15 mm,Emerge monorail) into the end of the guidewire.To provide the support and fixation of the whole PCI system,the guiding catheter was fixed by the first manipulator and the three-way screw plug was clamped via the second manipulator.Meanwhile,the distal part of the guidewire and balloon was clamped and fixed through the third manipulator and the fourth manipulator,respectively.After that,the fourth manipulator pushed the balloon or stent to the lesion along the guidewire.Finally,the operating physician expanded and released the balloon.The pre-expanded balloon was withdrawn and exchanged for a drug-eluting stent (2.5 mm × 18 mm,Firebird2) (Figure 2E).Following this,the high-pressure balloon (2.5 mm × 15 mm,Euphora) was exchanged for post expansion.The procedure for stent implantation of the LAD proximal segment(4.0 mm × 15 mm,Resolute) was also performed with a robot system in a similar manner (Figure 2F).After removal of the delivery system,final angiography and repeat intravascular ultrasound was performed to assess the efficacy of stent implantation and the procedure related complications were excluded.
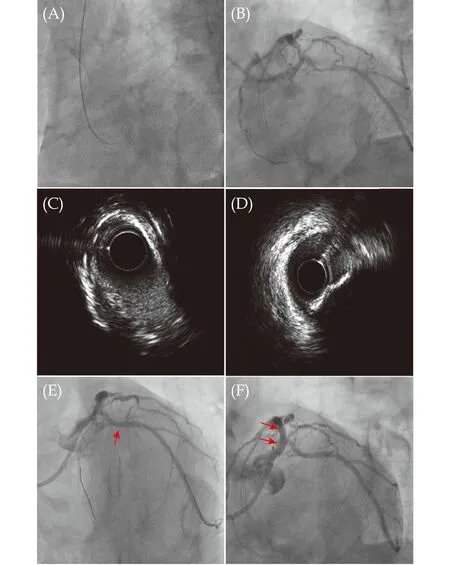
Figure 2 Robotic-assisted percutaneous coronary intervention for the LAD lesion and LCX lesion. (A): Insert J-shape guidewire and TIG catheter under robot control;(B): placement of an EBU guided catheter and a guidewire into the distal end of the lesion;(C &D): intravascular ultrasound images of the LAD and LCX lesions;(E): a 2.5 mm × 18 mm Firebird2 stent (red arrow) was delivered robotically and implanted in the LCX lesion;and (F): a 4.0 mm × 15 mm Resolute stent (red arrows) was delivered robotically and implanted in the LAD lesion.LAD: left anterior descending artery;LCX: left circumflex artery.
The patient took long-term aspirin orally and he received a loading dose of 180 mg of ticagrelor 24 h before the operation.After operation,the patient received maintenance dose of 100 mg,once a day of aspirin and 90 mg,twice a day of ticagrelor.The patient received 100 mg/d aspirin,90 mg/d ticagrelor,and 20 mg/d atorvastatin orally after PCI.The patient had an uneventful hospitalization and was discharged home on postoperative day 7.During the three-month follow-up,the patient did not experience chest discomfort.
Despite the advance of robot technology and equipment,there are still limitations in design and technique.For example,most commercialized robotic systems can only participate in part of the PCI procedure,and many process still requires manual operation.In contrast,the novel robot system in the present study can participate in the whole PCI process.To our knowledge,this study is the first to demonstrate the safety and feasibility of the multigripper robot assisted PCI in a patient with complex coronary anatomy.
Compared with the robots currently available for clinical use,the main difference is the novel robotic system accomplished multiple collaborative manipulations with twelve degrees of freedom though four robotic manipulators.[7]In this study,the novel robotic system can accomplish complex actions in multivessel coronary lesions,such as insertion,withdrawal and rotation of the guidewire,balloon and stent.With the help of the novel robot system,interventional doctors can remotely control most PCI procedures and only need to manually complete the puncture,sheath placement and catheter exchange,thereby reducing the risk of complications related to radiation exposure.
The entry to exit time of the procedure was from 08:45 to 11:35,March 2022.In this case,the total X-ray exposure dose was 2202.32 mGy using the robot assisted PCI system,which was slightly higher than our previous similar manual PCI (2146.21 ± 268.89 mGy).The learning curve issues associated with a new technology may contribute to the high exposure dose and we firmly believe that the radiation exposure dose will be significantly reduced with the continued use of the device.Additionally,there was a significant 20 mL reduction in the use of contrast volume in the present case (210 mL) when compared to previous similar manual PCI (231 ± 45 mL).The postoperative angiography showed that the position of the stent was accurate without any stent or PCI-related complications.In addition,this robot system cannot assist in intervening the chronic total occlusion of the coronary artery.More complications of robot assisted PCI,such as coronary dissection,need to be fully evaluated in more cases.Although robot systems may be more important for simple angioplasty in remote areas,robot operations have not been widely popularized due to the lack of sufficient experience and the ability to deal with intraoperative emergencies.
Multi-gripper robot-assisted endovascular treatment may have a wider application scope and greater advantages than current interventional robots.The reported case yielded encouraging results and provided experience and a basis for future research on more robot-assisted interventional therapies.In future work,we will focus on and explore the force feedback and three-dimensional navigation mechanism.
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No.81870356 &No.82170275),and the Shanghai Rising-Star Program (20QA1409000).All authors had no conflicts of interest to disclose.
 Journal of Geriatric Cardiology2023年8期
Journal of Geriatric Cardiology2023年8期
- Journal of Geriatric Cardiology的其它文章
- Prolonging dual antiplatelet therapy improves the long-term prognosis in patients with diabetes mellitus undergoing complex percutaneous coronary intervention
- Development and validation of a score predicting mortality for older patients with mitral regurgitation
- Age-related outcomes in patients with cardiogenic shock stratified by etiology
- Prognostic value of hematological parameters in older adult patients with acute coronary syndrome undergoing coronary intervention: a single centre prospective study
- Transcatheter aortic valve implantation in a patient with anomalous right coronary artery originating from the left aortic sinus with interarterial course
- Feasibility of emergent transcatheter aortic valve replacement sequentially followed by cardiac computed tomography angiography: experience from the procedure