
Open surgical approach for two coincidental splenic artery aneurysms: a case report
2023-09-19 12:59:12WeirongZhengSenLi
Weirong Zheng ,Sen Li
1 Department of Vascular Surgery, the First People's Hospital of Wenling, Wenling 317500, China
2 Department of Vascular Surgery, the Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou 310009, China
Several factors can contribute to the formation of aneurysms,including hemodynamic changes,polyarteritis nodosa,bacterial endocarditis,vasculitis,fibromuscular dysplasia,vascular malformation,and cystic medial necrosis.[1,2]Surgery is recommended for splenic artery aneurysms (SAAs) greater than 25 mm in diameter,and several surgical approaches are used,including open surgery,laparoscopic surgery,and percutaneous embolization.Laparoscopic surgery might be associated with an increased risk of pancreatic leakage compared to the open surgery approach.Open surgery without complete aneurysm resection should be preferred for patients with large SAAs in close contact with the pancreas.Here,we report a patient with two splenic artery aneurysms.
CASE
A 70-year-old male patient,a native resident of Hangzhou,was admitted to the emergency department with acute abdominal pain.He had a three-year history of hypertension that was treated with valsartan.During physical examination,a large pulsatile mass in the left upper abdomen and mild abdominal tenderness in the left abdomen were noted.Laboratory tests,including routine blood examination,electrolytes,amylase,liver function tests,X-rays,and electrocardiogram,were normal.However,computed tomography angiography (CTA) revealed a rare anatomical variation of the splenic artery arising from the hepatic artery.Additionally,one SAA measuring 74 mm in diameter in the proximal splenic artery and another SAA measuring 27 mm in diameter in the middle of the hepatic artery were found(Figure 1A).Both SAAs were saccular without calcifications or thrombosis.
Considering the risk of rupture and the irregularity and narrowness of the vessel structure,open surgery was chosen.Median laparotomy was performed,and large pulsating masses were observed in the abdomen (supplementary Figure 1).After careful consideration,the SAAs were ligated at the proximal and distal ends.The SAAs were very large,and the splenic artery ran to the left along the superior margin of the pancreas;therefore,separating the SAAs from the surrounding tissues was associated with a high risk of pancreatic damage and bleeding.The dissection of the SAAs revealed blood f low from several branch arteries into the aneurysm sac.The branch arteries were ligated with 5-0 prolene sutures from the inside of the aneurysm walls,and human fibrin sealant was applied to occlude the aneurysms.However,the vascular supply of the entire spleen was compromised,and the spleen turned black 30 min after the completion of the procedure while the patient was under observation.Ischemic necrosis of the spleen was considered,and splenectomy was performed,followed by closure of the laparotomy incision.
Pathologic examination revealed mucoid degeneration and hyalinization of the arterial wall of the aneurysm(supplementary Figure 2).The patient recovered without postoperative complications.Blood tests one week after surgery revealed a platelet count of 480×109/L,and 100 mg/d aspirin was initiated.At the 1-year follow-up evaluation,the patient was in good clinical condition.CTA showed that both SAAs were occluded with no blood f low,and the aneurysms had shrunk (Figure 1B).
DISCUSSION
Splenic artery aneurysms with a diameter of ≥5 cm are considered rare,whereas two coincidental SAAs are rarer,potentially life-threatening presentations.SAAs can cause jaundice,abdominal pain,portal hypertension,or hemorrhage,depending on the location of the aneurysm.[3]Surgery is recommended for SAAs larger than 25 mm in diameter,those with symptomatic SAAs,[4]and those with rapid growth due to the increased rupture risk,which is associated with 20%-30%mortality.[5]Except in cases of rupture,the diagnosis of SAA is difficult due to the nonspecific symptoms.
Moreover,patients may benef it from treatment regardless of the sac size for aneurysms in specific arterial territories.In the present case,the treatment strategy was based on the site and the morphologic and anatomic characteristics of the SAAs as well as the need for occlusion of large efferent vessels emerging from the aneurysms.In addition,clinical presentation,general health status,and comorbidities were considered to determine the treatment approach.
Treatment approaches for this disease are classic surgical approaches,[6]including aneurysmal resection with or without vascular reconstruction,laparoscopy,[7]and endovascular treatment such as percutaneous embolization or stent implantation.[8]A previous study reported an endovascular approach with coil embolization for the treatment of huge hepatic artery aneurysms.[9]Coil embolization of large SAAs with a very wide neck tends to be extremely troublesome due to the limited length of inflow and outflow arteries.[10]Moreover,embolization of large aneurysms is associated with increased cost.In large saccular aneurysms,coil embolization is associated with poor long-term prognosis,as the coils may not be stable,increasing the risk of displacement and migration.Locating SAAs,separating the surrounding tissue,and dissecting the aneurysm are timeconsuming procedures associated with an increased risk of postoperative complications,such as pancreatic leakage.Therefore,in the present case,open surgery was performed to ligate the distal and proximal ends of the aneurysms,which were occluded using human fibrin sealant to reduce the risk of pancreatic leakage and bleeding.During the long evolution of SAAs,multiple collaterals may develop,which can increase the splenic blood supply.In fact,the development of splenic ischemia following dissection and ligation of the SAAs in the present case required eventual removal of the spleen.For that patient,a laparoscopic approach may be minimally invasive.However,the present patient had two large SAAs,which were far apart,and the laparoscopic approach had difficulty in achieving precise manipulation and may cause a high risk of pancreatic injury.D’Errico et al[11]reported a patient with symptomatic double SAAs in the proximal and distal sections of the splenic artery who was successfully treated with surgery.Median laparotomy could provide a better view and more precise manipulation.
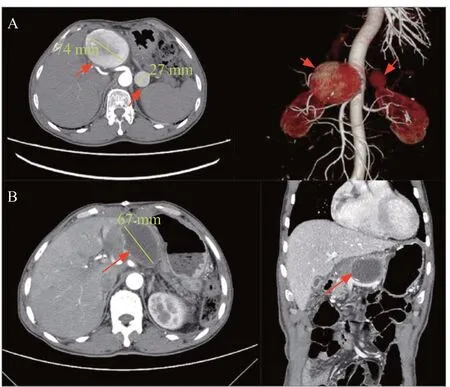
Figure 1.Results of computed tomographic angiography.A: two separate splenic artery aneurysms,measuring 74 mm and 27 mm in diameter,anomalously originating from the hepatic artery;B: the splenic aneurysm was completely occluded with no blood inf low at the 1-year follow-up.
CONCLUSION
In patients with large SAAs in close contact with the pancreas,open surgery without complete aneurysm resection could be preferred to minimize pancreatic complications.
Funding:This study was funded by the Natural Science Foundation of Zhejiang Province (LQ20H020006).
Ethical approval:The patient provided informed consent,and all procedures performed followed the ethical standards of our hospital.
Conf licts of interest:The authors declare that they have no competing interests.
Contributors:All authors contributed substantially to the writing and revision of this manuscript and approved its contents.
All the supplementary files in this paper are available at http://wjem.com.cn.
 World journal of emergency medicine2023年5期
World journal of emergency medicine2023年5期
- World journal of emergency medicine的其它文章
- Acute hemolytic anemia in a 34-year-old man after inhalation of a volatile nitrite “popper” product
- Severe disseminated intravascular coagulation complicated by acute renal failure during pregnancy
- Key elements and checklist of shared decisionmaking conversation on life-sustaining treatment in emergency: a multispecialty study from China
- Establishment and evaluation of animal models of sepsis-associated encephalopathy
- Progressive eschar-like wound and peripheral neurological dysfunction with severe inf lammatory status: infection or unnatural immune response?
- Inferior vena cava thrombosis in two adult patients with veno-arterial extracorporeal membrane oxygenation