
Disseminated tuberculosis presenting as meningitis and spondylodiscitis in an immunocompetent adult
2023-07-14 08:16:46JeyapraniyaArumugamShamilaDeSilva
Jeyapraniya Arumugam, Shamila De Silva
1University Medical Unit, Colombo North Teaching Hospital, Ragama, Sri Lanka
2Faculty of Medicine, University of Kelaniya, Sri Lanka
ABSTRACT Rationale: Disseminated tuberculosis involves the central nervous system in up to a third of cases.However, meningitis and spondylodiscitis due to miliary tuberculosis rarely occur together,particularly in the immuno-competent population.
KEYWORDS: Disseminated tuberculosis; Immunocompetent;Spondylodiscitis; Meningitis; Miliary tuberculosis
1.Introduction
Disseminated tuberculosis (TB) is a rare form of TB characterized by lymphatic and hematogenous spread of Mycobacterium tuberculosis bacilli[1].Despite the availability of effective therapy, diagnosis is usually late and mortality remains high[2].Disseminated tuberculosis is rare in immunocompetent adults[3].Extra-pulmonary sites of infection commonly include the gastrointestinal tract, lymph nodes,pleura, bone and joints[4].Extra-pulmonary TB classically does not show typical clinical symptoms.Therefore, it can be misdiagnosed,causing a delay in treatment, and adversely affecting the prognosis.Written informed consent for patient information and images to be published were provided by the patient.
2.Case presentation
A 37-year-old previously healthy male presented with altered level of consciousness for one week with a preceding history of lower back pain and evening pyrexia for one month.He also complained of loss of appetite, night sweats and a five-kilogram weight loss during this period.He had difficulty in walking for one week and his relatives noticed paucity of left upper and lower limb movements.He had a contact history of TB ten years ago.On examination, the patient was cachectic but afebrile, not dyspneic, and hemodynamically stable with clear lungs.There was neck stiffness with Glasgow coma scale(GCS) 8/15 (M-5, V-1, E-2).The gaze was deviated to the left.Limb examination revealed minimal left upper and lower limb movements with hypotonia.Reflexes were reduced in the left upper limb.He had increased tone, exaggerated reflexes, and clonus in bilateral lower limbs.A sensory level could not be assessed due to reduced GCS.As the patient had spastic paraplegia with left hemiparesis, a disseminated infection such as TB, a fungal infection with spinal cord compression or a disseminated malignancy were suspected.
Investigations revealed neutrophilic leukocytosis with elevated erythrocyte sedimentation rate (77 mm/first hour) and C-reactive protein (27 mg/L).Chest radiograph revealed miliary mottling.Thoracolumbar spine radiographs showed fusion of thoracic vertebrae.Contrast CT brain revealed leptomeningeal enhancement suggestive of meningitis and hypodense areas suggestive of infarction involving the right basal ganglia, thalamus, internal capsule and left internal capsule.The first lumbar puncture revealed cerebral spinal fluid (CSF) protein of 222 mg/dL and CSF sugar to blood sugar ratio of 0.24 but there were no cells.CSF for TB PCR was negative.Repeat lumbar puncture on day 14 revealed 150 cells with lymphocytic predominance and high protein of 288 mg/ dL.High resolution computed tomography chest revealed military TB with spinal involvement.Magnetic resonance imaging (MRI)of brain revealed multiple cerebral infarctions, likely to be due to TB cerebritis (Figure 1A).MRI cervicothoracic spine revealed TB spondylodiscitis at T10/T11 level with paravertebral abscess formation (Figures 1B and 1C).Ultrasound-guided abscess drainage was unsuccessful as the amount of fluid present was not aspirable.However, soft tissue thickening was noted at T10/T11 level vertebrae,and a biopsy was taken for histological assessment.Histology revealed granulomatous lesions with central caseating necrosis suggestive of TB.Work up for a cause of immunosuppression was negative.
Anti-TB treatment was started together with a tapering regimen of dexamethasone.The patient showed good clinical response to the anti-TB treatment with improvement of GCS to 14/15 and settling of fever.
3.Discussion
TB frequently presents with non-specific constitutional symptoms and systemic manifestations, requiring a high index of suspicion to establish the diagnosis.Infections such as brucellosis and disseminated malignancy may mimic TB.However, our patient had multiple symptoms suggestive of TB, typical miliary mottling in the chest radiograph, negative CSF and blood cultures for organisms and typical histological features highly suggestive of TB.
Disseminated TB is defined as concurrent involvement of at least two non-contiguous organ sites of the body, or involvement of the blood or bone marrow by the tuberculous process[5].Here, we describe central nervous system (CNS) and vertebral involvement in a patient with miliary TB.The patient presented with hemiparesis and spastic paraparesis.Instances where disseminated TB presents with status epilepticus, otitis media, altered consciousness and chronic back pain have been reported, but spastic paraparesis with hemiplegia has so far not been reported to occur concurrently[1-3,6].The young adult reported here had no comorbidities but developed disseminated TB.This case emphasizes the importance of considering disseminated TB in the differential diagnose even in those of younger age, when symptoms are suggestive.
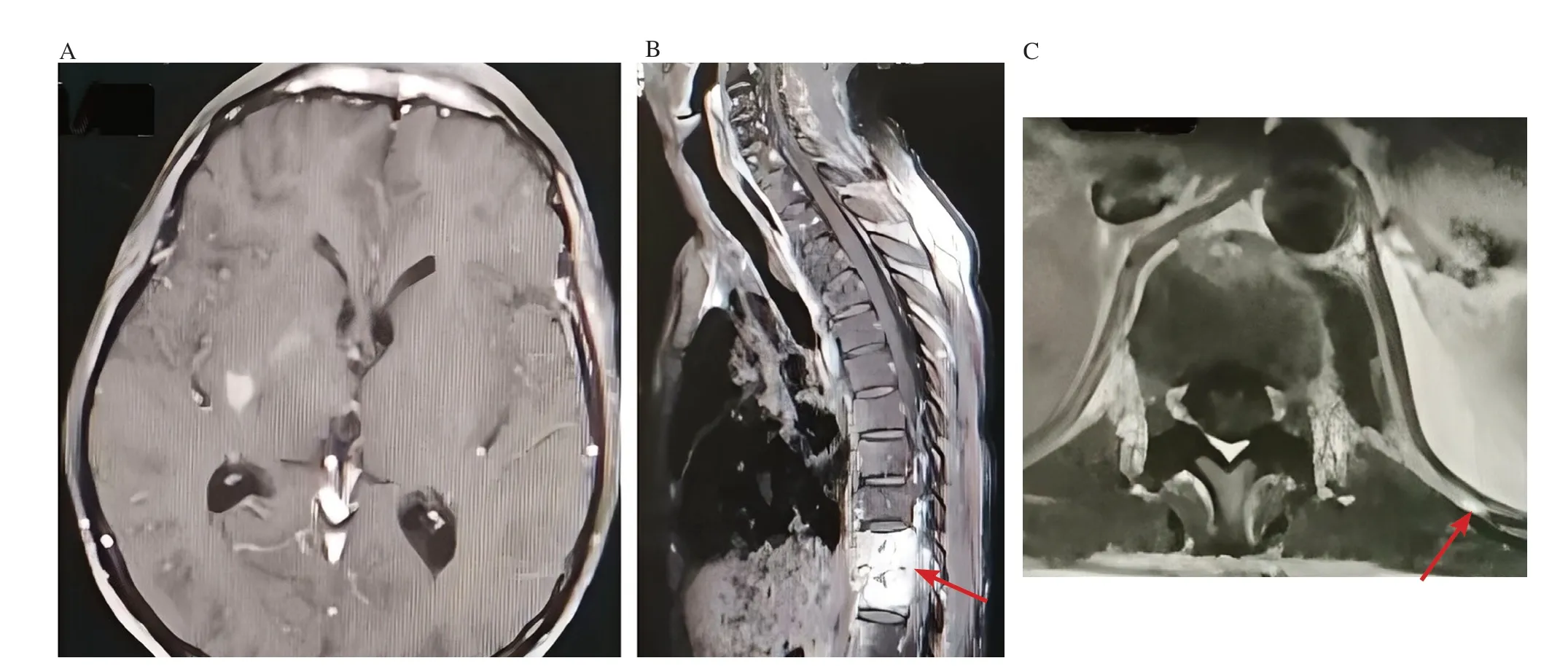
Figure 1.MRI brain and MRI spine.A 37-year-old immunocompetent male presented with altered level of consciousness for one week and lower back pain with evening pyrexia for one month.A: MRI brain-mild leptomeningeal enhancement.T1W low, T2W/FLAIR high signal intensity areas seen in right basal ganglia and right thalamus.B and C: T10/T11 space narrowing with destruction of adjacent vertebral end plates, abnormal signal intensities in T10/T11 vertebral bodies extending into posterior elements (red arrow in B) and contrast fluid collection in left paravertebral space (red arrow in C).
The patient had none of the risk factors for TB such as HIV,diabetes, smoking, alcohol abuse, or chronic liver and kidney disease.Previous studies have reported disseminated TB in immunocompetent persons who had one or more of these risk factors[1,2,6].Certain genetic defects also predispose immunocompetent individuals to develop disseminated TB.These include production or metabolism of interferon-gamma and interleukin-12.Tests for these immunoregulators are not widely available but these can be helpful in screening families and counseling them[2].
Cerebrospinal fluid examination is the best diagnostic test for tuberculous meningitis.CSF typically shows elevated protein and lowered glucose concentrations with prominent lymphocytosis[7].Our patient had no cells in the initial CSF analysis but had a high protein level with a low glucose level suggestive of TB.The absence of cells may be because this CSF sample was obtained quite early in the disease course.TB PCR has a sensitivity of 50% and specificity close to 100%[8].However, our patient had a negative TB PCR,which is also likely to be due to the timing of CSF sample collection in relation to disease course.
We were unable to confirm the diagnosis microbiologically.As clinical suspicion was high, we went ahead with further imaging followed by histological assessment to confirm the diagnosis.MRI spine typically showed paravertebral collection which was highly suggestive of TB and unlikely to be caused by malignancy.A disease can be confirmed when a patient responds to the specific treatment of that disease.Our patient improved tremendously with the initiation of anti-TB treatment.In general, antimicrobial therapy for disseminated TB is the same as for pulmonary infection.But modifications may be warranted in drug-resistant TB and a longer duration of therapy may be needed when organism burden is high,clinical response is slow, and when there is immune suppression,CNS infection or bone and joint involvement[6].Adjunctive systemic glucocorticoid therapy is recommended for treatment of TB involving the CNS and pericardium, but data is limited and based on a few case reports[6].
In conclusion, we believe this is a unique case of disseminated TB involving three different organs in a patient presenting with both spastic paraparesis and hemiparesis, a phenomenon previously not reported in an immunocompetent patient.As TB is endemic in many developing countries it should be suspected widely.Diagnosis of disseminated TB is not straightforward as patients may not present with typical clinical features.
Conflict of interest statement
The authors declared no potential conflicts of interest with respec
t to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research,authorship, and publication of this article.
Authors’contributions
AJ did literature survey, extracted information from patient records and wrote the case report.SDS did literature survey, organized,supervised, and edited the manuscript
 Asian Pacific Journal of Tropical Medicine2023年6期
Asian Pacific Journal of Tropical Medicine2023年6期
- Asian Pacific Journal of Tropical Medicine的其它文章
- R21 vaccine: A ray of hope for malaria elimination
- One Health practice in Hainan, China
- Chryseobacterium/Elizabethkingia species infections in children
- Association between the extent of public health measures and other respiratory infectious diseases cases amidst the COVID-19 pandemic in Thailand
- Magnetic resonance imaging evaluation of head and neck involvement in IgG4-related disease
- Excess mortality in Northeast Iran caused by COVID-19: Neglect of offset community transformations of health