
Atypical pompholyx presentation of secondary Staphyloccoccus and Klebsiella infections in a patient with premorbid Ebstein anomaly: A case report
2023-02-19 08:25:56HartantyoKusumaDwiyantiPuspitasariDominicusHusadaLenyKartinaParwatiSetionoBasukiIsmoedijanto
Hartantyo Kusuma, Dwiyanti Puspitasari, Dominicus Husada, Leny Kartina, Parwati Setiono Basuki, Ismoedijanto
Department of Child Health, Faculty of Medicine, Airlangga University, Dr. Soetomo Hospital Surabaya, Surabaya, Indonesia
ABSTRACT
KEYWORDS: Pompholyx; Ebstein anomaly; Klebsiella;
1. Introduction
Pompholyx or dyshidrotic eczema, also known as dyshidrotic dermatitis, is characterized by pruritic, tense, deep-seated vesicles mainly on the palms and lateral surfaces of the fingers[1]. The prevalence of hand dermatitis varies from 2% to 8.9% of the general population. Although dyshidrotic eczema occurs worldwide, it is less common among Asians. The peak age of onset is between 20 and 30 years, which is unusual in children[2].
Most cases are sporadic yet the exact etiology is not known. In severe conditions, a secondary bacterial infection of pompholyx with Staphylococcus or Streptococcus is common and results in pain,swelling, and pustules on the hands and feet[3]. This case reported an atypical presentation of pompholyx accompanied by Staphylococcus and Klebsiella infection in a child with cyanotic heart disease(Ebstein anomaly).
2. Patient’s consent
Informed consent was obtained from the patient for the publication of this case report and any accompanying images. The patient’s parents also gave consent for publication, as the patient is only 15 years old.
3. Case report

Figure 1. A 15-year-old girl with progressive wound and small bumps containing yellowish pus and crusts on her hands (A) and feet (B) and improvement of skin in hands (C) and feed (D) after treatment.
A 15-year-old girl came to the dermatology outpatient clinic of Dr.Soetomo Hospital, Surabaya, Indonesia, with a chief complaint of a progressive wound and small bumps containing pus on her feet and hands that initially appeared 6 months before admission (Figure 1A and 1B). It worsened during the last month, with itching and pain in the area with erosions. The patient’s mother reported that the wound initially manifested as a small papule which was subsequently filled with clear liquid and pus. It emerged as red patches on the foot with itchy and responded well to the application of an ointment. At the first visit, there was no complaint of fever, nausea, vomiting,diarrhea, or shortness of breath. However, she didn’t routinely come for follow-ups at the outpatient clinic; nor did she comply with the long-term skincare by regularly applying wet compresses as advised. According to her mother, the child was reluctant to this treatment regimen because the lesions were painful when touched.The complaint recurred monthly, and lesions contained clear liquid and sometimes pus. During the latest recurrence the condition worsened, the child experienced a fever and was unable to walk and decided to see a pediatrician. Despite having been treated with 250 mg erythromycin 3 times a day for 7 days, sodium fusidate cream, and wet dressing with normal saline 4-6 times a day, the complaint did not improve. On the day of admission, the lesions were more extended, covered with blackish yellow crusts, pus,looked dirty, on and off along with a pain or itchy, meanwhile, the child appeared weak and cyanotic. Noteworthy, the patient had a congenital heart disease, namely Ebstein anomaly and moderate secundum atrial septal defect, where the diagnosis was established at the age of 9 years. Accordingly, propranolol and spironolactone were prescribed and she routinely visited the pediatric cardiology outpatient clinic for follow-up. Cyanosis had been observed since infancy, along with poor weight gain and shortness of breath, which worsened on moderate to hard exertion.
None of the family members suffered from the same skin condition, history of prior skin disease, or contact with patient confirmed with COVID-19. There was neither evidence of traveling to areas or communities that have been affected by COVID-19 nor certain drug consumption.
4. Examination and treatment
The patient looked fatigued and dyspneic, was alert with GCS 456, blood pressure 100/70 mmHg (90-120/70-80), heart rate 112 bpm (80-100 bpm), respiration rate 30 tpm (12-20 tpm),temperature 36.9 ℃ (36.5-37.5 ℃), SpO2: 68-80% (>94%), no anemia or jaundice, but her lips were cyanotic. No chest retractions,no rales, or wheezing were noticed, there was a loud holosystolic murmur (grade 5) at the left parasternal line Ⅳ, and no significant findings of the abdominal and neurological examination were evident. The skin lesions involved her arms and legs: dorsum and palmar region right and left arm, digitiⅠ-Ⅴleft arm, digitiⅠ-Ⅱ right arm: multiple erythematous macules, sharply marginated with thick blackish-yellow crust, multiple papules and pustules in some areas, eschar (+). At dorsum and plantar right and left legs:multiple hyperpigmented macules, un sharply marginated with thick blackish-yellow crust, multiple papules and pustules in some areas,eschar (+). Her body weight was 23 kg and her height 145 cm. Both her weight and height for age was <P3 on CDC growth chart, with the ideal body weight of 37 kg, indicating a condition of severe malnutrition. And she did not menarche yet.
Her laboratory test revealed Hb 16.5 g/dL (12-16 g/dL), leucocytes 6 250/mm3(4 000-10 000/mm3), thrombocyte 283.000/mL (150-400×103/mL), eosinophils 3% (0-6%), neutrophil 70.2% (40%-70%), lymphocyte 23.3% (20%-50%), neutrophil lymphocyte ratio 3.01 (>3.5), serum glucose 112 mg/dL (70-140 mg/dL), aspartate aminotransferase 26 U/L (12-38 U/L), alanine aminotransferase 12 U/L (7-41 U/L), albumin 2.5 g/dL (3.5-5.5 g/dL), blood urea nitrogen 15 mg/dL (7-20 mg/dL), creatinine 0.4 mg/dL (0.6-1.2 mg/dL), Sodium 134 mEq/L (136-146 mEq/L), potassium 4.1 mEq/L(3.5-5.0 mEq/L), chloride 107 mEq/L (96-106 mEq/L). COVID-19 antibody rapid test was not reactive. Urinalysis revealed normal.The pus culture revealed Staphylococcus aureus, and Klebsiella aerogenes sensitive with amikacin, gentamycin, piperacillin,piperacillin tazobactam, oxacillin, ceftazidime, cefotaxime,ceftriaxone, cefoperazone-sulbactam, cotrimoxazole, tetracycline,chloramphenicol, moxifloxacin and meropenem. The chest radiograph showed cardiomegaly with a cardiothoracic ratio of 67%(Figure 2).
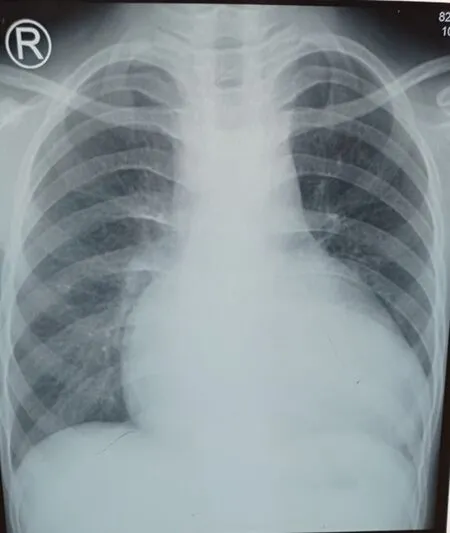
Figure 2. Chest radiography in Ebstein anomaly shows cardiomegaly with a cardiothoracic ratio of 67%.
Echocardiography revealed Ebstein anomaly, moderate secundum Atrial Septal Defect bidirectional shunt with a right to left shunt dominant, mild mitral regurgitation, and mild tricuspid regurgitation.
A comprehensive multidisciplinary management regimen was applied. Wound care consisted of wet dressing with normal saline on crust/erosion and moisturizing with cod liver oil ointment and natural hydrocolloid gel. Cloxacillin 250 mg every 6 hours and paracetamol 250 mg every 8 hours orally were prescribed. For the cardiac symptoms, the patient routinely consumed spironolactone 25 mg once daily and propranolol 5 mg every 8 hours orally. Additional nutrition with high-caloric milk (Nutrini) was provided by giving 200 mL every 8 hours. Culture of the pus yielded Staphylococcus aureus and Klebsiella aerogenes which indicated a secondary infection, and accordingly, Chloramphenicol 500 mg every 12 hours was added for 14 days. The skin lesions gradually improved, sloughed off, and dried, and after 10 days of hospitalization shortness of breath was unremarkable, she gained 1 kilogram of weight and the skin lesions were completely healed (Figure 1C and 1D).
5. Discussion
Pompholyx or dyshidrotic eczema is currently defined as dermatitis which is characterized by symmetrical non-erythematous pruritic vesicles or bullae that mainly affect the palms and lateral surfaces of fingers. The current and more accurate terminology for this condition is recurrent vesicular palmoplantar dermatitis (RVPD). The eruption may also occur on the soles of the feet, but in approximately 80% of cases, only hands are affected. In a clinical profile by Guimaraes et al., children and adolescents with RVPD aged 3 to 16 years, with an overall average of 8.4 years. The earliest onset case was 5 months old and the latest was 15 years[4].
The etiology of RVPD remains obscure. Factors that may predispose to the development of RVPD in a susceptible individual include atopy, contact allergens, contact irritants, infection of dermatophyte, allergy to ingested metal (in particular, nickel and cobalt), hyperhidrosis, prolonged use of protective gloves,intravenous immunoglobulin treatment, psychological stress,and smoking[4,5]. In our patient, there was no history of wearing protective gloves, consumption of suspicious food, smoking, or getting an Intravenous Immunoglobulin treatment. The most likely pompholyx inducer of our patient was hyperhidrosis which may have been related to her congenital heart disease (Ebstein anomaly).This disorder is a rare congenital malformation of the heart that is characterized by displacement of the septal and posterior tricuspid valve leaflets, atrialization of the right ventricle, and variable degrees of malformation and displacement of the anterior leaflet. Cyanosis,fatigue, palpitations, and dyspnea can be observed[6]. Hyperhidrosis in congenital heart disease occurs when the conditions develop into heart failure. Blanche et al. reported that excessive sweating(hyperhidrosis) is compensation to dissipate heat from the body,which increases in heart failure patients because of the increasing activity of the sympathetic nervous system[7]. In our patient, the atypical pompholyx is characterized by multiple hyperpigmented macules, unsharply marginated with blackish-yellow crust, multiple papules and pustules in some areas, and eschar on her legs and arms.The disease was associated with Staphylococcus aureus and Klebsiella aerogenes infection and responded well to the antibiotic given based on a sensitivity test.
The hallmark infection of Staphylococcus aureus skin and soft tissue infection (SSTI) is the cutaneous abscess, but other manifestations of skin infection are also found clinically. Non-purulent cellulitis may be also caused by Staphylococcus aureus Staphylococcus aureus cellulitis most commonly involves the lower extremities, but may also involve other regions, such as the upper extremities, abdominal wall, and face[8].
For complicated skin and soft tissue infections, a number of registrational trials have compared different antimicrobial agents by the Infectious Disease Society of America. For methycillin-resistant Staphylococcus aureus, the Infectious Disease Society of America recommends vancomycin, linezolid, daptomycin, telavancin,or ceftaroline for patients hospitalized with a severe purulent SSTI. In the case of a nonpurulent SSTI, beta-lactam antibiotic is recommended for mild or moderate infection, whereas vancomycin is recommended as part of empirical therapy for severe nonpurulent SSTI[8].
Chloramphenicol is effective against most Gram-positive(including most strains of MRSA) and Gram-negative bacteria including anaerobes like Klebsiella aerogenes. However, during the year 1970 to 1990, clinicians have become reluctant to use this drug because of potential side effects and resistance[9].
The patient improved after a comprehensive treatment regimen consisting of topical medication for the skin (corticosteroid),systemic drugs to manage secondary infections, and disturbance of the heart, along with additional nutrition to get optimal outcomes[10]. After 10 days of hospitalization, the skin lesions gradually improved, sloughed off, and dried, and her shortness of breath was unremarkable, she also gained weight by 1 kilogram and she was discharged uneventfully.
Diagnosing and identifying the etiology of atypical pompholyx with secondary infection requires detailed history taking and clinical examination. A comprehensive management approach of the patient’s skin, infection, nutrition, and premorbid can reduce prolonged hospitalization, and promote early recovery of patients.Cyanotic congenital heart disease may contribute to the occurrence of pompholyx by providing a state of hyperhidrosis, and as a result, decreased blood flow may hinder the delivery of oxygen and nutrition needed for proper wound healing. Evaluation of infection and nutritional problems was conducted to get the optimal outcome[10].
Conflict of interest statement
The authors declare that they have no conflict of interest.
Authors’ contributions
HK and DP examined, worked up the case, and drafted the manuscript. DH, LK and PSB conceived the idea, reviewed the literature and revised the manuscript. Is. supervised the case and finalized the draft.
 Asian Pacific Journal of Tropical Medicine2023年1期
Asian Pacific Journal of Tropical Medicine2023年1期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Time to stimulate Plasmodium vivax research in India: A way forwards
- Novel markers in predicting Brucella sacroiliitis: The platelet large cell ratio and basal immature reticulocyte fraction
- Sociodemographic and clinical characteristics of SARS-CoV-2 infected population during the second and third epidemiological waves in Sri Lanka
- Knowledge and associated factors of healthcare workers on measles vaccine and cold chain management at health institutions in Gondar, Ethiopia
- Modelling the probability of presence of Aedes aegypti and Aedes albopictus in Iran until 2070
- Prevalence and risk factors associated with tuberculosis mortality in Brunei Darussalam