
Effect of pH, lactate, electrolyte, and strong ion difference variability on prediction of intensive care unit mortality: A retrospective study
2022-10-17 12:28:38FurkanTontuSinanAsarBeyzaOrenBilgin
Journal of Acute Disease 2022年5期
Furkan Tontu, Sinan Asar, Beyza Oren Bilgin
1Department of Anesthesiology and Reanimation, Agri Training and Research Hospital, Agri, Turkey
2Department of Anesthesiology and Reanimation, Bak?rk?y Dr. Sadi Konuk Training and Research Hospital, Istanbul, Turkey
ABSTRACT Objective: To investigate the effect of the variability of Nas, Cls, Ks,lactate values and sodium effect (NaEffect), chloride effect (ClEffect),non-lactate strong ion difference (SIDnl) values calculated according to Stewart’s approach on predicting intensive care unit (ICU)mortality.Methods: The study was conducted on 1 539 patients,retrospectively. Serum Na (Nas), serum Cl (Cls), serum K (Ks),serum Ca (Cas), serum Mg (Mgs), lactate, pH values and SIDnl,NaEffect, ClEffect, APACHE Ⅱ (first, last), and SOFA (frist, last) scores were recorded. Radiometer ABL 800 (Denmark) was used for blood gas analysis. The variability of each parameter was calculated. The effect of variability of each parameter on 30-day ICU mortality was analyzed.Results: The variability of lactate (P<0.001, OR=0.580, 95%CI=0.505-0.652), pH (P=0.001, OR=0.004, 95% CI=0.000-0.104),NaEffect (P<0.001, OR=0.550, 95% CI=0.378-0.592), Ks (P<0.001,OR=0.385, 95% CI=0.244-0.565) values were protective factors of ICU mortality and Cls value was a risk factor (P=0.004, OR=1.095,95% CI=1.024-1.164). Variability of ClEffect, SIDnl values did not affect ICU mortality.Conclusions: The variability of electrolytes is important.Electrolyte, effects, and lactate variability can guide treatment and fulid applications in ICU.
KEYWORDS: Electrolyte; Variability; Mortality; Sodium; Chloride;Lactate; ICU
1. Introduction
Electrolyte imbalance is a common problem in the critically ill. It is related to mortality and morbidity[1]. The Stewart approach, which is increasingly used by intensive care physicians, revealed that electrolyte imbalance and acid-base disorders should be evaluated together[2].
In the Stewart approach, there are three main determinants of acidbase status:in vivopartial pressure of carbon dioxide (pCO2), total non-volatile weak acids (ATOT), and strong ion difference (SID). SID is the primary metabolic factor of the physicochemical approach[3].Gilfixet al. explained the effect of changes in non-lactate strong ion difference (SIDnl) and ATOTon pH with 4 simple mechanisms[sodium effect (NaEffect), chloride effect (ClEffect), albumin effect, other effects][4].
Nowadays, we can interpret the instant biochemical values of the patients as well as the former values and the change between them,through computer programs used in the intensive care unit (ICU).Recently, variability in serum electrolytes has attracted attention as a new risk factor for in-hospital mortality in critically ill patients[5].The variability, which helps us to follow the trend in addition to instant biochemistry measurements, is important in the follow-up of serum electrolyte values in critically ill patients. Our aim in this study was to investigate the relationship between variability of serum electrolyte values (Nas, Cls, Ks), lactate, effects (NaEffect, ClEffect), and SIDnlon 30-day ICU mortality.
2. Patients and methods
2.1. Ethical statement
The study was approved by the Health Sciences University Bak?rk?y Dr.Sadi Konuk Training and Research Hospital Clinical Research Ethics Committee with the approval number 2021-16-06. Informing and consent forms were obtained from patients or relatives.
2.2. Study population
Patients who were admitted to Intensive Care Unit, Department of Anesthesiology and Reanimation, Bak?rk?y Dr.Sadi Konuk Training and Research Hospital from 31 December 2013 to 31 December 2020 were included and divided into two groups (survivors and non-survivors). This study was registered to ‘ImdSoft-Metavision/QlinICU Clinical Decision Support Software (Israel)’.
2.3. Inclusion and exclusion criteria
All patients above the age of 17 who were admitted to medical and surgical ICU were included. Patients with hospitalizations less than 30 day and patients without APACHE Ⅱ and SOFA scores,electrolytes, effects, or scores were excluded.
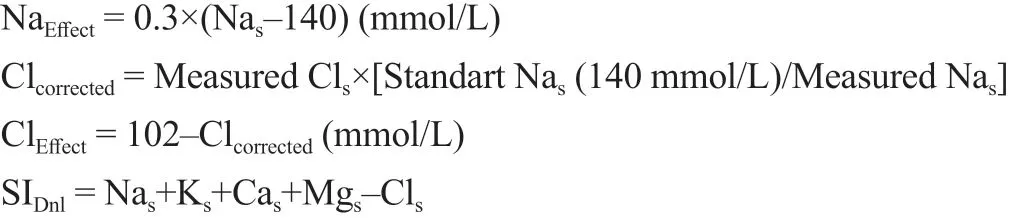
2.4. Definitions and calculations of the effects and SID
The four effects suggested by Gilfixet alare as follows[4]:
1) NaEffect: The SID is found by subtracting the concentration of the positively charged strong ions and the negatively charged strong ions. Changes in the amount of solvent,i.e.water, concentrate, or dilute the solution, thereby changing the SID[6]. This diluting effect of water is called the “free water effect”;
2) ClEffect: It measures the effect of Clsdeviation from normal.However, due to the dilution effect on Cls, corrected Cls(Clcorrected)must be calculated;
3) Albumin effect: It shows the effect of albumin change on standard base excess (SBE);
4) Other effects: It is found by subtracting the sum of the other 3 effects from SBE.
The calculation of the effects and SIDnlwith the formulas of Stewart’s approach, which was previously defined in the Decision Support System, was made by the system and the following formulas were used[4,6.7]:
2.5. Measurement
Nas, Cls, Ks, Cas, Mgs, lactate, pH values and their SIDnl, NaEffect,ClEffect, APACHE Ⅱ (first, last), and SOFA (first, last) scores were recorded. Radiometer ABL 800 (Denmark) was used for blood gas analysis. The variability of each parameter was calculated.Variability is defined as the 30-day standard deviation of the daily mean of all measurements performed in the ICU. The effect of variability of each parameter on 30-day ICU mortality was analyzed.
2.6. Statistical analysis
Data obtained from the Clinical Decision Support system were transferred to an Excel file. The collected data were evaluated by SPSS version 22.00 (SPSS Inc., Chicago, IL). Median (range/IQR), frequencies, and percentages were used for descriptive data.The normal distribution of the quantitative data was tested with the Kolmogorov-Smirnov test and graphical examinations. Survivor and non-survivor groups were compared with Mann WhitneyUfor continuous variables, Chi-square, and Fisher exact test for categorical variables. Potential factors affecting ICU mortality were analyzed by logistic regression analysis. AP-value of <0.05 was considered significant.
3. Results
A total of 1 539 patients were included as shown in Figure 1,including 39.4% (n=607) female and 60.6% (n=932) male. The median age of the patients was 67 years (54-78). The mortality rate was 64.84% (n=998). A total of 1 385 patients were admitted to the ICU for non-surgical reasons and 154 for surgical reasons. The differences in age, height, APACHE IIlast, SOFAfirst, and SOFAlastwere statistically significant between non-survivor patients and survivor patients (P<0.01) (Table 1). The levels of lactate, pH, Cls, Ks, NaEffectvariability were statistically higher in non-survivor patients than in survivor patients (P<0.01) (Table 2).
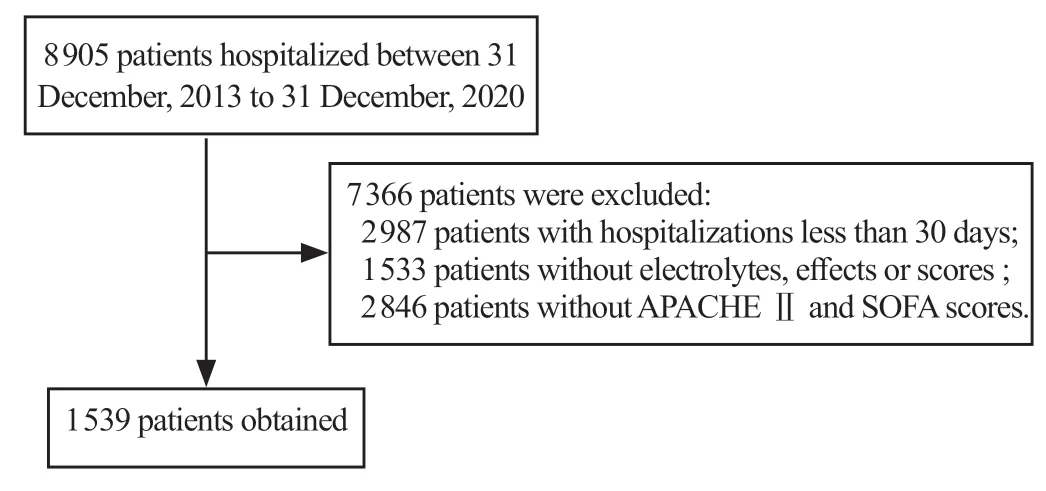
Figure 1. Diagram showing artificial intelligence (AI)-based algorithm approach.
The variability of lactate, pH, Ks, and NaEffectvalues were protective factors of 30-day ICU mortality. The variability of Clsvalues was a risk factor for 30-day ICU mortality (P=0.004,OR=1.095, 95%CI=1.024-1.164) (Table 3).
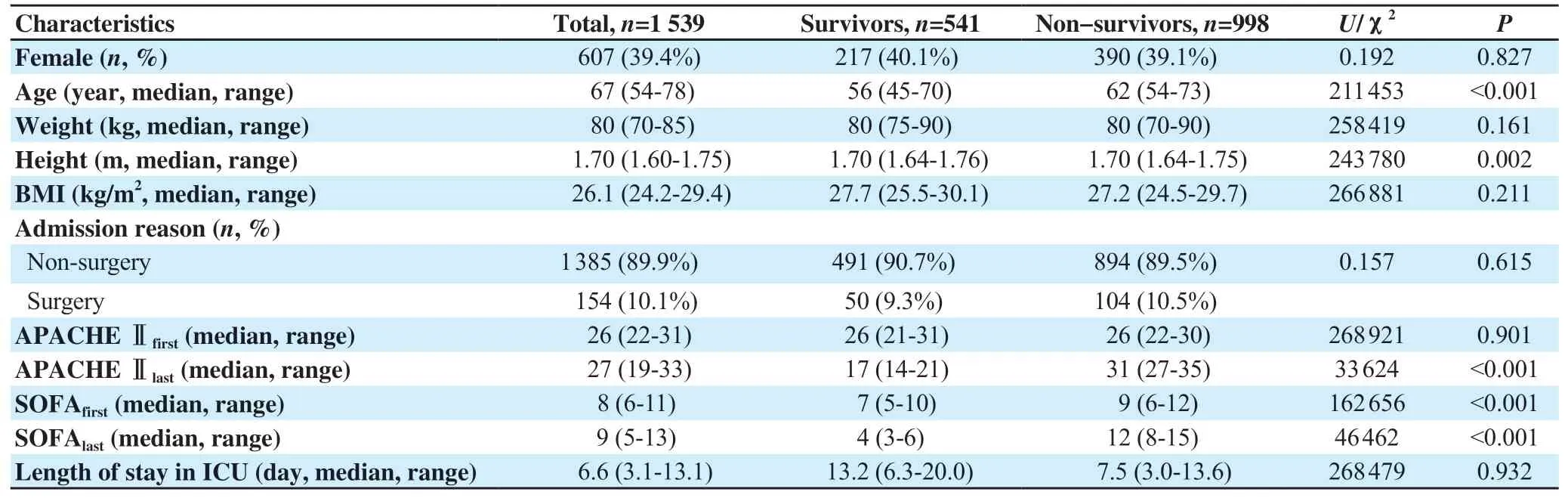
Table 1. Demographic and clinical characteristics.
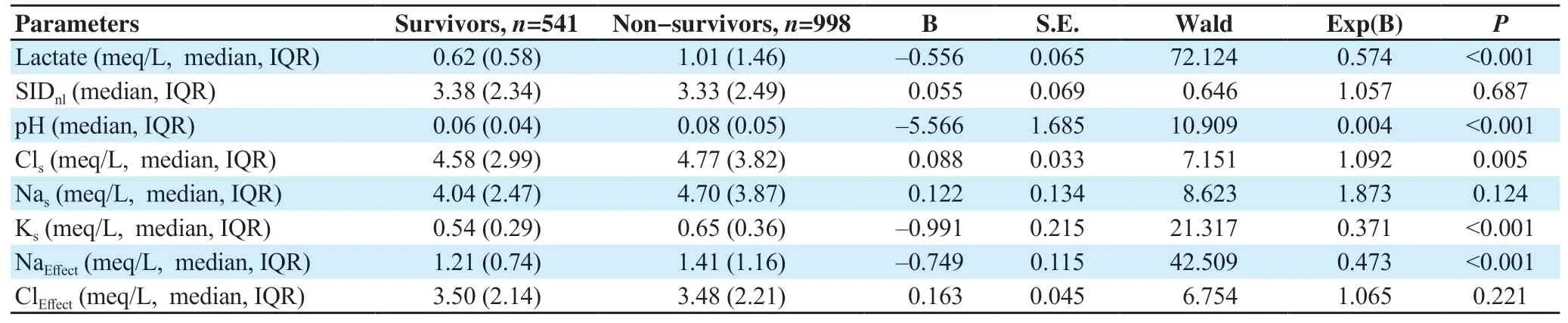
Table 2. Analysis of lactate, electrolytes, strong ion difference and effects.
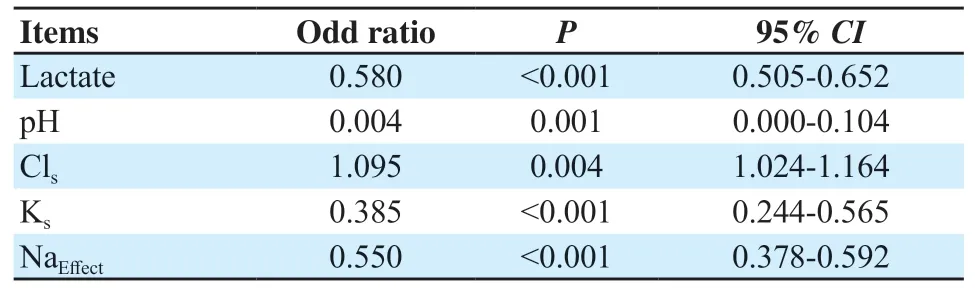
Table 3. Multivariate logistic regression analysis for 30-day mortality.
4. Discussion
Intensive care specialists make great efforts to manage problems with fluids, electrolytes, blood pH, and maintain acid-base balance[8].The optimum pH range for human cells is 7.35-7.45. Below or above this narrow range is called acidemia or alkalemia. Both acidemia and alkalemia are associated with mortality in ICU[9]. It is also known that pH predicts mortality in ICU patients[10]. Our study finds that low pH variability is protective against mortality.
Control of Clsconcentration could regulate the acid-base balance and maintain homeostasis[11]. Clsconcentration varies depending on the change in the body’s acid-base balance,viarenal excretion and transfer from the cell membrane due to Donnan effects[12]. Higher Clsvariability was associated with increased mortality. However,ClEffectvariability is not associated with mortality. The ClEffectformulation described by Gilfixet aluses Clcorrectedinstead of Cls.This correction was criticized in the previous study[13]. Alterations in Clslevels and hyperchloremia have been reported to be associated with increased hospital mortality[14-17]. These studies also show that Clsshould be considered without correction.
Nasconcentration is under hormonal control for the control of plasma osmolality and water balance. Nasvariability was not associated with mortality, while decreased NaEffectvariability was found to be protective against mortality. The free water effect is common but minor, a 10 mmol/L decrease in Nasconcentration contributes to a -3.3 mmol/L change in SBE[6]. Despite this, the results of our study show that the free water effect cannot be ignored in the acid-base balance of the human body, which consists of 50%-80% water from birth to death. Our study reveals that NaEffectis a valuable parameter when evaluating the contribution of Nasto acidbase balance.
The decreased Ksand lactate variability were found to be protective against mortality. It has been shown that low Ksvariability has a reducing effect on mortality[18,19]. It is already known that high lactate levels[20-23] and decreased lactate clearance[21-24] are associated with high mortality. This condition is associated with adequate tissue oxygenation and oxygen utilization.
The main determinant of SIDnl, which is the key to the pH control mechanism in the body, is the concentration difference between Nasand Clsions[3]. Although the relationship between SIDnl values and mortality is known, SIDnlvariability did not significantly affect mortality in our study.
The retrospective observational nature of this study is limiting.Including SBE and bicarbonate in the study would have enriched the study.
The variability, whose importance has increased recently, may be useful in the follow-up of intensive care patients. Electrolyte, effects and lactate variability can guide our treatment and fluid applications in ICU. In this study, lower pH, lactate, NaEffect, and Ksvariability were associated with decreased ICU mortality and higher Clsvariability was associated with increased ICU mortality.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This study received no extramural funding.
Authors'contributions
F.T., S.A., B.O.B.: Concept and design of study or acquisition of data or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content.
 Journal of Acute Disease2022年5期
Journal of Acute Disease2022年5期
- Journal of Acute Disease的其它文章
- Congestive heart failure masquerading as acute abdomen: A case report
- Symmetrical peripheral gangrene triggered by Escherichia coli sepsis
- Successful management of depression skull fracture in a boy with dog bite injury: A case report
- COVID-19 presentation as acute pancreatitis: A case report
- Effectiveness of ChAdOx1 nCoV-19 coronavius vaccine in preventing severe disease and mortality during the second wave of pandemic: A case-case analysis from a tertiary care center in South India
- Comparative efficacy of ketamine, lidocaine, acetaminophen, and dexmedetomidine combined with morphine patient-controlled analgesia in treating opium-addicted patients undergoing tibia fracture surgery: A randomized clinical trial