
Prednisolone induced pneumatosis coli and pneumoperitoneum
2022-08-12 08:47:52SereneGohVishalShelat
World Journal of Gastroenterology 2022年28期
Serene S N Goh,Vishal Shelat
Abstract Pneumatosis intestinalis (PI) is defined as the presence of gas within the submucosal or subserosal layer of the gastrointestinal tract. It is a radiologic sign suspicious for bowel ischemia, hence non-viable bowel must be ruled out in patients with PI. However, up to 15% of cases with PI are not associated with bowel ischemia or acute abdomen. We described an asymptomatic patient with prednisolone-induced PI and modified the Naranjo score to aid in a surgeon’s decision-making for emergency laparotomy vs non-operative management with serial assessment in patients who are immunocompromised due to long-term steroid use.
Key Words: Benign pneumatosis; Pneumatosis coli; Pneumatosis intestinalis; Prednisolone
TO THE EDITOR
We read with interest the report by Azzaroliet al[1], who conservatively managed two patients with benign pneumatosis intestinalis (PI). We would like to share a similar clinical case with prednisolone-induced pneumatosis coli and propose a modified Naranjo score for prednisolone-induced pneumatosis.

Figure 1 Computed tomography of abdomen and pelvis and serial erect abdominal radiographs showing interval improvement in pneumatosis coli and resolution of pneumoperitoneum. A: First admission day. Pneumatosis coli from cecum to transverse colon; B: 2 wk after admission. Progression of pneumatosis coli and pneumoperitoneum; C: 2 wk Post-hyperbaric oxygen therapy. Resolution of pneumoperitoneum and pneumatosis coli.
A 71-year-old lady with dysphagia and diplopia symptoms was diagnosed with Neuromyelitis Optica (NMO). Treatment with prednisolone 20 mg once daily improved her diplopia. Nasogastric tube(NGT) feeding was commenced due to malnourishment from dysphagia. The chest radiograph for NGT placement showed pneumoperitoneum, and she was referred urgently to the surgical unit. She was asymptomatic, afebrile with normal hemodynamics. Abdomen was soft and non-tender. Leukocyte count, procalcitonin, lactate, and arterial blood gas were normal. A computed tomography of abdomen and pelvis (CTAP) with intravenous and NGT contrast confirmed pneumoperitoneum and pneumatosis coli from cecum to splenic flexure (Figure 1). There was no contrast extravasation, portal venous gas,inflammatory pathology, or mesenteric ischemia. Non-operative management with nil enteral feeding,serial abdominal examination, serum tests, and abdominal radiographs (AXR) was done. The patient remained asymptomatic with normal serum tests. A repeat CTAP showed minimal improvement of pneumoperitoneum. A follow-up AXR two weeks later showed worsening of pneumatosis coli.Hyperbaric oxygen therapy (HBOT) was arranged. Five HBOT sessions were performed at 2.2 atmospheric pressure for 90 min. Her abdominal girth reduced from 79 to 73 cm with minimal AXR improvement. Prednisolone was weaned over next five days and she was discharged well on oral diet.At two-weeks outpatient follow-up, AXR showed improvement (Figure 1).
Corticosteroid therapy remains the cornerstone for the treatment of autoimmune diseases. The true incidence of benign PI as an ADR secondary to corticosteroids is unknown[2,3]. The hypothesis is due to atrophy of lymphoid follicles in the bowel wall. Although PI occurred after prednisolone's commencement in our patient, we did not initially stop prednisolone in balancing riskvsbenefits for NMO therapy. When PI worsened, HBOT was offered due to concerns for secondary bowel ischemia from PI. The HBOT regimen was similar to that described by Feuersteinet al[4], who suggested at least three sessions. As our patient's PI improved but did not resolve fully after 5 HBOT sessions, we reduced prednisolone dose. After two weeks of cessation, PI resolved, similar to a report described by Choiet al[5].
According to the Naranjo score (adverse drug reaction probability scale) of 6, PI was probably caused by prednisolone in our patient. Naranjo score recommends isolation of drug in toxic concentrations in body fluid, response to placebo administration, and drug rechallenge to evaluate for the occurrence of symptoms. These three criteria are not routinely done due to practical and safety reasons[6]. We propose a modified Naranjo score (Tables 1 and 2) for prednisolone-induced pneumatosis which replaces these three criteria with the following: (1) No symptoms or signs of abdominal pathology; (2)Serum investigations for inflammatory markers (e.g., C-reactive protein and procalcitonin) must be normal; and (3) Imaging studies should rule out hollow viscus perforation or inflammatory abdominal pathology as a cause for PI. With the modified Naranjo score, the causal link of PI due to prednisolone becomes definite. We propose validation of modified Naranjo score.
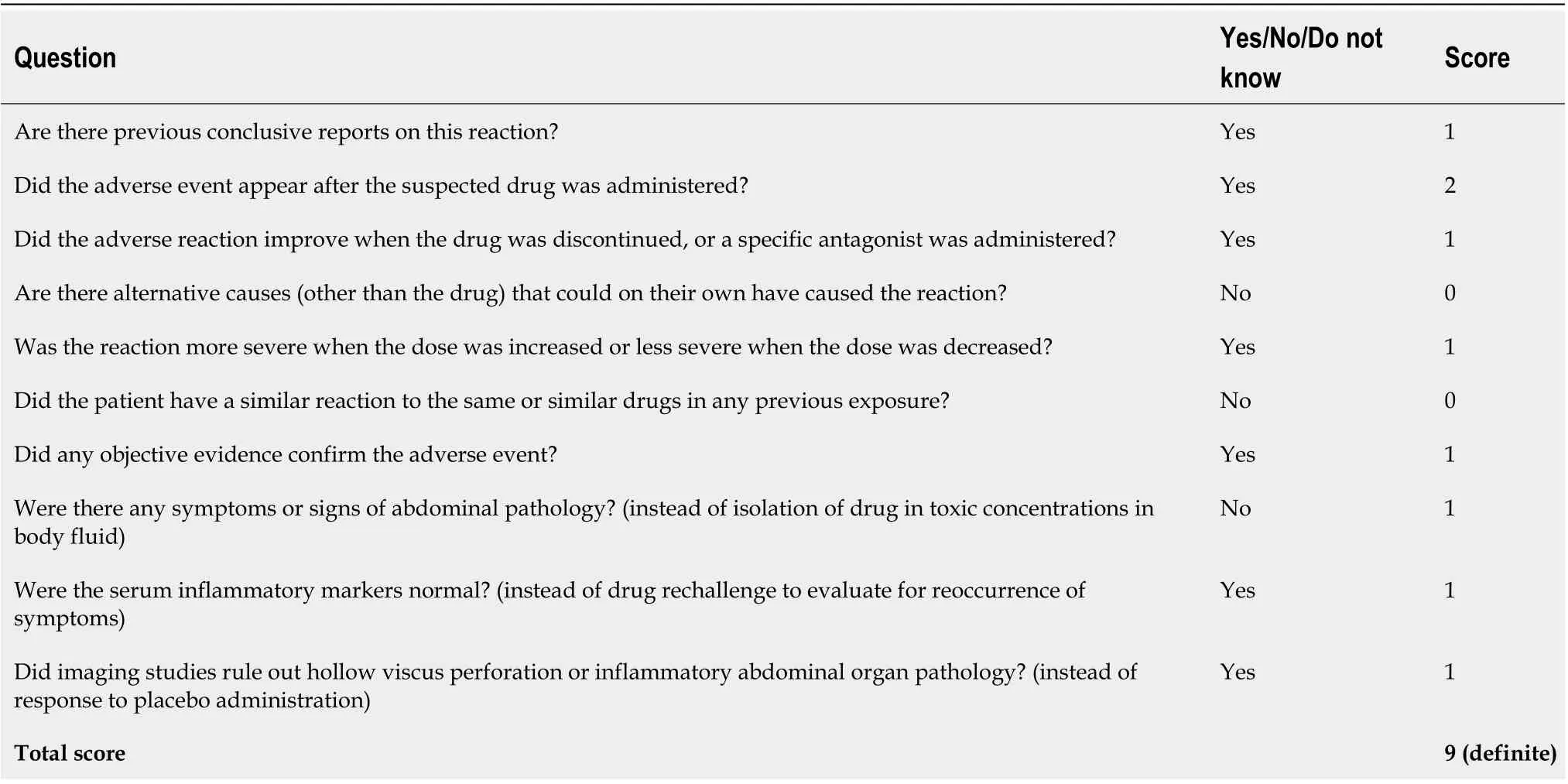
Table 1 Modified Naranjo score-pneumatosis intestinalis specific score

Table 2 Interpretation of scores
FOOTNOTES
Author contributions:Goh SSN wrote the letter; Shelat V revised the letter.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Singapore
ORCID number:Serene S N Goh 0000-0003-4916-2142; Vishal Shelat 0000-0003-3988-8142.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
 World Journal of Gastroenterology2022年28期
World Journal of Gastroenterology2022年28期
- World Journal of Gastroenterology的其它文章
- Endoluminal vacuum-assisted therapy as a treatment for anastomotic leakage in colorectal surgery
- Is patient satisfaction sufficient to validate endoscopic anti-reflux treatments?
- Delayed immune-related sclerosing cholangitis after discontinuation of pembrolizumab: A case report
- Global research on Clostridium difficile-associated diarrhoea: A visualized study
- Family-based Helicobacter pylori infection status and transmission pattern in central China, and its clinical implications for related disease prevention
- Gastric mucosal precancerous lesions in Helicobacter pylori-infected pediatric patients in central China: A single-center, retrospective investigation