
Pseudo-Wellens syndrome secondary to postexercise syncope
2022-06-27 10:38:18ShuFangZhihaoLiuQiJinYuxiLiWenhuiDingHaoyuWengTieciYiJianpingLi
World Journal of Emergency Medicine 2022年4期
Shu Fang, Zhi-hao Liu, Qi Jin, Yu-xi Li, Wen-hui Ding, Hao-yu Weng, Tie-ci Yi, Jian-ping Li,4
1Department of Cardiology, Peking University First Hospital, Beijing 100034, China
2Department of Cardiology, Xiamen Cardiovascular Hospital, Xiamen University, Xiamen 361004, China
3Department of Cardiology, Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University, Shanghai 200032, China
4Key Laboratory of Molecular Cardiovascular Sciences of Ministry of Education, Health Science Center, Peking University, Beijing 100034, China
Corresponding Author: Jian-ping Li, Email: lijianping03455@pkufh.com
Dear editor,
Wellens syndrome is characterized by electrocardiography (ECG) patterns of the biphasic or inverted T wave in the precordial leads with normal R wave progression and absence of Q waves,which indicates occlusive lesions of the proximal left anterior descending (LAD) coronary artery and warrants.These ECG changes usually occur during a pain-free interval and turn to a fatal consequence if without urgent intervention therapy.However, in some cases, coronary stenosis was absent and ECG patterns manifested as Wellens syndrome, which was defined as pseudo-Wellens syndrome.The mechanism of pseudo-Wellens syndrome is not well defined, posing a challenge to the diff erential diagnosis. Acute myocardial infarction is a common cause of syncope with a variety of ECG abnormalities,but the ECG pattern of Wellens syndrome secondary to syncope has not been reported. We focus on this rare phenomenon and hope to attract emergency physicians’ attention.
CASE
A 30-year-old man presented to the emergency room for amaurosis and transient loss of consciousness (lasting for about 10-30 s) a few minutes after strenuous exercise. He had no symptoms of chest pain, tightness, palpitation, dyspnea, nausea, vomiting or headache during the preceding or the following course at the onset of syncope. Similar symptoms had already occurred twice before, both after exercise in hot weather. Dyskinesia, cyanosis, tonic-clonic, and generalized atonic seizures were not witnessed. The past medical history included untreated hypertension for 5 years with a maximum blood pressure of 140/100 mmHg (1 mmHg=0.133 kPa) and well-controlled ulcerative colitis with mesalazine therapy. He denied smoking, drinking, and drug abuse (such as cocaine and marijuana). He had a family history of hypertension, but none of his family members suff ered from sudden death, syncope, or premature coronary heart disease.
On admission, his blood pressure was 141/90 mmHg, heart rate was 62 beats/min, and respiratory rate was 15 breaths/min. Physical examination of the respiratory, cardiac, abdominal and neurological systems was unremarkable. Brain computed tomography (CT) revealed no subarachnoid hemorrhage or hemorrhagic stroke evidence. ECG on admission showed sinus rhythm, biphasic T waves in leads V3-V4, inverted T waves in lead V5, and normal R wave progression without Q waves in precordial leads, consistent with the ECG pattern of Wellens syndrome (Figure 1A). Laboratory tests revealed a normal concentration of troponin I, blood electrolytes, serum glucose, and thyroid hormone. Echocardiography showed normal ventricular wall motion with an ejection fraction of 69.9% and a thickening of the interventricular septum base of 13.4 mm (Figure 2A). Exercise stress echocardiography showed that that left ventricular outflow tract obstruction (LVOTO) with a peak velocity of the left ventricular outflow tract (LVOT) was 342.1 cm/s and the LVOT gradient was 42.0 mmHg, but hypotension and discomfort were not noted (Figure 2B). The patient was suspected of suffering an acute coronary artery event because of the initial Wellens syndrome ECG pattern. However, acute coronary syndrome was nearly excluded because of no chest pain, no risk factors for coronary artery disease (except hypertension), negative troponin I, and normal ventricular wall motion. Therefore, emergency coronary angiography was not performed. Furthermore, the 24-h Holter monitoring showed an average sinus rhythm of 62 beats/min (normal range: 44-101 beats/min) without malignant arrhythmias. Coronary CT angiography revealed a normal course and origin of the coronary arteries without coronary artery stenosis. Cardiac magnetic resonance imaging showed the normal function and structure of the heart, and the normal perfusion of the myocardium. With dangerous cardiogenic syncope being ruled out, the patient underwent tilt table testing to evaluate autonomic nerve regulation subsequently. After being positioned in a head-up tilt position at a tilt angle of 70 degrees for 20 min and sublingual use of nitroglycerin 0.25 mg for 8 min, the patient developed symptoms of amaurosis, nausea and diaphoresis. At the onset of symptoms, the monitoring equipment recorded tachycardia, significantly decreased blood pressure and right middle cerebral artery (RMCA) blood flow velocity (Table 1). The tilt table testing was positive, indicating the impaired autonomic nerve regulation, and the patient was diagnosed with post-exercise syncope.
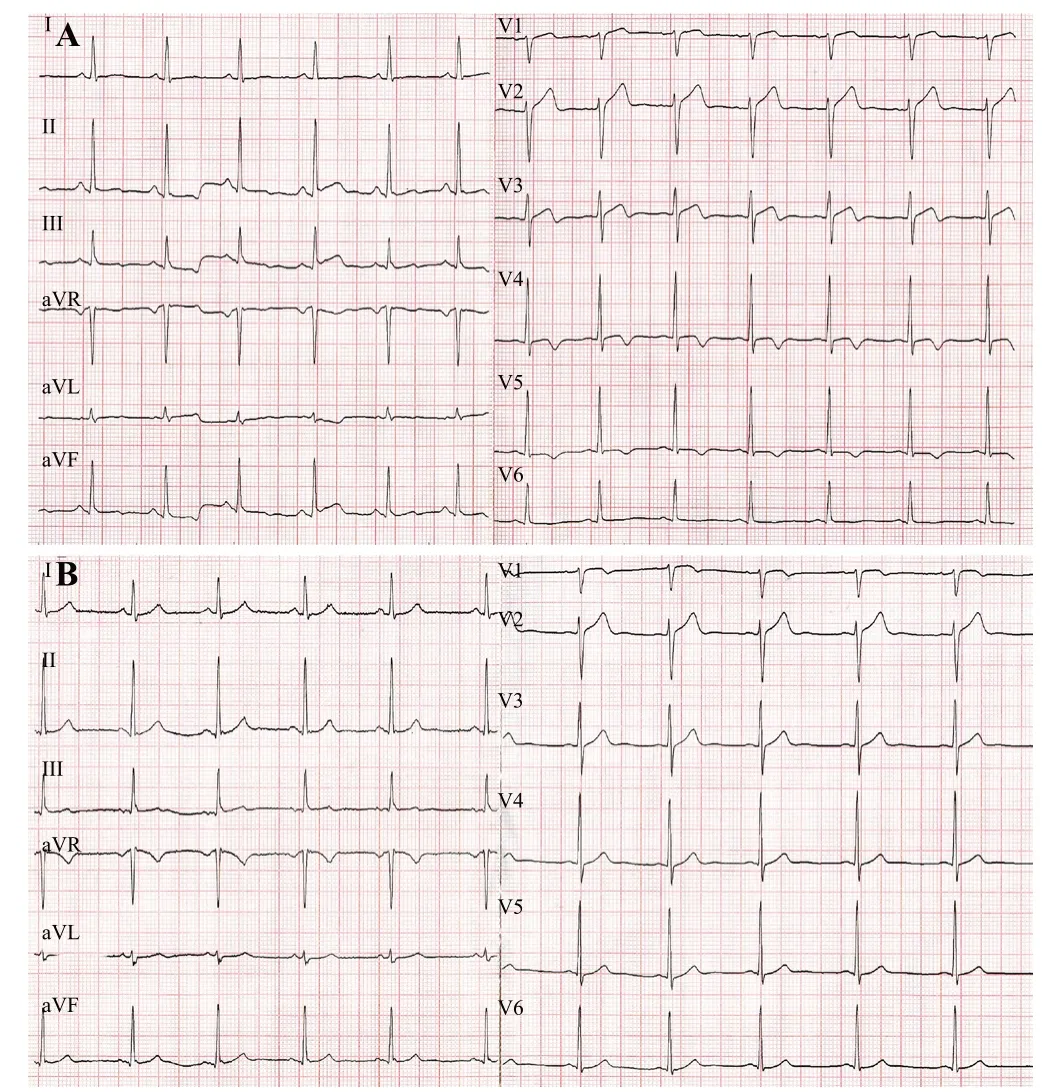
Figure 1. The patient’s electrocardiography (ECG) showed sinus rhythm, biphasic T waves in leads V3-V4, inverted T waves in lead V5, normal R wave progression without Q waves in precordial leads on admission (A). At one-month follow-up, his ECG showed abnormal T waves in leads V3-V5 returned to be upright (B).
We recommended the patient drink enough water, replenish electrolytes before exercise, and avoid abruptly stopping strenuous exercise. At the one-month follow-up, no episode of syncope was noted, and ECG showed an upright T wave in leads V3-V5 in this patient (Figure 1B).
DISCUSSION
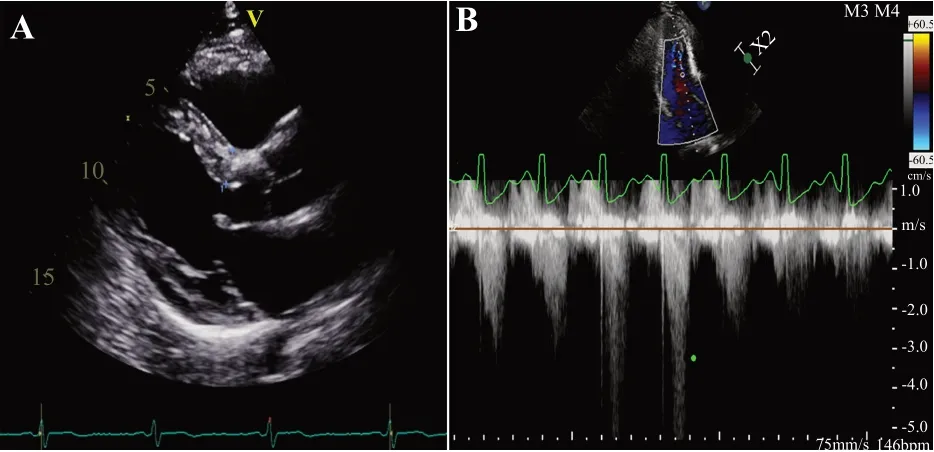
Figure 2. The results of the patient’s echocardiography. A: parasternal long-axis view on admission showed asymmetric hypertrophy of the left ventricle, and the thickening of the interventricular septum base of 13.4 mm; B: exercise stress echocardiography showed peak velocity of left ventricular outflow tract increased from 147.2 cm/s (at rest) to 342.1 cm/s, left ventricular outflow tract gradient increased from 8.6 mmHg (at rest) to 42.0 mmHg.

Table 1. Recorded data of HR, BP and RMCA blood flow velocity of the patient during tilt table testing
Wellens syndrome was first described by de Zwaan et alin 1982, characterized by deeply inverted (type A) or biphasic (type B) T waves in leads V2 and V3 (sometimes in V1, V4-V6), normal precordial R-wave progression, no pathologic Q waves, isoelectric or minimally ST-segment elevation less than 1 mm in addition to a history of angina and normal or minimal elevated cardiac enzymes.It was associated with severe stenosis of the proximal LAD coronary artery, and three-quarters of patients developed anterior myocardial infarction in a median of 9 d.Although the presence of Wellens syndrome ECG pattern has a high diagnostic value for LAD occlusion, a small portion of patients with Wellens ECG syndrome pattern have completely normal coronary artery anatomy and this is defined as pseudo-Wellens syndrome. In the previously reported cases, pseudo-Wellens syndrome has been described in patients with acute cholecystitis,myocardial bridge,pulmonary embolism,left ventricular hypertrophy,and drug abuse, such as cocaine and marijuana use,all of which can cause interruption or reduction in coronary blood flow (e.g. coronary artery spasm, increased ventricular strain, and increased vagal tone) without severe stenosis.
Syncope is defined as transient loss of consciousness due to cerebral hypoperfusion, characterized by a rapid onset, short duration, and complete spontaneous recovery.Cardiac syncope, such as acute myocardial infarction, pulmonary embolus, and acute aortic dissection, is often life-threatening. Physicians need to be vigilant, especially when there are ECG abnormalities. To the best of our knowledge, this is the first case report of pseudo-Wellens syndrome secondary to postexercise syncope.
In this case, a series of cardiac tests ruled out cardiac syncope. As the patient was an athletic young man and the symptoms occurred after strenuous exercise, postexercise syncope should be considered. The pathophysiology of postexercise syncope may be hypotension due to dehydration-related hypovolemia, impaired postexercise vasoconstriction, vagal nerve overexcitation, and hypocapnia-induced cerebral vasocontraction.The mechanisms of postexercise syncope-related pseudo-Wellens ECG pattern have not been elucidated. T wave evolvement was correlated with reperfusion injury and myocardial hibernation, which was reported as “cardiac memory” in an early study.Based on this theory, we speculated that cardiac electrical activity might be influenced by cardiac hypoperfusion during syncope in this patient. In addition, the low-volume state after exercise will aggravate LVOTO and increase ventricular strain when complicated by the thickening of the interventricular septum base which might also involve the episodes of syncope and cardiac hypoperfusion, and cause T-wave inversion.
CONCLUSIONS
In summary, we report a rare case of pseudo-Wellens syndrome secondary to postexercise syncope. Therefore, clinicians should fully recognize the dangers of Wellens syndrome and identify pseudo-Wellens syndrome caused by extraordinary circumstances to avoid unnecessary invasive procedures.
Funding: None.
Ethical approval: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflicts of interest: The authors declare that there were no conflicts of interest regarding the publication of this paper.
Contributors: SF proposed and wrote the first draft. SF and ZHL contributed equally to this work. All authors contributed to the design and interpretation of the study and to further drafts.