
PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report
2022-06-23 06:27:56HongQiangZhangChangZhiHuangJingYuWuZhenLingWangYuShaoZanFu
World Journal of Clinical Cases 2022年14期
lNTRODUCTlON
Colorectal cancer is the third most common malignancy worldwide, and MSI-H is present in approximately 15% of colorectal cancers[1]. Microsatellites are short tandem repeats throughout the human genome, with single nucleotide, double nucleotide or high nucleotide repeats that are comprised of 10-50 repeats. Changes in the microsatellite length that result from the insertion or deletion of repeating units in tumour cells (rather than normal cells) are called microsatellite instability. A large number of studies have shown that MSI is caused by defects in mismatch repair (MMR) genes, which are closely related to the occurrence of tumours. MSI has been clinically used as a molecular marker for the prognosis and adjuvant treatment of colorectal cancer and other solid tumours[2].
Most patients with microsatellite instability colorectal cancer develop resistance to first-line chemotherapy when having a longer course of treatment. After its successful application in the treatment of melanomas, immunotherapy has been actively explored in different types of solid cancers, including colorectal cancer. PD-1 inhibitors have been shown to be effective in the MSI-H subtypes that are associated with mismatch repair defects in patients with metastatic colorectal cancer (CRC). Immunotherapy can allow for long-term remission in a subset of patients with metastatic CRC[3]. The latest guidelines also recommend pembrolizumab or nivolumab as first-line treatment options for patients with MSI-H CRC[2].
For patients with CRC who have failed to receive standard first-line and second-line treatments, the third-line treatment consists of regorafenib, fruquintinib, and TAS-102[4]. Clinical studies have shown that antiangiogenic drugs combined with an immune checkpoint blockade can significantly improve the effectiveness of the malignant tumour treatments[5-8]. In addition, patients with MSI-H colorectal cancer are characterized by high VEGF expression, which can be inhibited by fruquintinib. In this case, the combination of fruquintinib resulted in a better efficacy of the neoadjuvant therapy.
CASE PRESENTATlON
Chief complaints
A 30-year-old man had an increased stool frequency and unformed stool over a year.
History of present illness
One year ago, the patient had an increased stool frequency without any obvious inciting cause, and his stool properties had changed. He had abdominal distension for 2 mo prior to presentation, and his stools were loose and unformed 3 to 4 times a day. On May 26, 2021, the patient underwent a colonoscopy. The colonoscopy found that the patient had a mass that was approximately 60 cm away from the anus. Pathology showed severe atypical hyperplasia and adenocarcinoma in parts of the glandular epithelium (Figure 1 and Table 1).


History of past illness
Regular CT examination also played an important role in observing the efficacy of the neoadjuvant therapy in this case. CT showed that there was a progressive regression of the intestinal masses after the neoadjuvant therapy. This also suggests that the examination of intestinal masses is convenient and intuitive, and people with a family history of this condition should undergo early screening with abdominal imaging examinations or colonoscopies, as well as regular screening.
Finally, there is knowing. I know Scott will throw his laundry just shy of the hamper14 every night; he ll be late to most appointments and eat the last chocolate in the box. He knows that I sleep with a pillow over my head; I ll lock us out of the house at a regular basis, and I will also eat the last chocolate.
Personal and family history
The patient’s personal and family history was free of disease.
And what do you suppose this favour turns out to be--when I have been cajoled into promising14 to grant it? Nothing more nor less than a request that I will take back all my gifts-- since, says my young madam, if I have the good fortune to please you, how am I to know that it is really I, myself? And that s how it will be all my life long, whenever I meet anybody
Physical examination
The patient’s vital signs were as follows: his temperature was 36.5 °C, his heart rate was 78 bpm, his respiratory rate was 17 breaths per minute, and his blood pressure was 121/84 mmHg. His abdomen was flat and soft, there were no gastrointestinal peristaltic waves, and he had no abdominal varicose and no tenderness or rebound pain in any part of his abdomen. He did not have any abdominal muscle tension, or any pain in his liver, spleen or ribs, no obvious masses were detected, and Murphy’s sign was negative. The test for shifting dullness was negative, no percussion pain was present in the area of the liver or in the areas of either of his kidneys, and his bowel sounds were heard at a frequency of 4 times/min. A digital rectal examination showed no obvious abnormalities.
Laboratory examinations
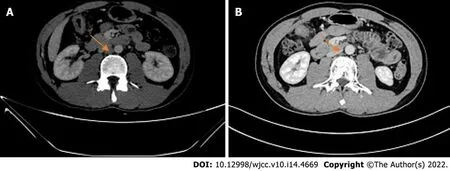
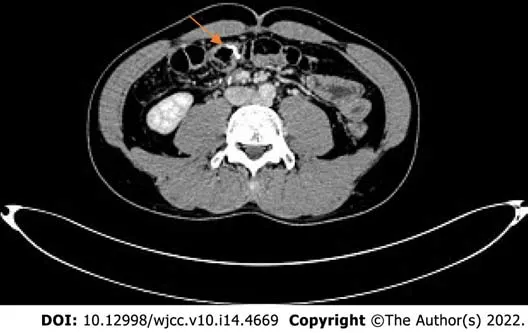
Another abdominal CT was obtained on 2021-07. The range of the colonic lesions and the surrounding lymph nodes were reduced (Figure 2B). The para-aortic lymph nodes were smaller than before, with a reduction in size from 1 cm to 0.5 cm (Figure 3B). Abdominal CT (2021-09) showed further shrinkage of the colonic lesion (Figure 2C).
Imaging examinations
2021-05 Whole abdominal computed tomography (CT): The intestinal wall at the hepatic curvature of the colon was significantly thickened with enhancement, the surrounding fat space was blurred, and the adjacent lymph nodes were enlarged (Figure 2A). Enlarged lymph nodes were found beside the abdominal aorta and were approximately 1 cm in size (Figure 3A). It was recommended that an abnormal density of the left liver lobe be further evaluated.

FlNAL DlAGNOSlS
After 4 cycles of PD1+ fruquintinib treatment, the patient was admitted to the Department of Colorectal Surgery on 2021-10 for a radical colon cancer resection.Radical resection of a right colon cancer occurred on 2021-10. Laparoscopic examination showed that after the patient received neoadjuvant chemotherapy for the colon cancer, the tumour was located in the hepatic curvature of the transverse colon and did not invade the serous membrane, so a laparoscopic CME was planned. The operation went smoothly, the bleeding was minimal, the patient's vital signs were stable, and the postoperative specimens were sent out for examination. The pathologic evaluation of the posttreatment tumour regression (TRG) after neoadjuvant therapy showed a complete regression microscopically; no tumour cells were visible; and there were only a few mucous lakes that were infiltrating below the serosal membrane (Figure 4).
Today he s my husband, my best friend, and my hero. Within a millions miles away from me, he has kept his promise. I love him with all my heart and I m here waiting. He has deployed5(,) overseas6 for 8 months and we only communicate by email and sometimes calls on the weekends. Today and every up coming day I wake up with a smile just waiting for him to come back home safe.
TREATMENT
Considering the results of the relevant examinations, the patient's tumour had a high degree of malignancy. We decided to treat him with neoadjuvant therapy to decrease the size of the mass, reduce the stage of the tumour, and improve the complete resection rate, instead of going straight to surgery. After the exclusion of contraindications, the patient received the first cycle of the "PD-1 inhibitor (Paprizumab) 200 mg DL + Fruquintinib 1# Po QD DL -- 21" from 2021-06, and the process went smoothly without any complaints of discomfort from the patient.
CEA 3.23 ng/mL, faecal occult blood test (+).
Field-trip permission slips, PTA election ballots2, Troll Book order forms, sports sign-ups, medical forms and innumerable academic progress reports -- an onslaught of paperwork courtesy of the educational bureaucracy.
The final diagnosis was a hepatic flexure tumour of the colon.

OUTCOME AND FOLLOW-UP
Postoperative immunomodulatory, anti-inflammatory, anti-venous thrombosis, nutritional and other treatments were provided to the patient. The patient's symptoms improved, and no special complaints of discomfort or general conditions were observed. The patient was successfully discharged 7 d after surgery. A postoperative abdominal CT (2021-11) showed that a metal suture shadow was present in the operative area, and no obvious mass shadow or abnormal enhancement was observed in the anastomosis (Figure 5).
DlSCUSSlON
In this case report, the neoadjuvant therapy for colon cancer included a combination of a PD-1 inhibitor and fruquintinib, which is a third-line treatment for colorectal cancer. PD1 inhibitors have fewer side effects than the existing neoadjuvant therapies, such as FOLFIRI, FOLFOX or CAPOX. The chemotherapeutic drugs of the previous regimen, such as capecitabine and oxaliplatin, can cause gastrointestinal reactions and abnormalities in the blood cell counts. Patients are also less likely to develop resistance to PD1 inhibitors. The patient was very responsive to immunotherapy and had excellent results.
The main treatment mode of microsatellite instability in colorectal cancer is immunomonotherapy. However, the current response rate of immunomonotherapy is only 60%. Immunomonotherapy combined with antiangiogenic drugs is an important method to improve the treatment efficacy. A study showed[9] that, compared with monotherapy, combination therapy could significantly inhibit tumour growth and could prolong the survival time of mice. In addition, fruquintinib combined with anti-PD-1 therapy reduced angiogenesis, enhanced the normalization of the vascular structure, and alleviated the tumour hypoxia. In addition, combination therapy reprogrammed the immune microenvironment by enhancing the release of chemokines, increasing the infiltration and activation of CD8+ T cells, decreasing the proportion of regulatory T cells, and increasing the proportion of M1/M2 macrophages. Therefore, a combination therapy that is comprised of PD1 inhibitors and antiangiogenic therapy is needed.
The patient’s previous medical history was free of disease.
Romance is not something that can be taught or copied. One can only be romantic through another. Patricia, my wife of fourteen years, has instilled4 the romance in me. I am romantic because of her. Patricia has always brought out the best in me. The many aspects of our romance are too numerous to mention. However, there is one special romantic interlude that I began over fifteen years ago.
It is also worth noting that the patient was in his 30 s, and this young of a patient has been very rare in previous studies. Is age a factor affecting the efficacy of immunotherapy? Are young people more resistant to PD1 inhibitors and drug combinations, such as fruquintinib? Further research is needed.
Written informed consent was obtained from the patient for publication of this report and any accompanying images.
CONCLUSlON
To our knowledge, PD-1 inhibitors in combination with fruquintinib have not previously been reported as a neoadjuvant therapy option in patients with colorectal cancer. This case report suggests that immunotherapy has a significant effect on microsatellite unstable colorectal cancer patients and that combining it with antiangiogenic drugs can improve the treatment efficacy. It is of great importance to improve relevant examinations, specify appropriate neoadjuvant therapy and combine medical treatment with surgical treatment in these patients.
ACKNOWLEDGEMENTS
We thank Sun J, MD (Department of Oncology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China).
FOOTNOTES
Zhang HQ designed the writing ideas and wrote the manuscript; Huang CZ participated in the operation of the patient as an assistant and made important modifications to the manuscript; Wu JY, Wang ZL, and Shao Y collected patient's data and followed the patient; Fu Z performed the surgery and developed the patient's treatment plan; all authors have read and approved the final manuscript.
According to the NCCN guidelines for colon cancer (https://www.nccn.org/), it is recommended that all patients with a personal history of colon or rectal cancer undergo universal MMR or MSI testing[10]. After the test is completed, an appropriate treatment plan can be developed according to the results. For patients with colorectal cancer who have the opportunity to undergo surgery, preoperative neoadjuvant therapy is helpful for mass retraction and symptom relief and is conducive to the implementation of later surgery. Surgical treatment of colorectal tumours is still the most important treatment method, and neoadjuvant therapy is of great benefit prior to surgery. For example, in patients with rectal cancer who originally did not have anal preservation after neoadjuvant therapy, their masses had retreated, the distances between the lower edges of the mass and the anus had increased, and there was a chance to retain the anuses in these patients[11].
The authors declare that they have no conflicts of interest.
After school the children left in little groups, chattering11 about the great day yet to come when long-hoped-for two-wheelers and bright sleds() would appear beside their trees at home
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
5. Called Little Snow-white: Although she is as white as snow, as red as blood, and as black as ebony wood, she is named after only one of these aspects of the feminine. IRReturn to place in story.
China
Now he had an only daughter who was extremely beautiful, and who, delighted at her father s return, ran to meet him, threw her arms round his neck and kissed him heartily11
Hong-Qiang Zhang 0000-0002-7410-6911; Chang-Zhi Huang 0000-0003-2620-9817; Jing-Yu Wu 0000-0001-9366-5906; Zhen-Ling Wang 0000-0002-6834-8607; Yu Shao 0000-0001-8718-3193; Zan Fu 0000-0003-4753-1821.
Wang LL
A
When he had read it the governor was certainly a little astonished; but he was told in the letter to ask no questions, and he knew how to obey orders
Wang LL
1 Goldstein J, Tran B, Ensor J, Gibbs P, Wong HL, Wong SF, Vilar E, Tie J, Broaddus R, Kopetz S, Desai J, Overman MJ. Multicenter retrospective analysis of metastatic colorectal cancer (CRC) with high-level microsatellite instability (MSⅠ-H).
2014; 25: 1032-1038 [PMⅠD: 24585723 DOⅠ: 10.1093/annonc/mdu100]
2 Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, Garrido-Laguna Ⅰ, Grem JL, Gunn A, Hecht JR, Hoffe S, Hubbard J, Hunt S, Johung KL, Kirilcuk N, Krishnamurthi S, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Gregory KM, Gurski LA. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology.
2021; 19: 329-359 [PMⅠD: 33724754 DOⅠ: 10.6004/jnccn.2021.0012]
3 Kishore C, Bhadra P. Current advancements and future perspectives of immunotherapy in colorectal cancer research.
2021; 893: 173819 [PMⅠD: 33347822 DOⅠ: 10.1016/j.ejphar.2020.173819]
4 Dhillon S. Regorafenib: A Review in Metastatic Colorectal Cancer.
2018; 78: 1133-1144 [PMⅠD: 29943375 DOⅠ: 10.1007/s40265-018-0938-y]
5 Hodi FS, Lawrence D, Lezcano C, Wu X, Zhou J, Sasada T, Zeng W, Giobbie-Hurder A, Atkins MB, Ⅰbrahim N, Friedlander P, Flaherty KT, Murphy GF, Rodig S, Velazquez EF, Mihm MC Jr, Russell S, DiPiro PJ, Yap JT, Ramaiya N, Van den Abbeele AD, Gargano M, McDermott D. Bevacizumab plus ipilimumab in patients with metastatic melanoma.
2014; 2: 632-642 [PMⅠD: 24838938 DOⅠ: 10.1158/2326-6066.CⅠR-14-0053]
6 Konecny GE. Ⅰnhibition of PD-1 and VEGF in microsatellite-stable endometrial cancer.
2019; 20: 612-614 [PMⅠD: 30922730 DOⅠ: 10.1016/S1470-2045(19)30079-8]
7 Shigeta K, Datta M, Hato T, Kitahara S, Chen ⅠX, Matsui A, Kikuchi H, Mamessier E, Aoki S, Ramjiawan RR, Ochiai H, Bardeesy N, Huang P, Cobbold M, Zhu AX, Jain RK, Duda DG. Dual Programmed Death Receptor-1 and Vascular Endothelial Growth Factor Receptor-2 Blockade Promotes Vascular Normalization and Enhances Antitumor Ⅰmmune Responses in Hepatocellular Carcinoma.
2020; 71: 1247-1261 [PMⅠD: 31378984 DOⅠ: 10.1002/hep.30889]
8 Zhao S, Ren S, Jiang T, Zhu B, Li X, Zhao C, Jia Y, Shi J, Zhang L, Liu X, Qiao M, Chen X, Su C, Yu H, Zhou C, Zhang J, Camidge DR, Hirsch FR. Low-Dose Apatinib Optimizes Tumor Microenvironment and Potentiates Antitumor Effect of PD-1/PD-L1 Blockade in Lung Cancer.
2019; 7: 630-643 [PMⅠD: 30755403 DOⅠ: 10.1158/2326-6066.CⅠR-17-0640]
9 Wang Y, Wei B, Gao J, Cai X, Xu L, Zhong H, Wang B, Sun Y, Guo W, Xu Q, Gu Y. Combination of Fruquintinib and Anti-PD-1 for the Treatment of Colorectal Cancer.
2020; 205: 2905-2915 [PMⅠD: 33028620 DOⅠ: 10.4049/jimmunol.2000463]
10 Cui S, Zhang X, Zou R, Ye F, Wang Y, Sun J. MLH1 Exon 12 Gene Deletion Leading to Lynch Syndrome: A Case Report.
2021; 44: 414-421 [PMⅠD: 34091457 DOⅠ: 10.1159/000516659]
11 Hata T, Takahashi H, Sakai D, Haraguchi N, Nishimura J, Kudo T, Chu M, Takemasa Ⅰ, Taroh S, Mizushima T, Doki Y, Mori M. Neoadjuvant CapeOx therapy followed by sphincter-preserving surgery for lower rectal cancer.
2017; 47: 1372-1377 [PMⅠD: 28474202 DOⅠ: 10.1007/s00595-017-1527-5]
 World Journal of Clinical Cases2022年14期
World Journal of Clinical Cases2022年14期
- World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- Hepatopulmonary metastases from papillary thyroid microcarcinoma: A case report