
Catheter-related infections caused by Mycobacterium abscessus in a patient with motor neurone disease: A case report
2022-06-22 08:49:26SuFeiPanYuanYuanZhangXiaoZhenWangJingJingSunShaoLingSongYuRongTangJiLiangWang
World Journal of Clinical Cases 2022年15期
INTRODUCTION
(
) is a rapidly growing non-tuberculous mycobacterium and is ubiquitous in the environment[1]. Recent gene sequence analysis has shown that
can be divided into three different subspecies (
and
)[2].
can cause a variety of clinical manifestations including cutaneous infections, catheter-related infections, post-surgical soft tissue infections, and respiratory diseases[3]. Besides, the incidence of pulmonary non-tuberculous mycobacteria infection has been increasing[4]. Of all the rapidly growing mycobacteria,
is the most common cause of pulmonary infections.
is also one of the mycobacteria that are most often isolated from patients with cystic fibrosis[5]. However,
is resistant to most antibiotics in vitro, and thus is a formidable and difficult-to-treat pathogen[6]. At present, little is known regarding the diagnosis and management of catheter-related
infections due to only a limited number of cases that have been reported[7,8]. Here, we present a case of catheter-related
infections in a patient with motor neurone disease.
CASE PRESENTATION
Chief complaints
On February 6, 2019, a 62-year-old Chinese man presented with mild skin edema at the site of the peripherally inserted central venous catheter (PICC, median cubital vein) which had been inserted for 30 d, without skin redness and inflammatory exudation.
History of present illness
He presented with a two-day history of dyspnea and was admitted to our emergency intensive care unit with a diagnosis of motor neurone disease on January 7, 2019. The patient received comprehensive symptomatic treatment including invasive ventilator-assisted ventilation, pulse oxygen saturation measurement, expectorant, and nutritional supplement.
History of past illness
There was no history of past illness.
Personal and family history
There was no personal and family history.
Physical examination
The main threat of
is its antibiotic resistance.
may be the most resistant species among pathogenic rapidly growing mycobacteria, and its antimicrobial therapy is still a challenge[8]. A previous study showed that the treatment strategy of
infections was the combination of multiple antibiotics, including amikacin, ofloxacin, ciprofloxacin, clarithromycin, and doxycycline[16]. In vitro studies showed that clarithromycin was the most effective of these antibiotics[17]. In the present study, the patient received anti-infective treatment with amikacin plus clarithromycin. In addition, in the case of catheter-related
infections, removal of the catheter is necessary due to the high incidence of relapsing or uncontrolled bacteremia[8]. After the removal of the PICC of our patient, he continued to receive anti-infective treatment with amikacin plus clarithromycin,and his body temperature was maintained at a basic level (35-36.3
C). Unfortunately, the patient gave up treatment due to an unsatisfactory response to respiratory failure and shock, so the long-term treatment results were not obtained.
On February 23, 2019, repeat blood cultures showed positive acid-fast bacilli, and the treatment regimen was adjusted to amikacin plus clarithromycin. On the second day, his body temperature was 35.3
C, his heart rate was 74 beats
minute, white blood cells 7.4 × 10
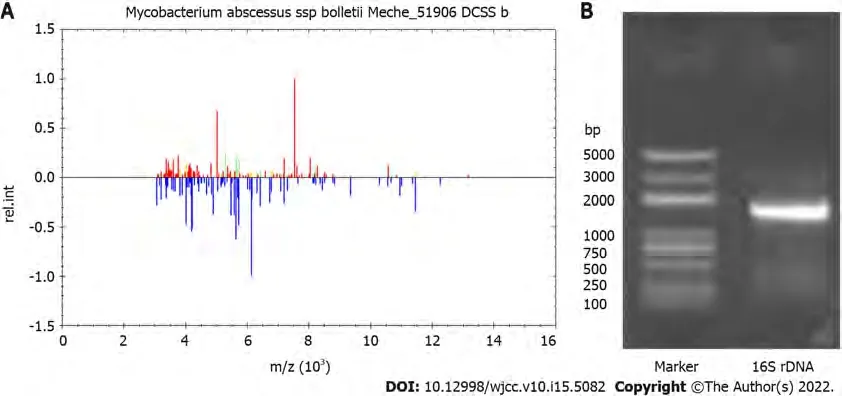
cells/L, and neutrophils 77.6%.After removal of the PICC on March 11, 2019, secretion culture and catheter blood culture were all positive. The blood culture isolate was identified as
by matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) (Figure 2A) and 16S rDNA sequencing(Figure 2B).
Laboratory examinations
Routine blood tests revealed 3.7 × 10
cells/L white blood cells (reference range, 4.0-10.0 × 10
cells/L)and 67.2% neutrophils (reference range, 40%-75%). Catheter and peripheral blood cultures were performed on February 10, 2019. On February 11, 2019, he presented with elevated body temperature(37.1
C), white blood cells (10.2 × 10
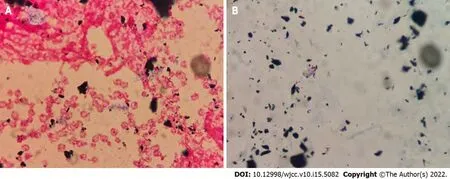
cells/L), and neutrophils (86.7%). The serum procalcitonin and Creactive protein levels was 0.99 ng/mL (reference range, 0-0.05 ng/mL) and 184.9 mg/L (reference range, 0-5 mg/L), respectively. The patient began to receive anti-infective treatment with vancomycin.On February 19, 2019, the blood culture showed positive results during Gram staining (Figure 1A) and acid-fast staining (Figure 1B). The alarm time of catheter blood culture was 10.6 h earlier than that of peripheral blood culture. The treatment regimen of the patient was changed to combination therapy with vancomycin and amikacin.
He got suspended for two days and had two days of in- school detention5 after that. I sometimes wonder if I had not told, would he have done what he said he was going to do? The guys in Colorado seemed pretty normal to a lot of people. The bottom line is, you should never joke around about something as serious as killing6 people. If you do, responsible people have no choice but to have you checked out to ensure everyone else s safety.
FINAL DIAGNOSIS
The patient was finally diagnosed with catheter-related infections caused by
With this new-found wisdom came the freedom to give up trying so very hard to gain the affections of others and to concentrate on finding me. I shattered the family taboo20() of silence about the break-up of my parents marriage. I also felt the need to speak out about the detrimental21 effect I felt my step-parents had had on my life.
TREATMENT
He continued to receive anti-infective treatment with amikacin plus clarithromycin.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
OUTCOME AND FOLLOW-UP
His body temperature was maintained at a basic level (35-36.3
C). Unfortunately, the patient gave up treatment due to an unsatisfactory response to respiratory failure and shock and was discharged on April 13, 2019.
DISCUSSION
Catheter-related bloodstream infection (CRBSI) is the most common complication associated with the use of intravascular catheters[14]. Our patient was a 62-year-old man with motor neurone disease. He had been treated in our hospital many times due to respiratory failure, shock, and electrolyte disorder.During the hospitalization, the patient used PICC for blood controls, which was high-risk factor for CRBSI. No other obvious source of bloodstream infection was found, except for PICC. He presented with fever and mild skin edema at the site of PICC. Routine blood tests revealed elevated white blood cells and neutrophils, procalcitonin, and C-reactive protein. Catheter and peripheral blood cultures of the patient showed positive results during Gram staining and acid-fast staining. The alarm time of catheter blood culture was 10.6 h earlier than that of peripheral blood. He was diagnosed with catheterrelated infections. Gram positive cocci (such as staphylococcus epidermidis, staphylococcus aureus, and enterococcus) have been historically the leading cause of CRBSI[15]. Catheter-related
infection is relatively rare, with limited literature reports[7,8]. In the present study,
was identified by matrix-assisted laser desorption ionization-time of flight mass spectrometry and 16S rDNA sequencing. The patient was finally diagnosed with catheter-related infections caused by
was a terrible and difficult-to-treat mycobacterial pathogen, which is resistant to most antibiotics
[9]. It was ubiquitous in the environment including soil, water, and dust, and survived extreme temperatures and nutritional deprivation[10]. It can cause soft tissue and skin infections after surgical procedures or trauma, pulmonary infections, and disseminated diseases among immunocompromised hosts[11]. Infections in immunocompetent patients tend to be more localized, and usually due to contamination of wounds or abrasions with soil, water, dust, or other materials[12]. While, infections in immunosuppressed patients are often deeper and more diffuse, involving subcutaneous tissue, and leading to the formation of an abscess. Catheter-related infections often occurred in the setting of central venous access devices[13]. In the present study, we present a case of catheter-related
infections in a patient with motor neurone disease.
Physical examination revealed that he was stuporous with a Glasgow coma scale of E1VTM1. His body temperature was 35.0
C, heart rate 66 beats
minute, blood pressure 90/54 mmHg, and respiratory rate 23 breaths
minute.
CONCLUSION
In conclusion, we reported a case of catheter-related
infections in a patient with motor neurone disease. For catheter-related
infection, rapid diagnosis, and timely and adequate antimicrobial therapy are crucial.
Then the hermit looked out and saw how near they were, and he said to the youth, Do you see that? The youth shrieked20 and cried, Ah, good father, it is a fleet of ships, and they are chasing us, and in a few moments they will be upon us
FOOTNOTES
Pan SF, Zhang YY, and Wang JL designed the research and wrote the paper; Pan SF, Zhang YY,Wang XZ, Sun JJ, Song SL, and Tang YR collected all the data related to the case report; Wang JL supervised the report; all authors have read and approved the final manuscript.
The authors declare that they have no conflict of interest.
Written informed consent was obtained from the patient.
Miraculously4 he managed to reach his friend, hoisted5() him onto his shoulder, and brought him back to their company s trench. As the two of them tumbled in together to the bottom of the trench, the officer checked the wounded soldier, then looked kindly6 at his friend. I told you it wouldn t be worth it, he said. Your friend is dead, and you are mortally wounded.
Then Grannonia knelt down before the fox, and begged him in her sweetest way to catch the birds for her and procure30 their blood, promising31 at the same time to reward him richly
One day she was sitting on the banks of a stream bewailing her wretched lot, when she suddenly caught sight of herself in the water. Her hair and part of her face was quite concealed25 by the ass’s head, which was drawn right over like a hood26, and the filthy27 matted skin covered her whole body. It was the first time she had seen herself as other people saw her, and she was filled with shame at the spectacle. Then she threw off her disguise and jumped into the water, plunging28 in again and again, till she shone like ivory. When it was time to go back to the farm, she was forced to put on the skin which disguised her, and now seemed more dirty than ever; but, as she did so, she comforted herself with the thought that to-morrow was a holiday, and that she would be able for a few hours to forget that she was a farm girl, and be a princess once more.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Su-Fei Pan 0000-0003-3898-3607; Yuan-Yuan Zhang 0000-0002-6002-6056; Xiao-Zhen Wang 0000-0001-6442-2454; Jing-Jing Sun 0000-0003-4045-9724; Shao-Ling Song 0000-0002-1077-8890; Yu-Rong Tang 0000-0002-5962-0664; Ji-Liang Wang 0000-0002-8650-3076.
And now her two sisters found her to be that fine, beautiful lady whom they had seen at the ball. They threw themselves at her feet to beg pardon60 for all the ill- treatment they had made her undergo. Cinderella took them up, and, as she embraced them, cried that she forgave them61 with all her heart, and desired them always to love her.
Fan JR
A
Fan JR
1 Rodríguez-García R, Espina Angulo MJ,Escudero Augusto D. Cutaneous infection with Mycobacterium abscessus.
2018; 44: 2292-2293 [PMID: 29974168 DOI: 10.1007/s00134-018-5284-8]
2 Aziz DB, Low JL, Wu ML, Gengenbacher M, Teo JWP, Dartois V, Dick T. Rifabutin Is Active against Mycobacterium abscessus Complex.
2017; 61 [PMID: 28396540 DOI: 10.1128/AAC.00155-17]
3 Gutiérrez AV, Viljoen A, Ghigo E, Herrmann JL, Kremer L. Glycopeptidolipids, a Double-Edged Sword of the
Complex.
2018; 9: 1145 [PMID: 29922253 DOI: 10.3389/fmicb.2018.01145]
4 Benwill JL, Wallace RJ Jr. Mycobacterium abscessus: challenges in diagnosis and treatment.
2014;27: 506-510 [PMID: 25268925 DOI: 10.1097/QCO.0000000000000104]
5 Petrini B. Mycobacterium abscessus: an emerging rapid-growing potential pathogen.
2006; 114: 319-328 [PMID:16725007 DOI: 10.1111/j.1600-0463.2006.apm_390.x]
6 Koh WJ, Jeon K, Lee NY, Kim BJ, Kook YH, Lee SH, Park YK, Kim CK, Shin SJ, Huitt GA, Daley CL, Kwon OJ.Clinical significance of differentiation of Mycobacterium massiliense from Mycobacterium abscessus.
2011; 183: 405-410 [PMID: 20833823 DOI: 10.1164/rccm.201003-0395OC]
7 Lee SA, Raad II, Adachi JA, Han XY. Catheter-related bloodstream infection caused by Mycobacterium brumae.
2004; 42: 5429-5431 [PMID: 15528764 DOI: 10.1128/JCM.42.11.5429-5431.2004]
8 Laurens C, Héry-Arnaud G, Chiron R, Oziol E, Jean-Pierre H, Bouzinbi N, Vande Perre P, Ba?uls AL, Godreuil S.Sacroiliitis secondary to catheter-related bacteremia due to Mycobacterium abscessus (sensu stricto).
2014; 13: 9 [PMID: 24479655 DOI: 10.1186/1476-0711-13-9]
9 Griffith DE, Brown-Elliott BA, Benwill JL, Wallace RJ Jr. Mycobacterium abscessus. "Pleased to meet you, hope you guess my name...".
2015; 12: 436-439 [PMID: 25643064 DOI: 10.1513/AnnalsATS.201501-015OI]
10 Mooren VHJF, Bleeker MWP, van Ingen J, Hermans MHA, Wever PC. Disseminated
infection in a peritoneal dialysis patient.
2017; 9: 6-7 [PMID: 28529886 DOI: 10.1016/j.idcr.2017.05.001]
11 Bechara C, Macheras E, Heym B, Pages A, Auffret N. Mycobacterium abscessus skin infection after tattooing: first case report and review of the literature.
2010; 221: 1-4 [PMID: 20558973 DOI: 10.1159/000313974]
12 Drage LA, Ecker PM, Orenstein R, Phillips PK, Edson RS. An outbreak of Mycobacterium chelonae infections in tattoos.
2010; 62: 501-506 [PMID: 19733936 DOI: 10.1016/j.jaad.2009.03.034]
13 Xie O, Khan S, Globan M, Lea K, Bajel A, Slavin M. Mycobacterium abscessus bloodstream infection: Unexpected catheter tunnel infection localized by PET/CT.
2019; 21: e13147 [PMID: 31306546 DOI:10.1111/tid.13147]
14 Ruiz-Ruigómez M, Fernández-Ruiz M, San-Juan R, López-Medrano F, Orellana Má, Corbella L, Rodríguez-Goncer I,Hernández Jiménez P, Aguado JM. Impact of duration of antibiotic therapy in central venous catheter-related bloodstream infection due to Gram-negative bacilli.
2020; 75: 3049-3055 [PMID: 32591804 DOI:10.1093/jac/dkaa244]
15 Tarpatzi A, Avlamis A, Papaparaskevas J, Daikos GL, Stefanou I, Katsandri A, Vasilakopoulou A, Chatzigeorgiou KS,Petrikkos GL. Incidence and risk factors for central vascular catheter-related bloodstream infections in a tertiary care hospital.
2012; 35: 429-437 [PMID: 23109010]
16 Kameyama H, Mori Y, Kimura T, Sugishita C, Adachi T, Sonomura K, Kusaba T, Tanda S, Kishimoto N, Okigaki M,Hatta T, Matsubara H. A case report of Mycobacterium abscessus peritonitis in a peritoneal dialysis patient.
2007; 11: 449-451 [PMID: 18028172 DOI: 10.1111/j.1744-9987.2007.00526.x]
17 Ellis EN, Schutze GE, Wheeler JG. Nontuberculous mycobacterial exit-site infection and abscess in a peritoneal dialysis patient. A case report and review of the literature.
2005; 20: 1016-1018 [PMID: 15880270 DOI:10.1007/s00467-005-1870-4]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report