Comments on "Review of the role of diagnostic modalities and imaging findings in the COVID-19 pandemic"
2022-06-01 09:54:38SaiSwarupaVulasalaDheerajGopireddyPriyaBhosaleMayurVirarkar
World Journal of Radiology 2022年2期
TO THE EDITOR
We read with interest the article published in the World Journal of Radiology by Pal
[1]on the depiction of radiological findings in identifying and predicting coronavirus disease 2019(COVID-19)patient patterns.We would like to commend the authors for this vital article encompassing the pathophysiology and evidence-based review of COVID-19 severity scoring systems on chest X-ray(CXR),computed tomography(CT),and lung ultrasound(LUS).The authors outlined the artificial intelligence(AI)aspect of the diagnostic process and its importance in supporting human resources during the pandemic.
Although reverse transcriptase-polymerase chain reaction(RT-PCR)is the standard work-up for a specific diagnosis,it is limited by sample quality,laboratory errors,ribonucleic acid(RNA)stability,and variable sensitivity[2].RT-PCR involves two steps:(1)Reverse transcription;and(2)Quantitative real time polymerase chain reaction.It can detect RNA by using either RNA or deoxyribonucleic acid(DNA)as positive controls.Most of the commercial kits adopt DNA as control in fear of RNA degradation by ribonucleases(RNases).However,DNA kits cannot report failed reverse transcriptase step,thus resulting in high false negative rates(40%)and variable sensitivity[3].To avoid this concern,appropriate controls are necessary for viral RNA detection.Also,a negative RT-PCR requires repetition of the test in cases of clinical suspicion[4].In contrast,imaging is a rapid and reliable procedure to evaluate suspicion of COVID-19 in individuals presenting with cough,dyspnea,and fatigue.At the beginning of the pandemic,there was a distinct and contentious discussion on the role and importance of radiology as part of the clinical management of COVID-19.
But he did remember, and a few years later he told his younger brother, Dave, about the all-leather, NFL regulation, 1963 Chicago Bears-inscribed football that was special and kept somewhere in the garage
CXR is a readily accessible and inexpensive modality in the majority of clinical settings.It is helpful for triage among suspected COVID-19 individuals in the emergency department[5].Peripheral predominant hazy opacification,bilateral lower lobe consolidation,and air space opacities similar to acute respiratory distress syndrome are the characteristic findings of COVID-19 on CXR.Pleural effusion,nodules,and pneumothorax are also unusual findings that can be discerned in COVID-19 patients[6].
Although, I do sincerely like to have a plan better than see what happens worked out when flying—it really isn t such a bad life strategy. All too often, I would see people chasing their goals halt frozen with inaction just because they don t have all the necessary pieces or guaranteed result when in reality—they will never have all the pieces. Success will never be guaranteed. The best thing that you can do is just get up in the air, and see what happens. Sometimes adjustments would be made in the air, or shall we say, in the middle of the process.
A 12-zone scoring system is used to quantify and predict the severity of lung involvement.Individuals are classified as normal,mild,moderate,and severely infected,with scores of 0,1-5,6-14,and ≥ 15,respectively.A cutoff score of 8 of 36 is 91% sensitive in predicting COVID-19 diagnosis.Hence LUS may be used as a screening tool,but in conjunction with other imaging modalities due to its ineffective differentiation between acute ongoing infection and recovery[1,2].
Familiarity with the COVID-19 imaging findings was essential for radiologists working during the pandemic.Even though the disease spread is controlled currently,the discovery of newer virus strains highlights the importance of strategies such as increasing work capacity and imaging capabilities that might be helpful during a future unanticipated outbreak.
CT imaging is the preferred diagnostic modality,given its high sensitivity(94%)[1].However,the specificity of CT ranges from 25% to 80%[1].Lateralized,bilateral,multifocal,basilar and peripheral predominance and peripheral ground-glass opacities are the classical CT findings of COVID-19 pneumonia.Non-classical features include subsegmental vessel engorgement,“atoll sign,” reticular opacifications,subpleural curvilinear opacifications,and bilateral hilar lymphadenopathy.All these findings are well illustrated by Pal
[1].
When he approached the bed the King spake to him: Most trusty John, I feel my end is drawing near, and I could face it without a care were it not for my son
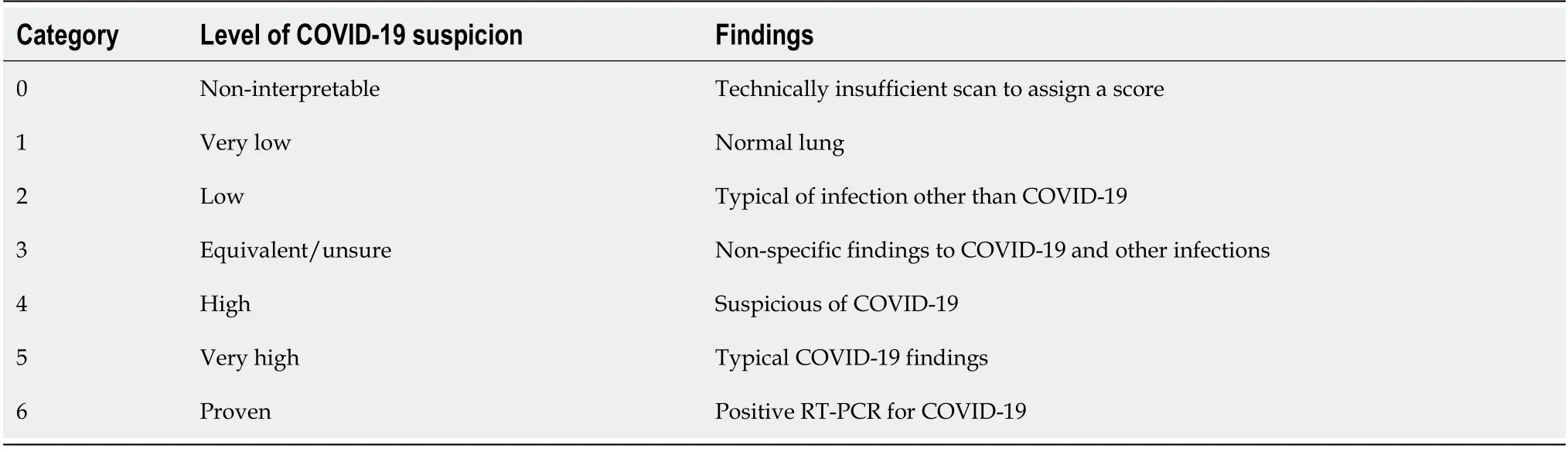
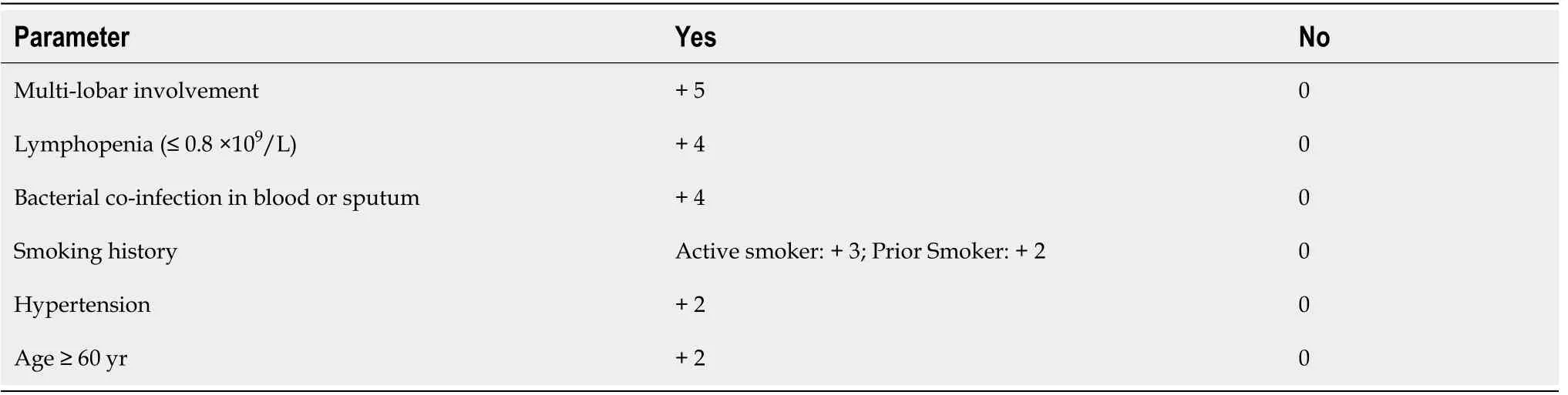
COVID-19 reporting and data system(CO-RADS)(Table 3)and MuLBSTA(multilobular infiltration,hypo-lymphocytosis,bacterial coinfection,smoking history,hypertension,and age)(Table 4)scoring systems aid in the identification of the lung involvement and prognosis in suspected COVID-19 patients.Pal
[1]described that CO-RADS and MuLBSTA have a sensitivity of 61% and 65.1%,and specificity of 81% and 95.4%,respectively.The main drawbacks of CT in clinical setting are:radiation exposure,the need to transfer the patient to the imaging room,and availability.

Vulasala SSR,Gopireddy DR,Bhosale P,Virarkar MK have equal contributions;all authors have read and approved the final manuscript.
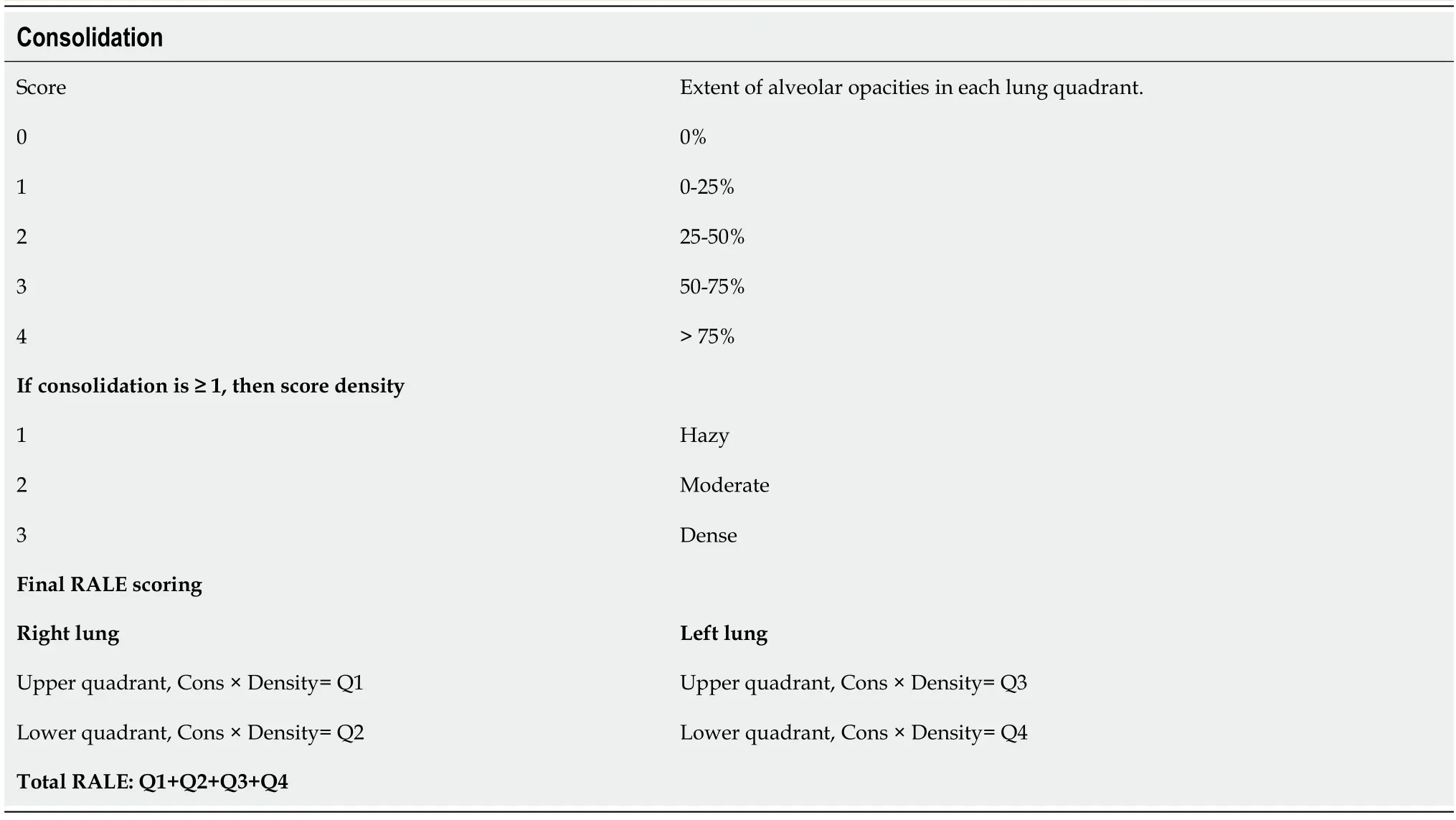
Radiological assessment of lung edema(RALE)(Table 1)and Brixia score(Table 2)are the CXR-based grading systems in practice to predict the severity and prognosis of COVID-19 disease.According to a study by Au-Yong
[7],RALE and Brixia scores have correlations of 0.87 and 0.86,respectively,in predicting patient outcomes.Individuals with high scores(RALE > 25 and Brixia > 11)have increased chances of intensive care unit admission or death within 60 days after diagnosis.As acknowledged by Pal
[1]the usage of CXR has been limited by lower sensitivity(56%)and specificity(60%).
Although the role of magnetic resonance imaging,Fluorodeoxyglucose positron emission tomography,CT pulmonary angiography,and point-of-care echocardiography is limited in COVID-19,they may help detect complications such as myocarditis,cardiomyopathy,right ventricular dilatation,and pulmonary embolism and monitor the treatment response.AI is an algorithm-based entity that allows rapid diagnosis and enhances a health system’s capability.AI COVID-19 algorithm has a sensitivity,specificity,and accuracy of 84%,93%,and 90.8%,respectively.AI-based deep learning technology has detected COVID-19 on CT with an area under the receiver operating characteristic curve of 0.96 and sensitivity and specificity of 90% and 96%,respectively[11].Wehbe
[12]compared the performance of AI and radiologists and reported similar diagnostic accuracy of 82% and 81%,respectively.Hence,AI has the ability to assist radiologists in prompt diagnosis and to improve workflow efficiency.
The next morning she was asked how she had slept. Oh, very badly indeed! 8 she replied. I have scarcely closed my eyes the whole night through. I do not know what was in my bed, but I had something hard under me, and am all over black and blue.9 It has hurt me so much!
FOOTNOTES
Lung ultrasound(LUS)may assist physicians in assessing the disease severity with sensitivity and specificity of 65%-76.9% and 72.7%-77.1%,respectively[1].It identifies subtle lung findings in the periphery which remain hidden in majority of CXR[8].In addition,the findings of COVID-19 pneumonia on LUS correlate well with CT findings[9,10].Hence LUS can be employed in the common and standard practice.LUS is advantageous as it eliminates the radiation risk and resource consumption of CXR and CT,if the patients require daily monitoring of lung status.It also overcomes the limitations of CT by its portability and accessibility at bedside with great learning curve.B-line artifacts,subpleural consolidations,pleural irregularities,and patchy opacities can be seen on the LUS of COVID-19-infected patients.The presence of B-lines indicates parenchymal involvement,and they increase proportionately with the disease,resulting in “white lungs”[2].With recuperation from illness,B-lines are replaced with A-lines,which represent normal lung surface.Subpleural consolidation specifies the inflammatory changes;however,these findings may last for several weeks after recovery.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
The authors declare they have no conflicts of interest.
United States
Sai Swarupa R Vulasala 0000-0002-9387-3673;Dheeraj R Gopireddy 0000-0001-8441-7804;Priya Bhosale 0000-0003-4014-4941;Mayur K Virarkar 0000-0002-5825-3102.
Xing YX
As we talked, I could tell my initial assessment8 was correct. These people were survivors9 of the Holocaust10 who had gathered at the synagogue to see if they could find someone, anyone, who might know of a relative or friend who had also survived. Because there was no civilian11 mail service from Austria to the rest of the world, these gatherings12 were the only way the survivors could hope to hear news of their families.
A
Xing YX
1 Pal A,Ali A,Young TR,Oostenbrink J,Prabhakar A,Deacon N,Arnold A,Eltayeb A,Yap C,Young DM,Tang A,Lakshmanan S,Lim YY,Pokarowski M,Kakodkar P.Comprehensive literature review on the radiographic findings,imaging modalities,and the role of radiology in the COVID-19 pandemic.
2021;13:258-282[PMID:34630913 DOI:10.4329/wjr.v13.i9.258]
2 Skoczyński S,Buda N,Mendrala K,Górecki T,Kucewicz-Czech E,Krzych ?,Koszutski T,Darocha T.Lung ultrasound may improve COVID-19 safety protocols.
2021;13:2698-2704[PMID:34164162 DOI:10.21037/jtd-21-295]
3 Luo G,Zhang J,Zhang S,Hu B,Hu L,Huang Z.High-quality RT-PCR with chemically modified RNA controls.
2021;224:121850[PMID:33379066 DOI:10.1016/j.talanta.2020.121850]
4 Arevalo-Rodriguez I,Buitrago-Garcia D,Simancas-Racines D,Zambrano-Achig P,Del Campo R,Ciapponi A,Sued O,Martinez-García L,Rutjes AW,Low N,Bossuyt PM,Perez-Molina JA,Zamora J.False-negative results of initial RT-PCR assays for COVID-19:A systematic review.
2020;15:e0242958[PMID:33301459 DOI:10.1371/journal.pone.0242958]
5 Reeves RA,Pomeranz C,Gomella AA,Gulati A,Metra B,Hage AN,Lange S,Parekh M,Donuru A,Lakhani P,Sundaram B.Performance of a Severity Score on Admission Chest Radiography in Predicting Clinical Outcomes in Hospitalized Patients With Coronavirus Disease(COVID-19).
2021;217:623-632[PMID:33112201 DOI:10.2214/AJR.20.24801]
6 Jacobi A,Chung M,Bernheim A,Eber C.Portable chest X-ray in coronavirus disease-19(COVID-19):A pictorial review.
2020;64:35-42[PMID:32302927 DOI:10.1016/j.clinimag.2020.04.001]
7 Au-Yong I,Higashi Y,Giannotti E,Fogarty A,Morling JR,Grainge M,Race A,Juurlink I,Simmonds M,Briggs S,Cruikshank S,Hammond-Pears S,West J,Crooks CJ,Card T.Chest Radiograph Scoring Alone or Combined with Other Risk Scores for Predicting Outcomes in COVID-19.
2021;210986[PMID:34519573 DOI:10.1148/radiol.2021210986]
8 Boero E,Schreiber A,Rovida S,Vetrugno L,Blaivas M.The role of lung ultrasonography in COVID-19 disease management.
2020[PMID:32838389 DOI:10.1002/emp2.12194]
9 Skopljanac I,Ivelja MP,Barcot O,Brdar I,Dolic K,Polasek O,Radic M.Role of Lung Ultrasound in Predicting Clinical Severity and Fatality in COVID-19 Pneumonia.
2021;11[PMID:34442401 DOI:10.3390/jpm11080757]
10 Lieveld AWE,Kok B,Azijli K,Schuit FH,van de Ven PM,de Korte CL,Nijveldt R,van den Heuvel FMA,Teunissen BP,Hoefsloot W,Nanayakkara PWB,Bosch FH.Assessing COVID-19 pneumonia-Clinical extension and risk with point-ofcare ultrasound:A multicenter,prospective,observational study.
2021;2:e12429[PMID:33969350 DOI:10.1002/emp2.12429]
11 Szabó IV,Simon J,Nardocci C,Kardos AS,Nagy N,Abdelrahman RH,Zsarnóczay E,Fejér B,Futácsi B,Müller V,Merkely B,Maurovich-Horvat P.The Predictive Role of Artificial Intelligence-Based Chest CT Quantification in Patients with COVID-19 Pneumonia.
2021;7:697-710[PMID:34842822 DOI:10.3390/tomography7040058]
12 Wehbe RM,Sheng J,Dutta S,Chai S,Dravid A,Barutcu S,Wu Y,Cantrell DR,Xiao N,Allen BD,MacNealy GA,Savas H,Agrawal R,Parekh N,Katsaggelos AK.DeepCOVID-XR:An Artificial Intelligence Algorithm to Detect COVID-19 on Chest Radiographs Trained and Tested on a Large U.S.Clinical Data Set.
2021;299:E167-E176[PMID:33231531 DOI:10.1148/radiol.2020203511]
13 Warren MA,Zhao Z,Koyama T,Bastarache JA,Shaver CM,Semler MW,Rice TW,Matthay MA,Calfee CS,Ware LB.Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS.
2018;73:840-846[PMID:29903755 DOI:10.1136/thoraxjnl-2017-211280]