
Multiple different remote epidural hematomas after craniotomy:A case report
2022-03-18 02:16:32QiangHeChuanYuanTaoRuiHongFuChaoYou
World Journal of Clinical Cases 2022年6期
lNTRODUCTlON
Postoperative hemorrhage includes intracerebral hematoma(ICH),subdural hematoma,and extradural hematoma(EDH),which are serious complications after craniotomy.EDH is one of the most frequent and devastating complications.It may occur in supratentorial,infratentorial,ipsilateral,and even contralateral sites of the operative area[1,2].As a specific subset of EDH after craniotomy,multiple remote EDHs are very rare.In this study,we present a 21-year-old woman who developed three remote EDHs in different sites after craniotomy.
CASE PRESENTATlON
Chief complaints
A 21-year-old woman visited the emergency department and was admitted to the Neurosurgery Department.She complained of headache and vomiting for 1 mo,and rapid vision loss for 1 wk.
History of present illness
The patient had a headache and recurrent vomiting,along with rapid vision loss.
History of past illness
The patient had no significant medical history.
Personal and family history
Neither the patient nor her family members had special medical history.
I was scared because no one had ever said anything like that to me before. I found out when talking to other friends that he also bragged4 about this to other people. My friends told me that I should tell an adult what he had said, but I was too scared and I made them promise not to tell anyone either.
Physical examination
The patient was conscious.The extremities were moved as instructed.General sensory was normal.The positive sign was blurred binocular vision.
He tried to reason with his son, and told him that during all these years he had been looking forward to his return, in order to resign his throne and its cares, which pressed so heavily upon him
Laboratory examinations
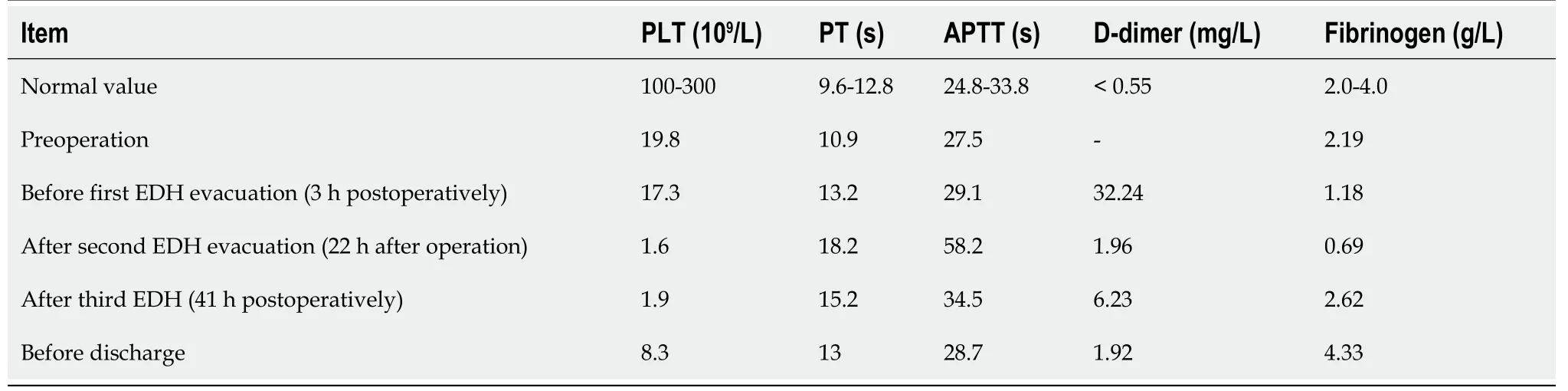
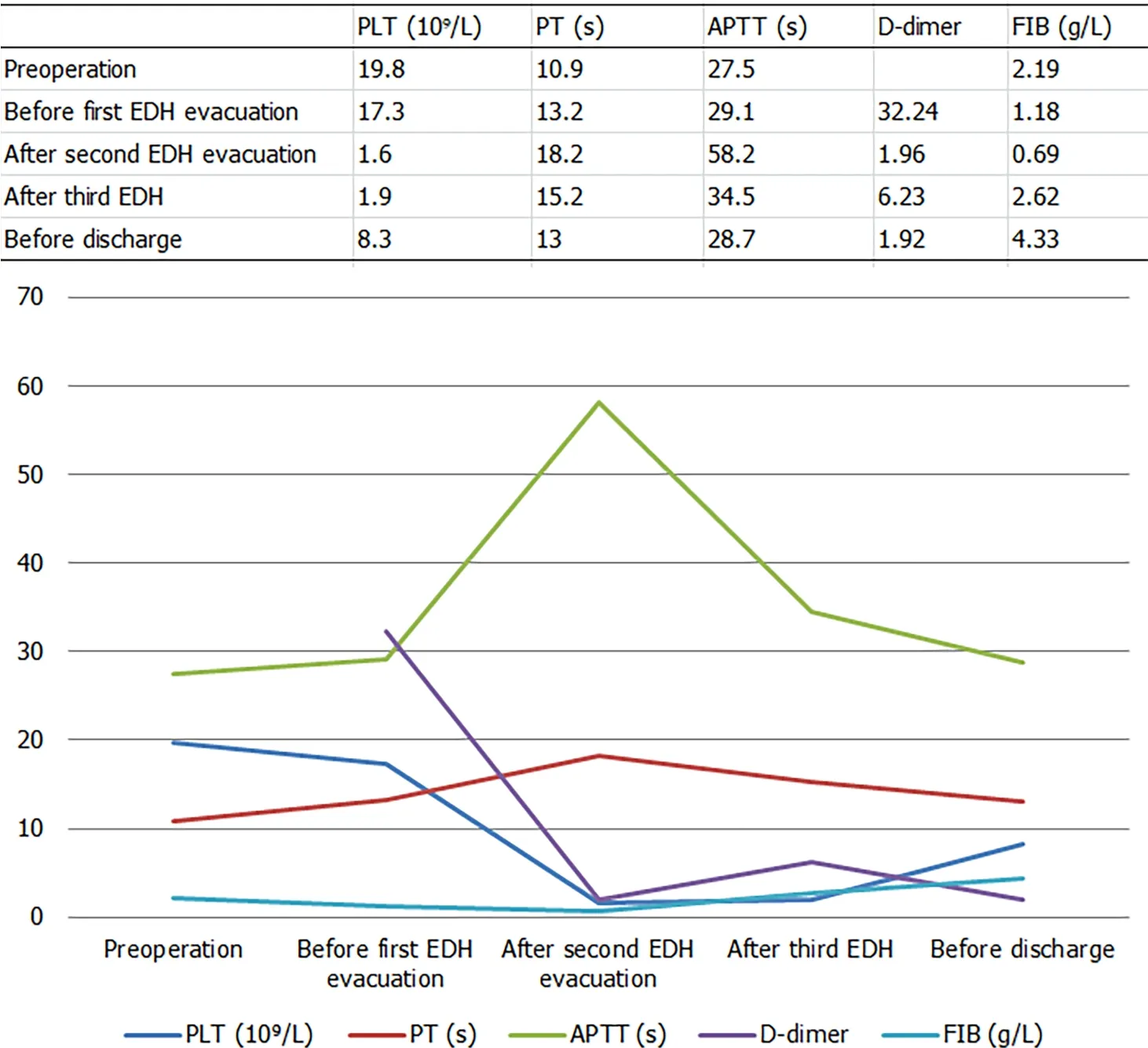
The blood test results were within normal limits before surgery.The laboratory examination results in the whole treatment process are shown in Figure 1 and Table 1.
Imaging examinations
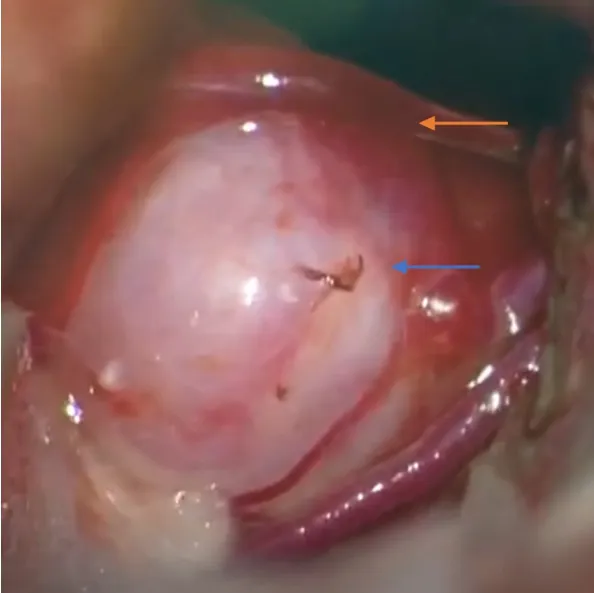
Under the neuro-electrophysiological monitoring,a triangular approach was performed.The cystic mass was dissected,and then yellow fluid was released from the cyst.However,a small artery was observed below the cyst cavity.In addition,a red bulge was observed and considered an aneurysm,which had a drainage vein(Figure 3).Therefore,aneurysm clipping and vascular malformation resection were performed.Neuro-electrophysiological monitoring revealed a decline in the left lower limb.The entire procedure lasted 6.5 h.
MULTlDlSClPLlNARY EXPERT CONSULTATlON
The patient was diagnosed with a right thalamic tumor before surgery.
FlNAL DlAGNOSlS
The final diagnosis was a solid cystic tumor,right posterior cerebral artery aneurysm,vascular malformation in the thalamus,and multiple remote EDHs.
TREATMENT
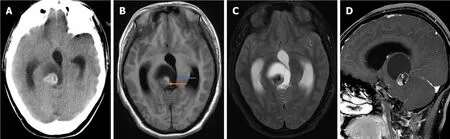
Computerized tomography(CT)revealed a solid cystic tumor in the right thalamus(Figure 2A).Brian magnetic resonance imaging(MRI)showed a solid cystic tumor in the right thalamus and midbrain(Figure 2B-D).
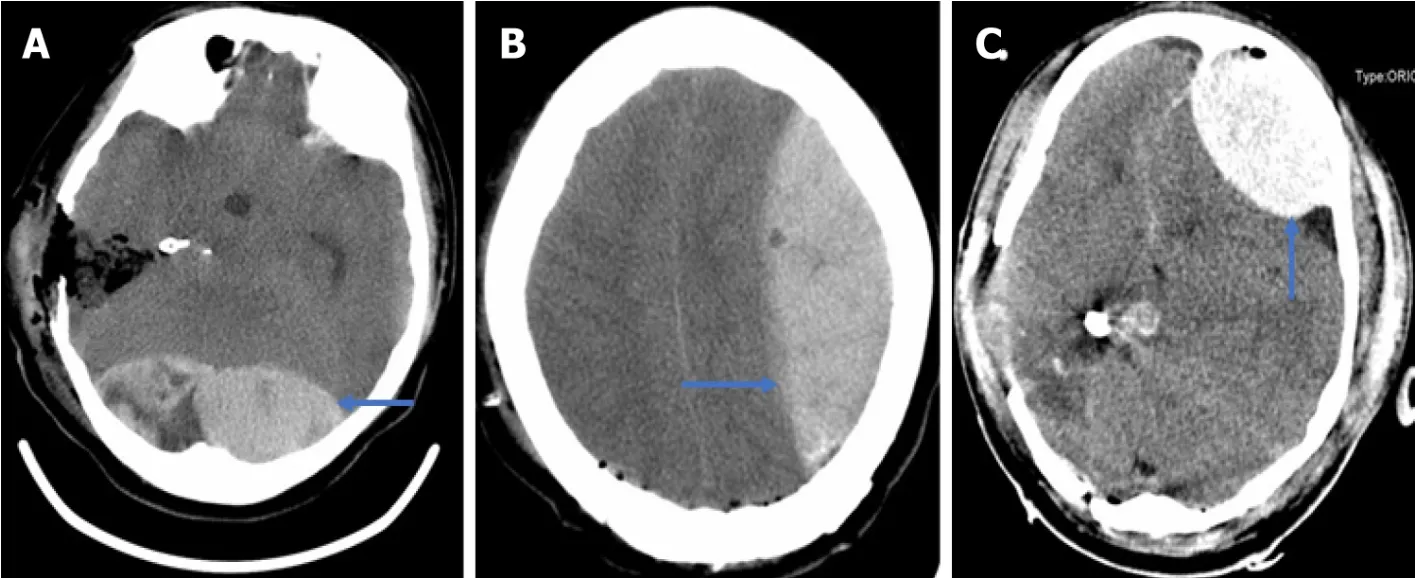
Because the patient did not wake up from anesthesia after 3 h,CT confirmed the first EDH of about 130 mL in the occipital(Figure 4A).Hematoma evacuation was performed.However,the second EDH after 22 h and the third EDH after 41 h developed in the left frontotemporal and the frontal regions(Figure 4B and C).Familial members consented to the second hematoma evacuation but refused the third.
You C and Tao CY were the patient’s neurosurgeons,reviewed the literature,and were responsible for the revision of the manuscript;He Q and Fu RH contributed to manuscript drafting and data collection;all authors issued final approval for the version to be submitted.
OUTCOME AND FOLLOW-UP
All authors declare that they have no conflict of interest to disclose.
DlSCUSSlON
Remote EDH is defined as EDH at a site away from the primary surgical site.Although EDH accounts for 20%[1]among remote site bleeding[3,4],only 12% required surgical intervention[2].According to published articles,only three cases of multiple postoperative EDHs were reported.Wolfsberger[5]presented a patient with four EDHs in the supratentorial area after surgery for the fourth ventricular choroid plexus papilloma.Lim[6]and Gaurav Tyagi[7]reported two EDHs in the supratentorial area after posterior fossa surgery.However,our patient had three remote EDHs in different locations,including supratentorial and infratentorial regions.
Informed written consent was obtained from the patient for the publication of this case report and any accompanying images.
The pins of a Mayfield head holder may be a reason[11],which may damage the transverse sinus.However,no evidence of fracture was found at the pin sites.Therefore,the cause was ruled out.Age may be a factor for the first EDH because the not-tight adhesion between the dura and skull is more frequent in young people[12,13].Our patient was a 21-year-old woman.EDH may also result from jugular vein compression because of the extended neck position and intraoperative rotation[14,15].The patient was positioned in a supine gesture with the head rotation about 65 degrees during surgery,which could lead to obstruction of cerebral venous return.
Coagulopathy is a possible explanation.Our patient had a normal coagulation function before surgery.For the second EDH,consumptive coagulopathy after tumor resection and first EDH might disturb coagulation.The disturbance presented increasing prothrombin time,activated partial thromboplastin time,and international normalized ratio and decreasing fibrinogen,combining with drastically declining platelets.The volume of the first EDH was 130 mL.After the first EDH hematoma evacuation,changes in ICP between the supratentorial and infratentorial regions led to the second left supratentorial EDH.The third EDH could also be attributed to those hypotheses.Thrombocytopenia may play an important role in the third bleeding.Platelet counts in our patients decreased drastically,although the patient was infused with platelets.Unfortunately,a thromboelastogram test was not performed.Decreased factor XIII activity and factor X deficiency may result in EDH[16-18],but the patient and her family did not have this medical history.
The Caliph, who liked to have old manuscripts in his library, even though he could not read them, purchased the scroll and the box, and dismissed the pedlar
We noticed that no definitive source of ooze could be identified during the two hematoma evacuations.There was no visible bleeding on the edge of the dura mater.In the first EDH,the pupil change was noted in time.CT confirmed the EDH.In the third and second EDH,the assessment of CT scan was also a matter of time.Accordingly,early computed tomography scanning of the brain after surgery should be highlighted.Postoperative pupil changes and not waking up from anesthesia are indications for early CT scanning.
CONCLUSlON
The king made no difficulties about it, and even gave his finest rubies14 and diamonds to ornament15 the dress, which was so dazzling, when finished, that it could not be looked at save through smoked glasses!
Although multiple remote EDH is an uncommon complication,attention should be paid to it.Understanding the mechanism of the complication,sufficient preparation and evaluation before an operation,and meticulous operation during surgery are the keys to preventing postoperative EDH,especially for acute onset.Intraoperative administration of ICP should be meticulous.It is important to monitor the ICP and nerve function after the operation.When the pupil change and the patient cannot recover from anesthesia in time,early CT scanning of the brain should be a priority.
ACKNOWLEDGEMENTS
We appreciate the patient and her family members contributing to this medical study.
The powerful contrast between God s way of treating people and Death s manner of making no distinctions based on social class reflected growing skepticism about the comforts of religion. Social justice would have to come through means other than piousness27 and prayer. (196)
FOOTNOTES
It happened that, a little before this time, the princess had been sent away for her health to another remote province; and whilst she was there her old friend, the governor s wife, had begged her to come and stay with them as soon as she could
How delighted the witch was when she found the clothes all finished! The next time Prince Ring came to see her she gave them to him, and he paid her many compliments on her skilful23 work, after which he took leave of her in the most friendly manner
The drastic fluctuation of ICP is a trigger point of postoperative remote ICH[4,8,9].The fluctuation may result from tumor resection and/or rapid release of cerebrospinal fluid(CSF)and sac fluid.Patients with ventricular drainage systems have a higher incidence of remote ICH than those without[10].The fast decline of ICP results in negative pressure in a distant area.This fluctuation causes the rupture of blood vessels.With the increasing hematoma caused by vessel rupture,the dura and skull are separated.The phenomenon aggravates hematoma expansion.The above points are a vicious cycle.In our case,the lesion was in the thalamus and midbrain with a posterior cerebral artery.Angiographic assessment should be necessary but was not performed.Because the acute onset occurred and the lesion compressed the aqueduct,the patient had acute obstructive hydrocephalus.Those are special factors for the first occipital EDH.
The patient’s family members refused further treatment and asked for discharging.The patient died.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Qiang He 0000-0003-0142-7615;Chuan-Yuan Tao 0000-0002-1863-5392;Rui-Hong Fu 0000-0003-4756-2601;Chao You 0000-0003-1931-6315.
Ma YJ
From then on, we both talked incessantly5. I discovered that they were heading to the same orphanage to be met by the same coordinator6. We became fast friends. I whispered a prayer of thanks to God for answering my earlier prayer.
Wang TQ
Ma YJ
 World Journal of Clinical Cases2022年6期
World Journal of Clinical Cases2022年6期
- World Journal of Clinical Cases的其它文章
- Vaginal enterocele after cystectomy:A case report
- Acute kidney injury due to intravenous detergent poisoning:A case report
- Bilateral pneumothorax and pneumomediastinum during colonoscopy in a patient with intestinal Behcet’s disease:A case report
- Successful embolization of an intrahepatic portosystemic shunt using balloon-occluded retrograde transvenous obliteration:A case report
- lmplant site development using titanium plate and platelet-rich fibrin for congenitally missed maxillary lateral incisors:A case report
- Primary duodenal dedifferentiated liposarcoma:A case report and literature review