
Hoffa’s fracture in an adolescent treated with an innovative surgical procedure:A case report
2022-03-15 07:12:30ZuXinJiangPanWangShunXinYeXiaoPingXieChunXiuWangYueWang
World Journal of Clinical Cases 2022年4期
INTRODUCTION
Hoffa fracture,a fracture of the femoral condyle in the coronal plane involving one or both of the condyles,was first described in 1904 by Hoffa[1].The conventional classification system includes the three subtypes proposed by Letenneur[2].The diagnosis of these fractures is challenging,since they are easily misdiagnosed and missed in anteroposterior X-rays,because the unfractured condylar part of the femur can obscure the fractured condyle[3].Therefore,when Hoffa's fracture is suspected,further computed tomography (CT) is necessary.This is an uncommon injury in adults,which is even rarer in adolescents.It accounts for 8.7% to 13% of distal femoral fractures[4].There are no data on the potential injury mechanism.Although in children and individuals with osteoporosis,low-energy trauma can produce the lesion,the main cause of a Hoffa fracture is a high-energy injury (,a traffic collisions or a fall)[5,6].Surgical treatment,anatomical reduction,and stable fixation are recommended to reduce the rate of complications,such as arthritis,nonunion,and osteonecrosis[7].However,as far as the literature reports,there is no optimal surgical approach and fixation method[3].Hence,we present the case of an adolescent girl with a medial condyle fracture (type III) of the distal femur,which was successfully managed with an innovative surgical procedure.We hope to provide a new possibility for the treatment of similar fractures,and further improve their management.
CASE PRESENTATION
Chief complaints
A 16-year-old girl presented to our orthopedic emergency department with sustained pain following a right knee injury in a sprint race.
History of present illness
She felt persistent pain in her right knee and was unable to walk normally.She had no other symptoms,including dizziness,headache,chest tightness,and abdominal pain.
History of past illness
She had no other history of past illnesses.
Personal and family history
She had no genetic or familial disease history.
Physical examination
And when they reached the shore, what an unpacking5 there was! For this was a noted6 fishing ground, and here they would live, in little wooden huts, till autumn and bad weather came round again
On examination,the patient's vital signs were stable.Right knee was swollen and tender with bone crepitation and decreased range of motion.There were no open wounds or distal neurovascular deficits.
Laboratory examinations
All the servants stood in the courtyard and saw them mount their steeds, and here by chance came the third brother; for the squire had three sons, but nobody counted him with his brothers, for he was not so learned as they were, and he was generally called Blockhead-Hans
Laboratory examination revealed no obvious abnormality.
Imaging examinations
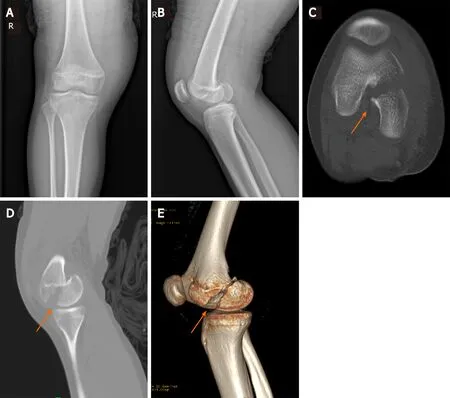
Knee radiographs and CT images confirmed a coronal plane fracture of the posterior part of the medial femoral condyle with epiphyseal injury (Figure 1).
FINAL DIAGNOSIS
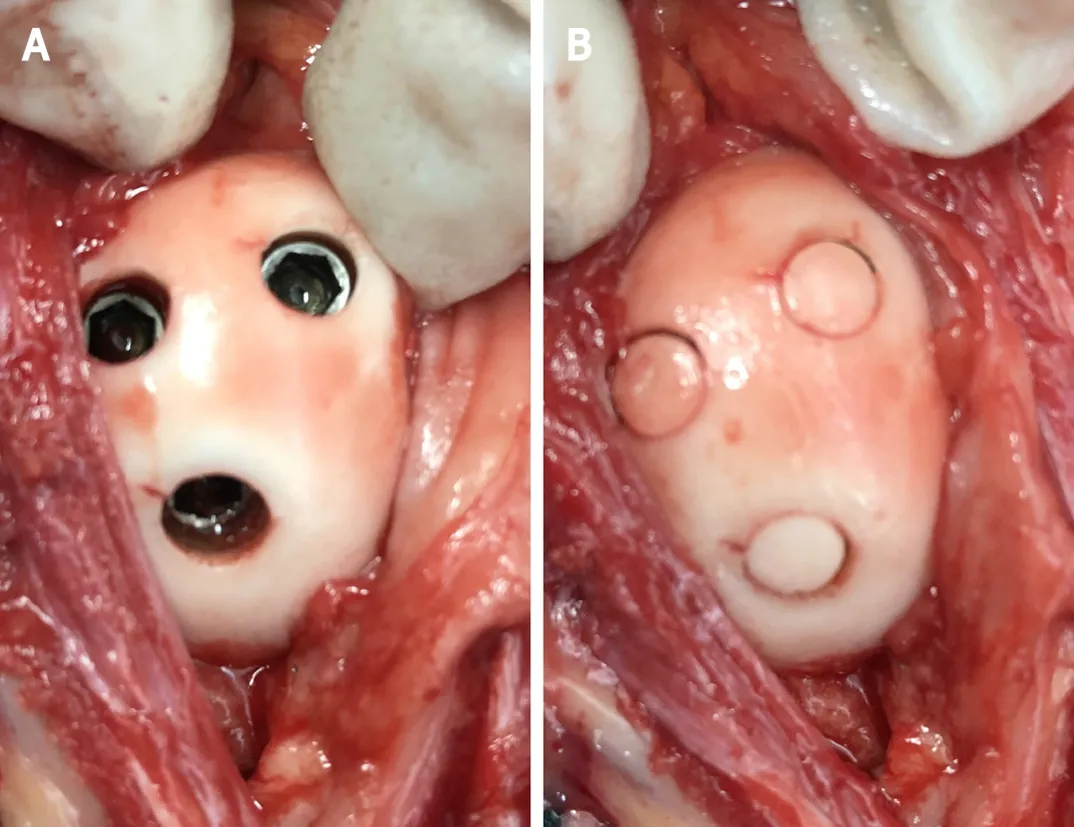
Following examination and under anesthesia,the patient was placed in the prone position,with the knee stabilized and locked in a flexed 30° position.The fracture was accessed through a posteromedial incision to the knee.Under X-ray guidance,the medial femoral condyle fragment was reduced and temporarily fixed with Kirschner wires.A 5.0 mm annular drill (Wellbone,Suzhou,China) was used to remove the 5.0 mm × 5.0 mm cylindrical articular cartilage and subchondral bone.After fixing the fragment with three 3.5 mm partially threaded cancellous screws (inserted in a posterior-to-anterior direction),the articular cartilage and subchondral bone were reimplantedand the screw heads were covered (Figure 2) to ensure stability and ease upon pressure.Postoperatively,the limb was maintained on a long-leg back slab with the knee in a 30° flexion position for approximately 2 wk.Active isometric muscle contractions were permitted during this period.Subsequently,the slab was removed,and passive flexion and extension exercises were initiated.
TREATMENT
Hoffa fracture.
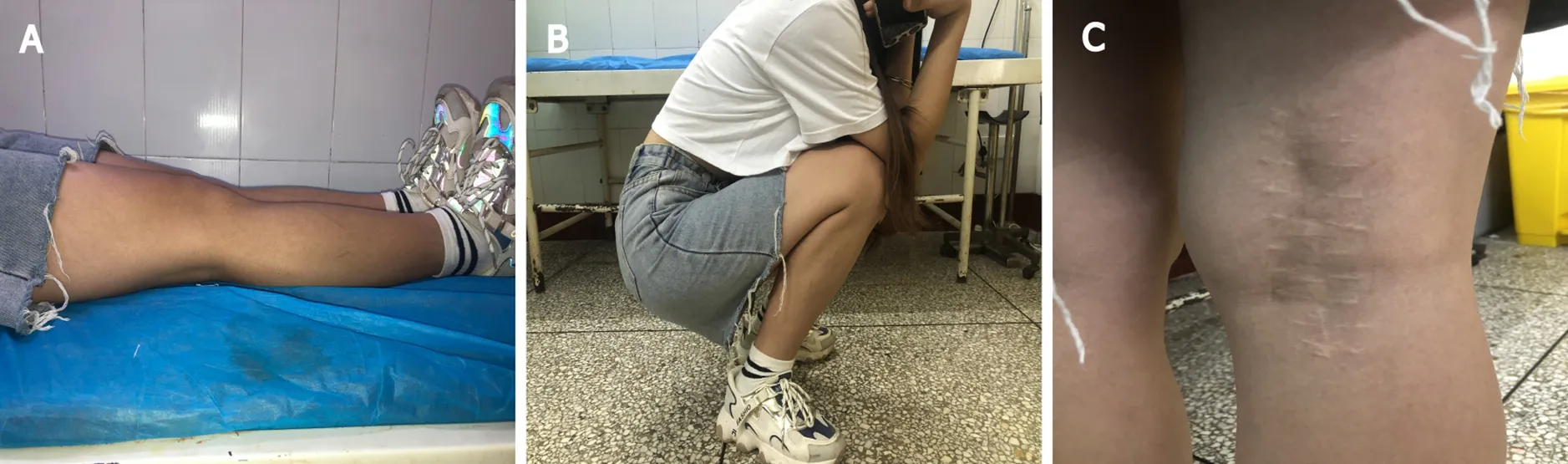
Upon radiographic monitoring,weight-bearing was gradually permitted at 2 mo.At the 6-mo follow-up,the patient presented a knee range of motion of 0°–135° without pain,and was walking without support with a normal gait (Figure 3).The fracture and osteochondral plug had completely healed.There were no signs of avascular necrosis of the femoral condyle or knee osteoarthritis (Figure 4).The patient and her parents provided consent for the publication of the images.
OUTCOME AND FOLLOW-UP
The passengers on the bus watched sympathetically as the young woman with the white cane1 made her way carefully up the steps. She paid the driver and then, using her hands to feel the location of the seats, settled in to one. She placed her briefcase2 on her lap and rested her cane against her leg.
“Which brings up the vegetables, sir. Would you like steamed broccoli8, creamed corn, sauteed zucchini, diced9 carrots--”That did it. I threw my napkin to the floor, stood up, put my face right in his arrogant10 kisser and said, “How’d you like to settle this outside?”
When I have a fine courtyard of my own at the King s palace, I shall perhaps ask some of you to come and pay me a short visit, and scarcely waiting to say good-bye to his family, away he stumped12 down the high road that led to Madrid

DISCUSSION
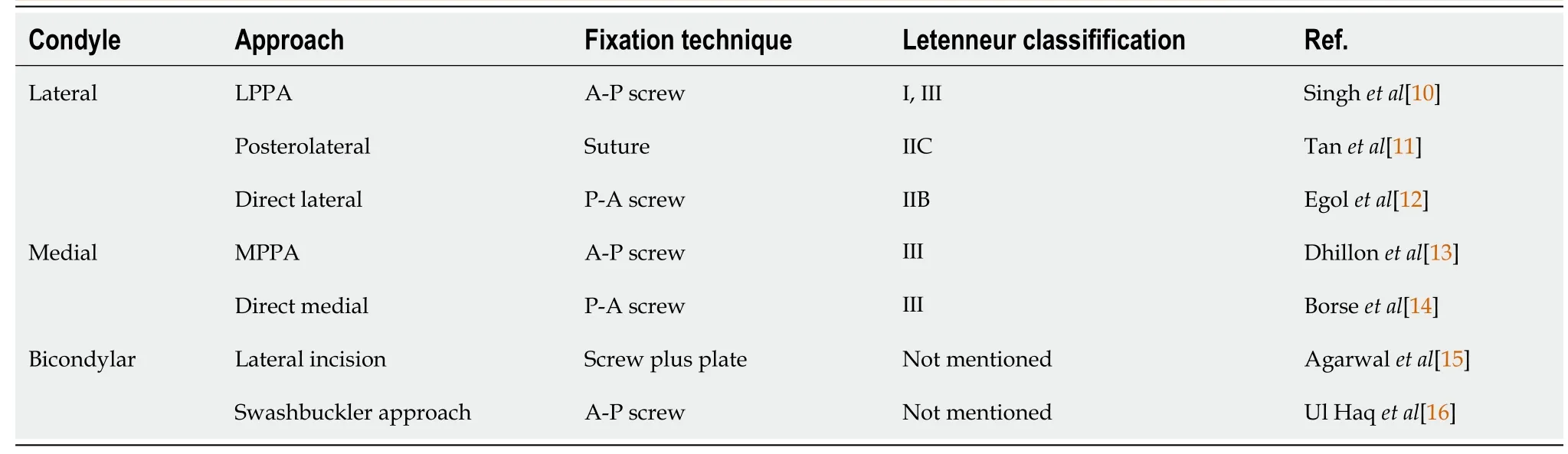
A coronal fracture of the distal femur is termed as Hoffa fracture;Letenneur et al[2] divided it into three types according to the relationship between the fracture line and the posterior cortex of the femoral shaft in 1978[2].Type I is a fracture in the posterior cortical extension of the distal femur.Type II fracture is similar to type I fracture,but the fracture line is closer to the posterior condyle,and is further divided into A,B,and C subtypes based on the distance.Type III is a fracture oblique to the femur condyle,and can be divided into the medial,lateral,or conjoint bicondylar fracture according to the fracture site[1,8,9].A summary of the main surgical approaches and fixation methods for different Hoffa fracture types is provided in Table 1[10-16].There is no optimal surgical approach and fixation method for Hoffa fractures as described in Table 1.Direct lateral/medial and posterolateral approaches can expose small Hoffa fragments and employ the more biologically advantageous posterior-anterior direction screws,as well as a plate if necessary,but with a risk of neurovascular injury;lateral/medial parapatellar approaches are suitable for large Hoffa fragments and can expose both the femoral condyles,but small Hoffa fragments are difficult to expose and reduce,and posterior-anterior direction screws are not feasible[17].Other studies[18-21] reported the treatment of the nonunion of Hoffa fracture,suggesting bone grafting following debridement and fixation with screws and bone plates,and finally achieved satisfactory results.Currently,there is no optimal surgical approach and fixation method[3];hence,the treatment of the different types of Hoffa fractures are mainly determined by the experience and skill of the surgeon.Studies have demonstrated that the biomechanics of the screws in the posterior-anterior direction are superior to the screws in the anterior-posterior direction[22,23].Furthermore,if the fracture is small,such as a type II fracture,posterior-anterior direction screws are strongly recommended except for the type II C fracture[11].Therefore,the posterior-anterior direction screws should be preferred for Hoffa fractures.However,this will inevitably damage the articular cartilage when holes are punched in the articular surface.Even though Borse[14] attempted to avoid damage to the articular cartilage by using headless screws,the cartilage was still damaged to a certain extent.However,the method we provide solves this problem well.Our paper reports a rare case;although open isolated Hoffa fractures of the medial femoral condyle have been reported in children[24],no study has reported a similar case treated by open reduction and internal fixation with osteochondral plug re-implantation.
This type of fracture has a high rate of complications,such as avascular necrosis and osteoarthritis,owing to the subsequent reduction of blood supply to the area and the absence of soft tissue attachment.Surgical stabilization is the preferred treatment for Hoffa’s fractures to achieve satisfactory long-term functional results[25].In our case,we chose the posteromedial approach to access the knee and used the screws to fix the fragment.The articular cartilage and subchondral bone at the location of the screw were removed in advance,and the head of the screw lowered following its fixation;the articular cartilage and subchondral bone were re-implanted and used to cover the screw heads.Similar to osteochondral autograft implantation,osteochondral plug reimplantationcan reduce the extent of cartilage damage.Osteochondral autograft implantation is commonly used in articular cartilage defects,and excellent results have been achieved[26].This report offers similar methods.The osteochondral plug healed successfully,because fragmentation of healthy cartilage is meant to activate the mitogenic activity of chondrocytes,which proliferate and secrete extracellular matrix to repair damaged cartilage tissue[27].We obtained sufficient stability between the fragments,and minimized the damage to the articular cartilage attributed to the surgical procedure.The fracture and osteochondral plug healed,and joint function improved 6 mo postoperatively.
The potential risks,the non-healing and failure of the osteochondral plugs,and minor difficulties in removing the internal fixation when necessary are the potential problems that need to be resolved.
CONCLUSION
To date,a similar surgical treatment has not been reported in the literature.We believe that this innovative surgical procedure could provide a new possibility for the treatment of Hoffa fracture,and further improve the treatment system in patients with similar conditions;however,more cases are warranted to confirm our claims.
We would like to thank the nursing team of the Department of Orthopedics,No.2 People’s Hospital of Yibin City,for the support,and our patient for participating in this study.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report