
Successful management of delirium with dexmedetomidine in a patient with haloperidol-induced neuroleptic malignant syndrome:A case report
2022-02-13 06:03:35ChiJuYangChingTangChiuYuChangYehAnneChao
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Delirium,a transient,reversible organic mental syndrome characterized by disorganized thinking and altered consciousness,commonly occurs in acutely hospitalized elderly patients[1].Hospital-acquired delirium can be triggered by certain drugs administered upon admission or during the patient’s stay,including benzodiazepines[2].While haloperidol is a commonly accepted first-line treatment against agitated delirium[3],the risk of serious adverse events is not negligible.Among them,neuroleptic malignant syndrome (NMS),a life-threatening condition characterized by hyperthermia,severe muscle rigidity,altered mental status,and autonomic dysfunction,can occur in 0.02%-3% of all patients who receive haloperidol[4].The clinical management of NMS poses major challenges,but intensive care unit (ICU)medications are emerging as part of the therapeutic armamentarium[5].
Herein,we report a case of lorazepam-induced agitated delirium treated with haloperidol,which in turn triggered the onset of NMS.The latter condition,a medical emergency,was effectively managed with medical treatment and dexmedetomidine,a versatile and highly selective short-acting alpha-2 adrenergic agonist with sedativehypnotic and anxiolytic effects[6].Because extreme sympathetic nervous system activation is involved in the pathophysiology of NMS[7],we hypothesized that dexmedetomidine may be clinically beneficial for managing this medical emergency because of its sympatholytic activity[8].
CASE PRESENTATION
Chief complaints
A 65-year-old man presented to the emergency department with severe abdominal discomfort after binge eating.
The King mourned, but he did not think that the Queen had done the wicked deed, and as he was afraid the maiden would also be taken from him, he wanted to take her with him
History of present illness
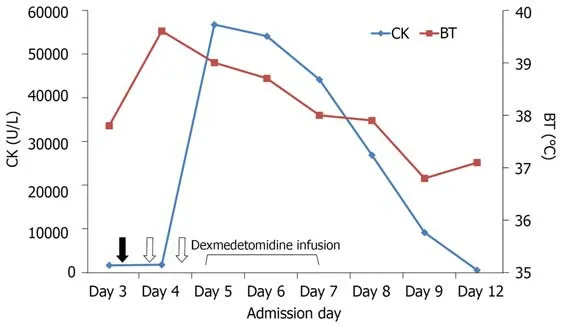
Because of food impaction,oral intake and medications were discontinued.However,lorazepam was administered intravenously to treat insomnia.The next day,the patient became delirious and was thus treated with seven doses (5 mg each) of haloperidol over a 48 h period.Unfortunately,he developed hyperthermia (body temperature:40.6°C) accompanied by tachypnea (respiratory rate:40 breaths per min),tachycardia(heart rate:128 beats per min),impaired consciousness,muscle rigidity,and dark urine.The serum creatine kinase (CK) levels were markedly increased (1910 U/L)(Figure 1),indicating rhabdomyolysis.NMS was diagnosed,and haloperidol was immediately stopped.Adequate hydration and body cooling were implemented;additionally,bromocriptine (2.5 mg/3 times daily) and transdermal patches containing rotigotine (2 mg/24 h) were applied to overcome the hypodopaminergic state.The patient was subsequently transferred to the ICU for intensive monitoring and treatment of NMS.
History of past illness
On ICU admission,the patient was confused and disoriented to time,space,situation,and persons.His Glasgow coma score (GCS) was 13 (Eye 4,Motor 5,and Verbal 4) and papillary light reflexes were bilaterally positive.Severe rigidity and myoclonus(especially in the upper extremities) were evident.Additionally,the patient was severely agitated (Richmond Agitation-Sedation Scale (RASS)[9] score=3),and made attempts at removing his intravenous catheter and nasogastric tube.In addition to continuation of medical management,dexmedetomidine infusion was started (initial rate:0.2 μg/kg/h) with the goal of achieving a RASS score of-1 or 0.Owing to persistent agitation (accompanied by shouting and attempts to remove restraints),dexmedetomidine dosing was further increased to 0.5 μg/kg/h.Gradual resolution of muscle rigidity,myoclonus,and agitation was observed over the next day (GCS score:14).Thus,the dosage of dexmedetomidine was lowered to 0.3 μg/kg/h.The family’s presence at the patient’s bed side was encouraged.Containment measures were removed and the dexmedetomidine dosing was further reduced.Full cooperation was achieved 72 h after the initial infusion of dexmedetomidine,which was thus discontinued.After full regression of rhabdomyolysis and rigidity,the patient was transferred to the general ward for further care.Figure 3 depicts the timeline of the main clinical events.
“Yes, you are dear to me,” said the prince; “for you have the best heart, and you are the most devoted99 to me; you are like a young maiden whom I once saw, but whom I shall never meet again
Personal and family history
Lorazepam-induced delirium treated with haloperidol,which in turn triggered NMS.
Physical examination
Upon initial evaluation,the patient’s temperature was 36 °C,the heart rate 102 beats per min,and the respiratory rate 20 breaths per min.A physical examination revealed abdominal tension.
The world is filled with smart, talented, educated and gifted people. We meet them every day. A few days ago, my car was not running well. I pulled it into a garage, and the young mechanic had it fixed1 in just a few minutes. He knew what was wrong by simply listening to the engine. I was amazed. The sad truth is, great talent is not enough.
Laboratory examinations
The patient did not present additional episodes of delirium and was successfully discharged 18 d after admission.He is currently undergoing regular follow-up at our psychiatric clinic.
Computed tomography revealed food impaction accompanied by bowel distension from the esophagus to the small intestine (Figure 2).
Imaging examinations
The Prince, without the smallest hesitation47, snatched up a great stone, and hammered vigorously upon the bell, which gave forth48 a deep and terrible sound, the gate flew open, and closed again with a thundering clang the moment the Prince had passed through it, while from every tower and battlement rose a wheeling, screaming crowd of bats which darkened the whole sky with their multitudes
FINAL DIAGNOSIS
Bipolar disorder.
TREATMENT
The patient’s medical history was notable for bipolar disorder,and his medications included trihexyphenidyl,quetiapine,flupentixol,and flunitrazepam.


OUTCOME AND FOLLOW-UP
The laboratory findings upon ICU admission were as follows:CK,21000 U/L;blood urea nitrogen,29 mg/dL;creatinine,1.4 mg/dL;potassium,4.5 mEq/L;blood pH,7.4;PCO,31 mmHg;PO,70 mmHg;HCO,23 mEq/L;and base excess,-1.5 mmol/L.
Her delight was complete when her brother (who had killed the Magician under the form of a bull) was seen coming from the forest in his proper shape, and that very day, according to her promise, she gave her hand in marriage to the happy young tailor
DISCUSSION
We describe a complex case of lorazepam-induced delirium occurring in an elderly hospitalized patient who was admitted for food impaction.Treatment of delirium with haloperidol precipitated the onset of NMS,an uncommon,yet life-threatening,complication of antipsychotics.Early diagnosis and removal of precipitating agents are very important in the management of NMS.NMS was managed with dexmedetomidine,an ICU drug,which successfully corrected autonomic instability.Clinical improvement was observed within a few days and the patient was successfully discharged 18 d after admission.Our case provides an illustrative example of how polypharmacotherapy in acutely hospitalized elderly patients can give rise to medical emergencies requiring ICU care.
Benzodiazepines are a common cause of drug-induced delirium.In the elderly,because of the decreased renal clearance and other age-related pharmacodynamic and pharmacokinetic changes,these drugs can accumulate and cause toxicity and delirium[10].Our patient became delirious after in-hospital administration of lorazepam for insomnia.Although the mechanisms of benzodiazepine-induced delirium are not well defined,neurotransmitter imbalances with excess brain dopaminergic activity are common in delirious patients[10,11].Importantly,while medications can induce delirium,they may also be used to manage its symptoms[10].Owing to their antidopaminergic effects,typical antipsychotics like haloperidol are commonly used in managing delirium[3].As in our patient,haloperidol can be given at multiple doses(2-5 mg every 15-30 min) until clinical improvement is achieved[12].However,the use of haloperidol for managing delirium in our case precipitated the onset of NMS,possibly as a result of excess dopamine Dreceptor blockade in the hypothalamic,nigrostriatal,mesolimbic,and mesocortical pathways[13].
Once NMS is diagnosed,ICU drugs like dexmedetomidine or propofol are potentially effective management options[14,15].Because extreme sympathetic nervous system activation is involved in the pathophysiology of NMS[7],we reasoned that dexmedetomidine may be helpful in the management of this medical emergency because of its sympatholytic activity[8].In the presence of rapid shallow breathing as in our case,dexmedetomidine may also provide better patient comfort with less respiratory depression than does propofol[16].Importantly,dexmedetomidine also suppresses the spontaneous firing rate of locus coeruleus neurons and decreases heat generation by alpha-2 adrenergic receptor blockade in the hypothalamus[17].Hence,it can successfully correct the profound thermogenesis and hypermetabolism typical of NMS as it did in our patient.While recommendations for specific treatments in NMS continue to be based on small-sized studies and clinical experience,this case serves as a useful reminder to clinicians to consider dexmedetomidine as part of the current therapeutic armamentarium.
CONCLUSION
Dexmedetomidine may be clinically beneficial for managing NMS because of its sympatholytic activity and its capacity to reduce heat generation.In the presence of rapid shallow breathing,dexmedetomidine may also provide better patient comfort with less respiratory depression than does propofol.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- Using a fretsaw in treating chronic penial incarceration:A case report
- Occupational fibrotic hypersensitivity pneumonia in a halogen dishes manufacturer:A case report
- Accelerated Infliximab Induction for Severe Lower Gastrointestinal Bleeding in a Young Patient with Crohn’s Disease:A Case Report
- Tension pneumocephalus following endoscopic resection of a mediastinal thoracic spinal tumor:A case report
- Primary adrenal diffuse large B-cell lymphoma with normal adrenal cortex function:A case report
- Varicella-zoster virus-associated meningitis,encephalitis,and myelitis with sporadic skin blisters:A case report