
Effects of acupuncture plus spinal manipulations on physical functioning and biochemical indicators in patients with ankylosing spondylitis
2021-06-22 06:37:06DengGuiyi鄧貴毅HuangJianhui黃健輝ZhongXingmu鐘興木HanJiawei韓嘉瑋WeiZengsheng韋增勝QiuYuehui邱月輝
Deng Gui-yi (鄧貴毅), Huang Jian-hui (黃健輝), Zhong Xing-mu (鐘興木), Han Jia-wei (韓嘉瑋), Wei Zeng-sheng (韋增勝),Qiu Yue-hui (邱月輝)
Qinzhou Hospital of Traditional Chinese Medicine, Guangxi Zhuang Autonomous Region, Qinzhou 535099, China
Abstract Objective: To observe the effects of acupuncture plus spinal manipulations on the physical functioning and levels of alkaline phosphatase (ALP), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and osteoprotegerin (OPG) in patients with ankylosing spondylitis (AS).
Keywords: Acupuncture Therapy; Chiropractic; Visual Analog Scale; Pain Measurement; Blood Sedimentation; Spondylitis,Ankylosing
Ankylosing spondylitis (AS) is an autoimmune disease of unknown etiology characterized by chronic inflammation that primarily affects the axial skeleton,sacroiliac joints and spine. Patients often present with bony ankylosis, intervertebral disc fibrosis and calcification of connective tissue. The early stage AS may cause pain and stiffness in the lower back. Over time, it may cause a high rate of disability and multiple complications, thus severely affecting the patients’quality of life[1].
Currently, AS is often treated with slow-acting antirheumatic drugs (SAARDs) and non-steroidal antiinflammatory drugs (NSAIDs). However, these drugs may cause adverse reactions such as gastrointestinal discomfort, bone marrow suppression or liver damage[2].It is therefore important to seek a safe and effective therapy for AS.
Some studies have reported that biological agents may be beneficial[3]. However, they are too expensive for most patients. Some researchers[4]have reported that needling Jiaji (EX-B 2) points can improve clinical symptoms in AS patients and help with functional recovery of the spine. Other researchers[5]have reported that spinal manipulations can relax the ligament and improve the spinal mobility in AS patients. In this study,we treated two groups of AS patients diagnosed between October 2017 and May 2019 with acupuncture plus spinal manipulations, and observed the efficacy and compared the physical functioning as well as the levels of alkaline phosphatase (ALP), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and osteoprotegerin (OPG). The results are now summarized as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnosis in Western medicine[6]
The lower back pain persisted >3 months and the pain improves with activity but not with rest; poor spinal range of motion; a lower chest expansion range; and sacroiliitis grade Ⅲ-Ⅳ on one side or sacroiliitis gradeⅡ-Ⅲ on both sides.
1.1.2 Diagnosis in traditional Chinese medicine (TCM)[7]
Major symptoms: Stiffness and pain in the low back,difficulty bending the low back, and pain or weakness in the leg that improves with warm and worsens with cold.
Minor symptoms: Leucorrhea in women, or a cold sensation in the scrotum in men, a white thick or thin white tongue coating, and a deep, wiry, and thready or weak pulse.
1.2 Inclusion criteria
Those who met the above criteria in both Chinese and Western medicine; aged between 18 and 60 years; no history of mental illness; no history of drug allergy; and willing to sign the informed consent.
1.3 Exclusion criteria
Those having severe cerebro-cardiovascular diseases;women during pregnancy or lactation; having other rheumatic diseases; having severe spine or joint deformity; and those who are not suitable for acupuncture or spinal manipulations.
1.4 Statistical methods
The data were analyzed using the SPSS version 21.0 statistical software. The measurement data in normal distribution and equal variance were expressed as mean± standard deviation (±s). The pairedt-test was used for within-group comparisons, while independent samplest-test was used for between-group comparisons.The measurement data in abnormal distribution and unequal variance were expressed as median(interquartile range). The Wilcoxon rank sum test was used for intra-group comparison. The enumeration data were expressed as percentage, analyzed by Chi-square test. The Wilcoxon rank sum test was used for ranked data. A two-tailedP-value of less than 0.05 indicated statistical significance.
1.5 General materials
All the 128 cases included in this study were treated in our hospital between October 2017 and May 2019. They were allocated into a control group and an observation group by using random number table method, with 64 cases in each group. There were no dropouts during the treatment. There were no between-group significant differences in gender, age and disease duration (allP>0.05), indicating that the two groups were comparable(Table 1).
2 Treatment Methods
2.1 Control group
Patients in the control group took sulfasalazine enteric-coated tablets [State Food and Drug Administration (SFDA) Approval No. H31020840,0.25 g/tablet, Shanghai Fuda Pharmaceutical Co., Ltd.,China], 1.0 g per dose and three doses a day, along with meloxicam tablets (SFDA Approval No. H20030486,7.5 mg/tablet, Hainan Xiansheng Pharmaceutical Co.,Ltd., China), 7.5 mg per dose and one dose a day. The dosage can be adjusted to patients’ actual conditions.
2.2 Observation group
Besides the same medications as in the control group,patients in the observation group received additional acupuncture and spinal manipulations.
Points: Thirty-four Jiaji (EX-B 2) points (17 points on each side) from T1to L5(0.5 cun lateral to the spinous processes of the thoracic and lumbar vertebrae).
Method: Punctured till 0.3-0.5 cun perpendicularly using disposable stainless filiform needles (0.25 mm in diameter and 40 mm in length) and retained the needles for 30 min after arrival of qi. The treatment was done once a day, 5 d a week. There was a 2-day interval between two sessions.
Spinal manipulations: With a prone position of the patient, the practitioner first An-pressed and Roukneaded both sides of the erector spinae 2-3 min to relax muscles, Tanbo-plucked tight rope-like nodules 2-3 min to relax these firm nodules and the surrounding muscles,applied approximately 5-minute Dian-digital pressing(Figure 1) to the points along the Governor Vessel, Jiaji(EX-B 2) points and Houxi (SI 3), including 30 s each for Dazhui (GV 14), Zhiyang (GV 9), Jizhong (GV 6), Jinsuo(GV 8), Yaoyangguan (GV 3), Mingmen (GV 4) and Houxi(SI 3), then applied oblique Ban-pulling to the cervical and lumbar vertebrae and pressed down along the thoracic vertebrae using crossed hands to increase the joint space (Figure 2 and Figure 3), and finally applied Mo-circular rubbing and Ca-scrubbing to both sides of the spine until a warm sensation occurred. The treatment was done once a week.
The therapeutic efficacy was observed after 8 weeks of treatment.
3 Observation of Results
3.1 Observation items
3.1.1 TCM symptoms
The TCM symptom scoring system was used to evaluate lumbosacral pain, low back/leg weakness and soreness, limited lumbar motion, morning stiffness, cold feeling in the joints, limb heaviness, cold intolerance, and fatigue. Each item was graded 2 (mild), 4 (moderate) or 6 points (severe), and a higher score indicated a more severe symptom.
3.1.2 The visual analog scale (VAS) scoring
The VAS (0-10) was used to assess the pain severity. A higher score indicated a more severe pain.
3.1.3 Physical functioning
The Bath AS functional index (BASFI) and Bath AS disease activity index (BASDAI) were used to assess the physical functioning. A higher score (0-10) indicated a poorer physical functioning.

Figure 1. Dian-digital pressing the lumbar Jiaji (EX-B 2) points

Figure 2. Obliquely Ban-pulling the cervical vertebrae

Figure 3. Obliquely Ban-pulling the lumbar vertebrae
3.1.4 Lab test items
Before and after treatment, 5 mL venous blood was drawn from patients with an empty stomach to measure the ALP, CRP and OPG levels using enzyme-linked immunosorbent assay (ELISA). The ESR was measured using Westergren method.
3.1.5 Adverse reactions
Adverse reactions were observed and recorded in both groups.
3.2 Efficacy criteria[8]
Clinical recovered: Morning stiffness and joint pain were almost absent, along with a normal spinal motion and ESR level.
Markedly effective: Morning stiffness and joint pain were remarkably alleviated, along with a notable increase in spinal motion and decrease in ESR.
Effective: Morning stiffness and joint pain were alleviated, along with an increase in spinal motion and decrease in ESR.
Failure: Morning stiffness and joint pain worsened,and there was no improvement in spinal motion or decrease in ESR.
3.3 Results
3.3.1 Comparison of TCM symptoms
Before treatment, there were no significant betweengroup significant differences in clinical symptoms(lumbosacral pain, low back/leg weakness and soreness,limited lumbar motion, morning stiffness, cold feeling in the joints, limb heaviness, cold intolerance and fatigue),(allP>0.05). After treatment, the TCM symptom scores in both groups were decreased and these scores in the observation group were significantly lower than in the control group (allP<0.05), (Table 2).
Table 2. Comparison of TCM symptoms (±s, point)
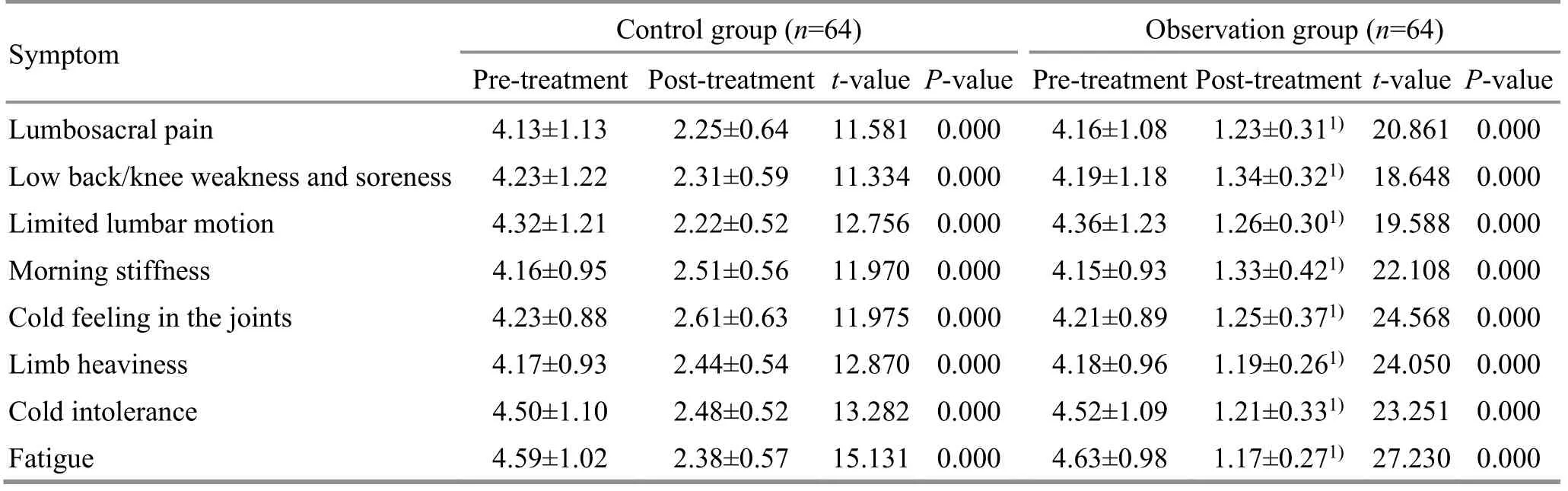
Table 2. Comparison of TCM symptoms (±s, point)
Note: Compared with the control group at the same time point, 1) P<0.05
Symptom Control group (n=64) Observation group (n=64)Pre-treatment Post-treatment t-value P-valuePre-treatment Post-treatment t-value P-value Lumbosacral pain 4.13±1.13 2.25±0.64 11.581 0.000 4.16±1.08 1.23±0.311) 20.861 0.000 Low back/knee weakness and soreness 4.23±1.22 2.31±0.59 11.334 0.000 4.19±1.18 1.34±0.321) 18.648 0.000 Limited lumbar motion 4.32±1.21 2.22±0.52 12.756 0.000 4.36±1.23 1.26±0.301) 19.588 0.000 Morning stiffness 4.16±0.95 2.51±0.56 11.970 0.000 4.15±0.93 1.33±0.421) 22.108 0.000 Cold feeling in the joints 4.23±0.88 2.61±0.63 11.975 0.000 4.21±0.89 1.25±0.371) 24.568 0.000 Limb heaviness 4.17±0.93 2.44±0.54 12.870 0.000 4.18±0.96 1.19±0.261) 24.050 0.000 Cold intolerance 4.50±1.10 2.48±0.52 13.282 0.000 4.52±1.09 1.21±0.331) 23.251 0.000 Fatigue 4.59±1.02 2.38±0.57 15.131 0.000 4.63±0.98 1.17±0.271) 27.230 0.000
3.3.2 Comparison of the VAS, BASFI and BASDAI scores
Before treatment, there were no significant betweengroup differences in the VAS, BASFI and ASDAI scores before treatment (allP>0.05). After treatment, the VAS,BASFI and BASDAI scores in both groups were decreased(allP<0.05), and these scores in the observation group were significantly lower than in the control group (allP<0.05), (Table 3, Table 4 and Table 5).
3.3.3 Comparison of the ALP, ESR, CRP and OPG levels
Before treatment, there were no significant betweengroup differences in the ALP, ESR, CRP and OPG levels (allP>0.05). After treatment, the ALP, ESR, CRP and OPG levels in both groups were decreased (allP<0.05), and these levels in the observation group were significantly lower than in the control group (allP<0.05), (Table 6-Table 9).
Table 3. Comparison of VAS score (±s, point)
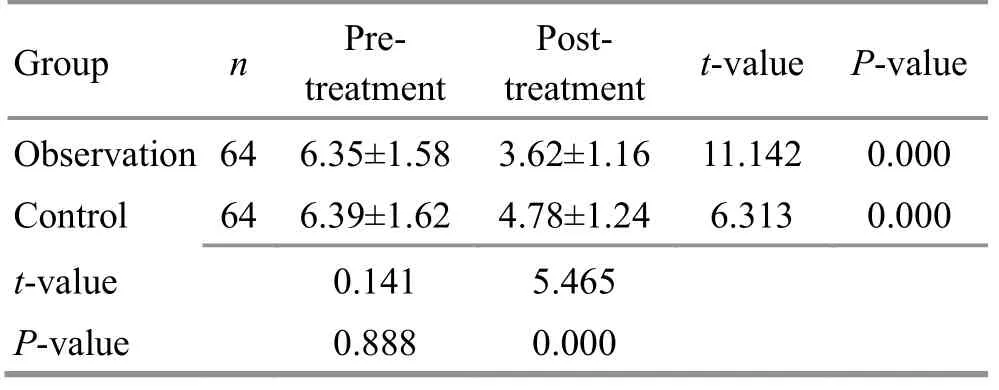
Table 3. Comparison of VAS score (±s, point)
Group n Pretreatment Posttreatment t-value P-value Observation 64 6.35±1.58 3.62±1.16 11.142 0.000 Control 64 6.39±1.62 4.78±1.24 6.313 0.000 t-value 0.141 5.465 P-value 0.888 0.000
Table 4. Comparison of BASFI score (±s, point)

Table 4. Comparison of BASFI score (±s, point)
Group n Pretreatment Posttreatment t-value P-value Observation 64 4.93±1.12 3.26±1.02 8.819 0.000 Control 64 4.89±1.11 4.13±1.06 3.961 0.001 t-value 0.203 4.731 P-value 0.888 0.000
Table 5. Comparison of BASDAI score (±s,point)
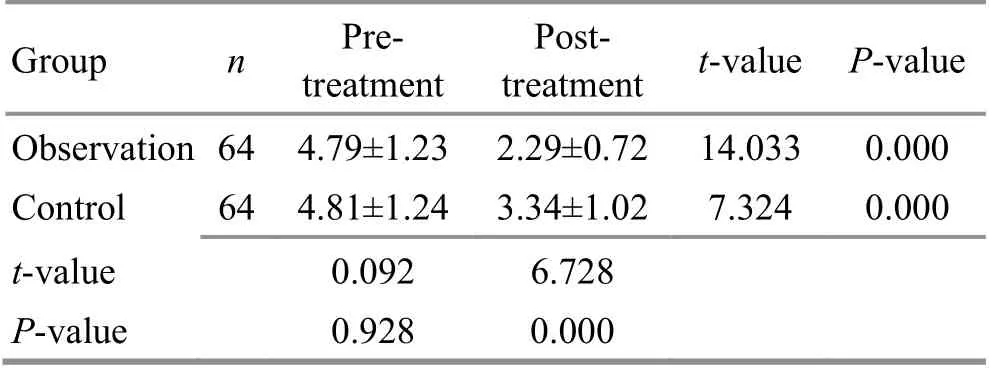
Table 5. Comparison of BASDAI score (±s,point)
Group n Pretreatment Posttreatment t-value P-value Observation 64 4.79±1.23 2.29±0.72 14.033 0.000 Control 64 4.81±1.24 3.34±1.02 7.324 0.000 t-value 0.092 6.728 P-value 0.928 0.000
Table 6. Comparison of ALP level (±s, U/L)

Table 6. Comparison of ALP level (±s, U/L)
Group n Pretreatment Posttreatment t-value P-value Observation 64 139.92±42.16 82.79±25.37 9.289 0.000 Control 64 143.28±43.58 95.46±26.49 7.501 0.000 t-value 0.443 2.763 P-value 0.658 0.006
Table 7. Comparison of ESR level (±s, mm/h)
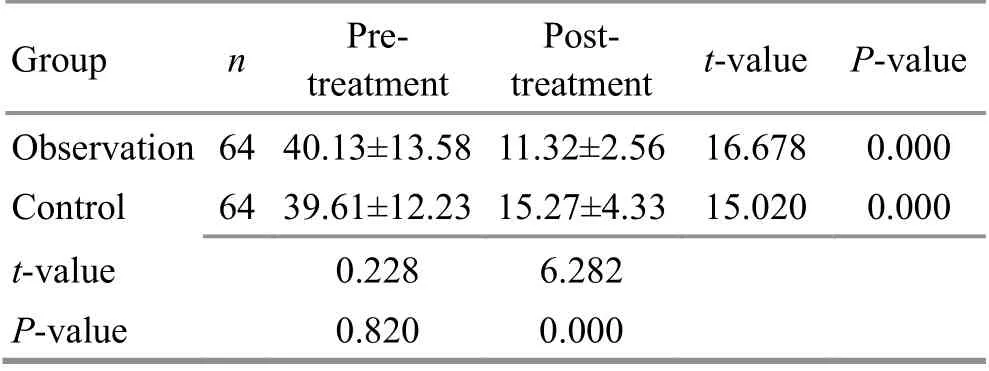
Table 7. Comparison of ESR level (±s, mm/h)
Group n Pretreatment Posttreatment t-value P-value Observation 64 40.13±13.58 11.32±2.56 16.678 0.000 Control 64 39.61±12.23 15.27±4.33 15.020 0.000 t-value 0.228 6.282 P-value 0.820 0.000
Table 8. Comparison of CRP level (±s, mg/L)
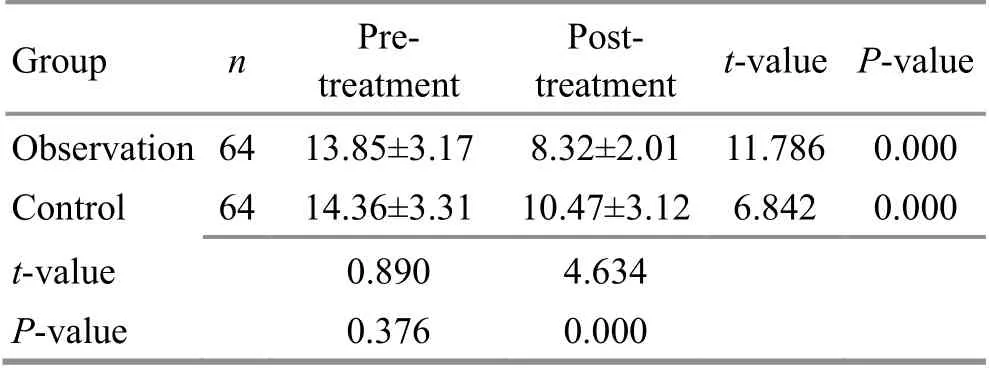
Table 8. Comparison of CRP level (±s, mg/L)
Group n Pretreatment Posttreatment t-value P-value Observation 64 13.85±3.17 8.32±2.01 11.786 0.000 Control 64 14.36±3.31 10.47±3.12 6.842 0.000 t-value 0.890 4.634 P-value 0.376 0.000
Table 9. Comparison of OPG level before and after treatment (±s, pg/mL)

Table 9. Comparison of OPG level before and after treatment (±s, pg/mL)
Group n Pre-treatment Post-treatment t-value P-value Observation 64 1 642.13±513.87 1 230.27±314.52 5.469 0.000 Control 64 1 674.33±521.47 1 473.62±356.45 2.542 0.012 t-value 0.352 4.095 P-value 0.726 0.000
3.3.4 Comparison of clinical efficacy
After treatment, the total efficacy rate was 92.2% in the observation group, versus 78.1% in the control group.There were statistical significances in both efficacy(Z=2.202,P=0.030) and total efficacy rate (P<0.05),(Table 10).
3.3.5 Comparison of adverse reactions
During treatment, 4 cases in the control group had gastrointestinal discomfort, 1 case had skin rash, 1 case had anemia, 2 cases had dizziness and headache, and the overall adverse reaction rate was 12.5%, versus 3 cases in the observation group experiencing gastrointestinal discomfort, 2 cases of skin rash, 1 with anemia, 1 with dizziness and headache and 10.9% of overall adverse reaction rate. There was no significant between-group difference (P>0.05).

Table 10. Between-group comparison of clinical efficacy (case)
4 Discussion
AS is an autoimmune rheumatic disease that primarily affects the axial skeleton and peripheral joints. The basic pathologic process is the tissue degeneration and noninfectious inflammation that targets articular joints,ligaments and tendons[9]. It may cause osteoporosis and a high risk (92.0%) of bone fracture. Some patients may also experience complications involving the heart, eyes,lung and kidney. Due to its high rate of misdiagnosis and disability, this condition may cause loss of joint function and severely affect the patients’ quality of life, if not treated effectively in time[10].
So far, the etiology of AS still remains unknown. Its pathogenesis mainly includes the following aspects[11].The human leukocyte antigen B27 (HLA-B27) gene is important in the pathogenesis of AS. Some studies suggested a strong correlation between AS and HLAB27[12]. This correlation is based on eight hypotheses[13],namely linkage disequilibrium, molecular mimicry, T-cell repertoire, arthritogenic peptide, unfolded protein response, rearrangement of heavy chain structure,heavy chain homodimer and failure of immune tolerance.Currently, AS is often treated with SAARDs and NSAIDs.However, these drugs may cause adverse reactions such as gastrointestinal discomfort or bone marrow suppression. It is therefore important to seek a safe and effective therapy for AS. Some studies have reported that biological agents may be beneficial. However, they are too expensive for most patients[14].
In TCM, AS falls under the category of Bi-impediment syndrome. Contributing factors include malnourishment of bone marrow and Governor Vessel due to kidney yang deficiency, along with stagnation of qi and blood upon exposure to wind, cold or dampness[15].
AS mainly affects the spine (the pathway along the Governor Vessel). This study has found that needling Jiaji(EX-B 2) points on both sides of the spine can increase the circulation of qi and blood, activate yang qi, remove wind cold, eliminate dampness and thus to alleviate pain and unblock meridians. In addition, as the sea of yang meridians, the Governor Vessel governs yang qi of the entire body. As a result, unblocking the Governor Vessel can achieve the goal of unblocking all yang meridians[16].The spinal manipulations in this study focused on Dazhui(GV 14), Zhiyang (GV 9), Jizhong (GV 6), Jinsuo (GV 8),Yaoyangguan (GV 3), Mingmen (GV 4) and Houxi (SI 3) to unblock meridian qi, remove pathogenic factors and reinforce the healthy qi[17].
Modern studies have also found that needling Jiaji(EX-B 2) points can regulate immune functions, inhibit local inflammatory mediators, increase blood flow and thus alleviate pain[18-20]. Spinal manipulations can relieve morning stiffness, increase the spinal range of motion and help to correct spinal deformity[21-23].
Sulfasalazine is an anti-rheumatic drug and can suppress the immune system and reduce inflammation.Meloxicam is a new selective cyclooxygenase-2 (COX-2)inhibitor NSAIDs and can alleviate pain and inflammation.After treatment, the symptom scores were decreased in both groups and the scores in the observation group were lower than in the control group (allP<0.05),suggesting that conventional medications alone or in combination with acupuncture plus spinal manipulation can both alleviate clinical symptoms, but the combination achieved a better efficacy. The VAS, BASFI and BASDAI scores were decreased in both groups and the scores in the observation group were lower than in the control group (allP<0.05), suggesting that conventional medications combined with acupuncture and spinal manipulations can achieve better efficacies than medications alone in alleviating pain and improving the physical functioning.
ALP is produced by osteoblasts and involved in the formation of bone, and its concentration is associated with bone cell activity and bone metabolism. ALP plays a role in bone calcification and increases the enzyme activity[24]. ESR and CRP are biomarkers of inflammatory response and associated with the activity of AS. OPG inhibits the differentiation and maturation of osteoclast precursors as well as the activity of mature osteoclasts[25].After treatment, the ALP, ESR, CRP and OPG levels were decreased in both groups and the levels in the observation group were lower than in the control group(allP<0.05), suggesting that conventional medications alone or in combination with acupuncture and spinal manipulations both can improve the bone cell activity and metabolism, and inhibit bone erosion or destruction,thus alleviating AS severity. A higher overall response rate in the observation group than in the control group indicated a better efficacy by combining medications with acupuncture plus spinal manipulations (P<0.05).Since there was no significant between-group difference in adverse reactions (P>0.05), both methods are safe for AS.
In summary, conventional medications combined with acupuncture and spinal manipulations can alleviate AS symptoms, improve physical functioning and reduce the levels of ALP, ESR, CRP and OPG.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Guangxi Scientific and Technology Key Research and Development Plan (廣西科學(xué)技術(shù)重點(diǎn)研發(fā)計(jì)劃, No. ZXGC201701358).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 30 March 2020/Accepted: 23 July 2020
猜你喜歡
同煤科技(2024年1期)2024-05-12 15:11:52
同煤科技(2023年5期)2023-11-29 05:35:40
中國(guó)空間科學(xué)技術(shù)(2022年2期)2022-04-20 10:46:36
計(jì)算機(jī)技術(shù)與發(fā)展(2021年12期)2022-01-10 07:42:40
中國(guó)體育科技(2019年12期)2019-02-28 12:44:06
歌海(2017年1期)2017-05-30 13:07:40
今日重慶(2017年2期)2017-03-04 01:59:12
歌海(2016年6期)2017-01-10 01:35:52
中國(guó)火炬(2015年2期)2015-07-25 10:45:23
中國(guó)火炬(2015年1期)2015-07-25 10:26:24
 Journal of Acupuncture and Tuina Science2021年3期
Journal of Acupuncture and Tuina Science2021年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Efficacy of acupuncture in treating chronic non-specific low back pain
- Therapeutic efficacy observation of acupuncture plus medicine for laryngopharyngeal reflux due to liver-qi stagnation and spleen deficiency
- Clinical efficacy observation on pediatric massage for chronic cough in children
- Clinical study of warm needling moxibustion plus intra-articular injection of sodium hyaluronate for chondromalacia patellae
- Effect of mild moxibustion on cancer-related fatigue,serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery
- Clinical efficacy observation of acupoint threadembedding in treating obese patients with food addiction