
Abdominal drainage systems in modified piggyback orthotopic liver transplantation
2021-03-05 05:55:24RuiTngLiHnYuJunWeiHnJingYiLinJinJieAnQinLu
Rui Tng , Li-Hn Yu , Jun-Wei Hn , , Jing-Yi Lin , Jin-Jie An , Qin Lu ,
a Hepatopancreatobiliary Center, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Institute for Precision Medicine, Tsinghua University,Beijing 102218, China
b Department of Hepatopancreatobiliary Surgery, Affiliated Hospital of Qinghai University, Xining 810 0 01, China
TotheEditor:
Whether orthotopic liver transplantation requires the placement of an abdominal drainage system is a controversial topic. A number of studies have suggested that prophylactic placement of abdominal drainage systems do not improve the diagnostic rate of complications such as bile leakage and hemorrhage after liver transplantation, even increased the risk of infection [1–3]. However, there is no uniform standard for the selection of drainage tube and how to place the drainage tube in orthotopic liver transplantation. The types and placement modes of the drainage tubes used in each center are different. If adequate drainage is not possible, it may affect the drainage efficiency, which may lead to the misunderstanding that “it is unnecessary to place the drainage tube”. Herein we aimed to explore the most efficient abdominal drainage in modified piggyback orthotopic liver transplantation,based on the types and placement modes of drainage tubes in our clinical practice.
All patients received donation after cardiac death (DCD) or donation after brain death (DBD) liver transplants without marginal donor or partial graft. The donors were under 60 years old, with mild or no fatty liver. In the present study, 5 previous conventional drainages after modified piggyback liver transplantations consisting of subphrenic and epiploic foramen drainages with Tube A(perforated tube) (conventional drainage group) were compared with 40 patients who underwent modified piggyback liver transplantation and were treated with subphrenic drainage and epiploic foramen drainages with Tube B (cruciform drainage tube)and porta hepatis drainage with Tube A (experimental group)( Fig. 1 A). The subphrenic drainage tubes were located between the diaphragm and the right liver, and passed through the hepatorenal recess, the right paracolic sulcus, and were drawn from the right lower abdominal wall. The tip of the drainage tube was near the right-side margin of the suprahepatic vena cava, and the drainage tube was mainly used to drain the effusion from the recessus hepatorenalis and the lowest region of the abdominal cavity ( Fig. 1 B).The epiploic foramen drainage tube was located beside the leftside caudate lobe and the left margin of the inferior vena cava,passed through the backside of the ligamentum hepatoduodenale,the hepato-renal space, and the right-side of paracolic sulci, and finally drawn from the right lower abdominal wall. The tip of the drainage tube was near the left-side margin of the suprahepatic vena cava, and drainage tube was mainly used to drain the effusion from the left-side inferior vena cava, lesser peritoneal sac and backside of the ligamentum hepatoduodenale ( Fig. 1 B). Drainage tubes at the hepatic hilar region were located between the left lateral lobe and the left caudal lobe of the liver, run across the ventral part of the ligamentum hepatoduodenale, the gallbladder bed, and the right-side of paracolic sulci, and finally drawn from the right lower abdominal wall. The drainage tube mainly drained the effusion from the ventral side of the ligamentum hepatoduodenale and the lesser peritoneal sac. The drainage tubes were connected to the airtight drainage bag outside the body. The peritoneal effusion area and positional relationship of the liver, blood vessels, bile duct after transplantation are shown in Fig. 1 C-G. Fig. 1 F and 1 G show patients with hepatic hilar region and epiploic foramen drainage tubes, which were proved to be hemorrhagic ascites cases in the experimental group.
The basic characteristics and drainage information of the experimental and conventional drainage groups are provided in Table 1 .There were no complications resulting from drainage or its extractions.
Tube A was placed in all 5 cases in the conventional drainage group. Complications occurred in 4 patients, including 1 case of hemorrhage combined with abdominal infection and pleural effusion, 1 case of bile leakage combined with abdominal infection, 1 case of abdominal infection combined with renal insufficiency and pleural effusion, and 1 case of poor wound healing ( Table 2 ). Because the subdiaphragm and epiploic foramen drainages were usually located at a lower position, and the surrounding gap was relatively large, we placed a relatively thicker Tube B to improve the drainage efficiency in the experimental group. A thinner drainage Tube A was placed in the hepatic hilar region located on the blood vessel and ventral side of the bile duct. The reason why the thick Tube B was not placed in this hepatic hilar region was that the local space was relatively small, and a thick tube may compress the blood vessels and bile duct. In the conventional drainage group,inadequate drainage may be due to the small diameter of Tube A and in addition there were no hepatic hilar region drainages while effusions tended to accumulate there and around the hepatic duodenal ligament, leading to secondary infections. In the experimental group, there was no case of abdominal infection and therefore,puncture or catheterization due to bile leakage was not necessary,though some patients had positive cultures in samples derived from their drainage, indicating that secondary infections of peritoneal effusion or abscess could be avoided by effective drainages( Table 2 ).
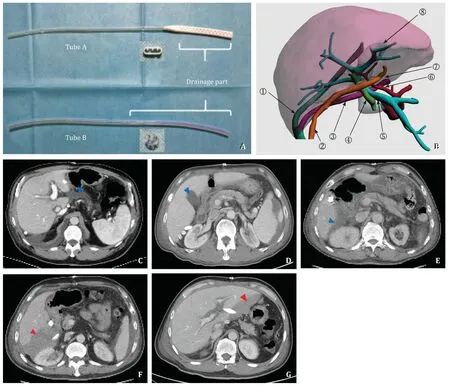
Fig. 1. A : Drainage Tube A (perforated tube) and Tube B (cruciform drainage tube) and their head-end sections. B : Three-dimensional reconstruction image showing the relationship between the drainage tubes and liver structure. Pink: liver; 1 ○subphrenic drainage tube; 2 ○hepatic hilar region drainage tube; 3 ○epiploic foramen drainage tube; 4 ○common bile duct; 5 ○portal vein; 6 ○proper hepatic artery; 7 ○hepatic Spigelian lobe inferior vena cava (retrohepatic); 8 ○inferior vena cava (retrohepatic). C :Lesser peritoneal sac, between the Spigelian lobe and left lateral lobe. D : Gallbladder bed next to hepatic hilar region. E : Between liver and kidney. Blue arrowheads show the peritoneal effusion area after liver transplantation. F : Epiploic foramen drainage tube. G : Hepatic hilar region drainage tube proved to be hemorrhagic ascites. Red arrowheads show abdominal hemorrhage after liver transplantation.
Prophylactic drains are controversial, although deemed necessary, after hepatectomy, gastrointestinal and pancreas surgeries,and liver transplantation [3–6]. Patients after liver transplantation often develop some degree of ascites and are prone to abscess formation once infected. There have been reports of abscess aspiration after transplantation [ 7 , 8 ], or of excessive peritoneal effusion requiring aspiration to relieve the ascites [9]. These findings suggest that drainage should be performed after transplantation and that drainage tubes should be placed in appropriate positions to avoid effusion and secondary infection. The review by Gurusamy et al. pointed out an increased complication rate after stopping the use of drains which may not have been reported by surgeons, because of fear of criticism and punishment for not having offered patients drainages. Thus, these surgeons returned back to the current standard practice of inserting a drain at the end of a liver transplantation. Therefore, there may be bias in the reports of controlled studies with and without drainage tubes and reports of results without drainages might be underrepresented [10].
Our clinical experience suggests that an ultrasound examination should be performed daily within 1 week after surgery, and performed on alternate days 2 weeks after surgery. An abdominal enhanced CT examination should be carried out 5–7 days af-
ter surgery, and a repetitive abdominal CT scan or enhanced CT examination should be performed at 12–14 days after surgery if necessary.
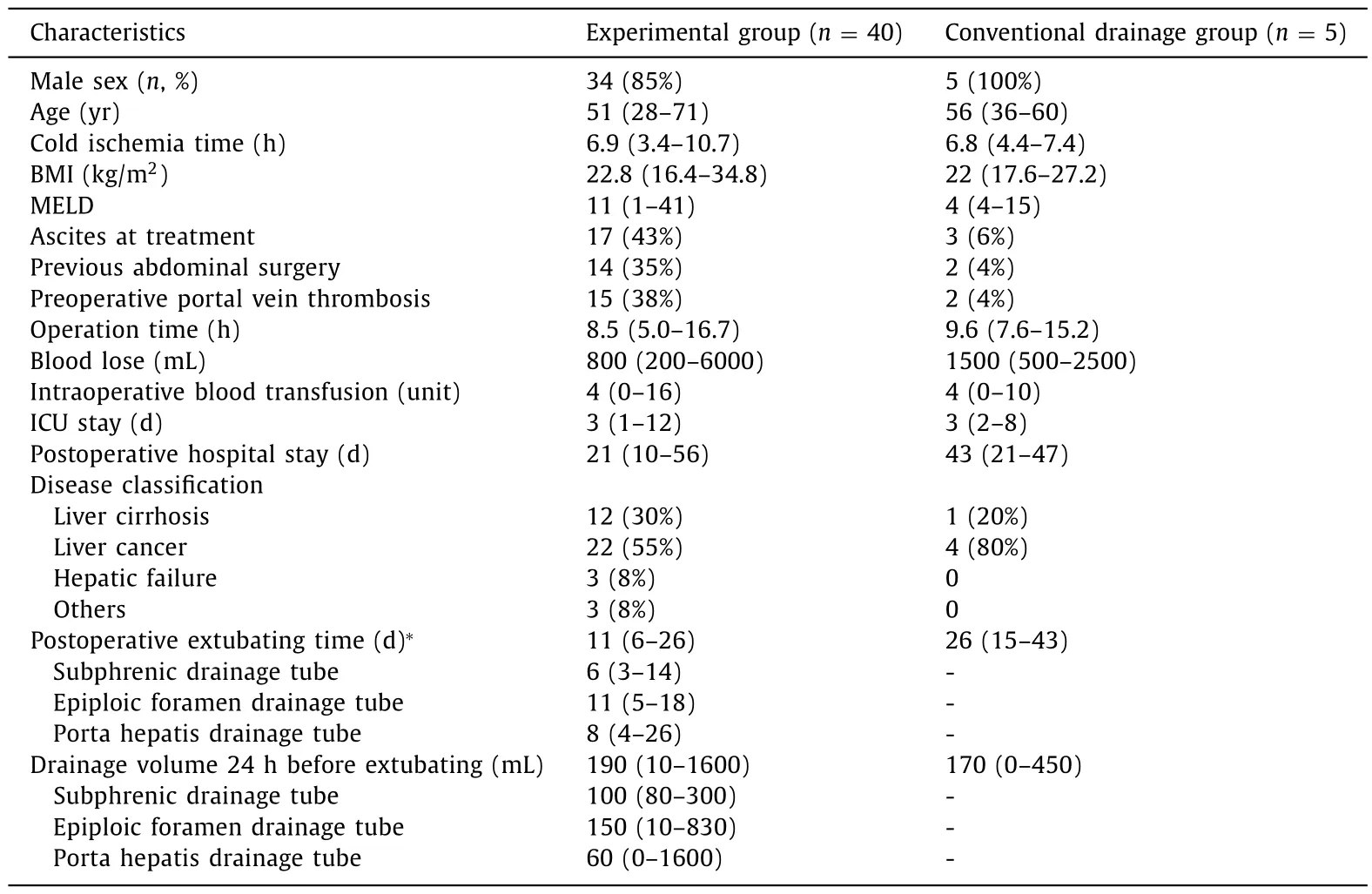
Table 1 Basic and drainage information.
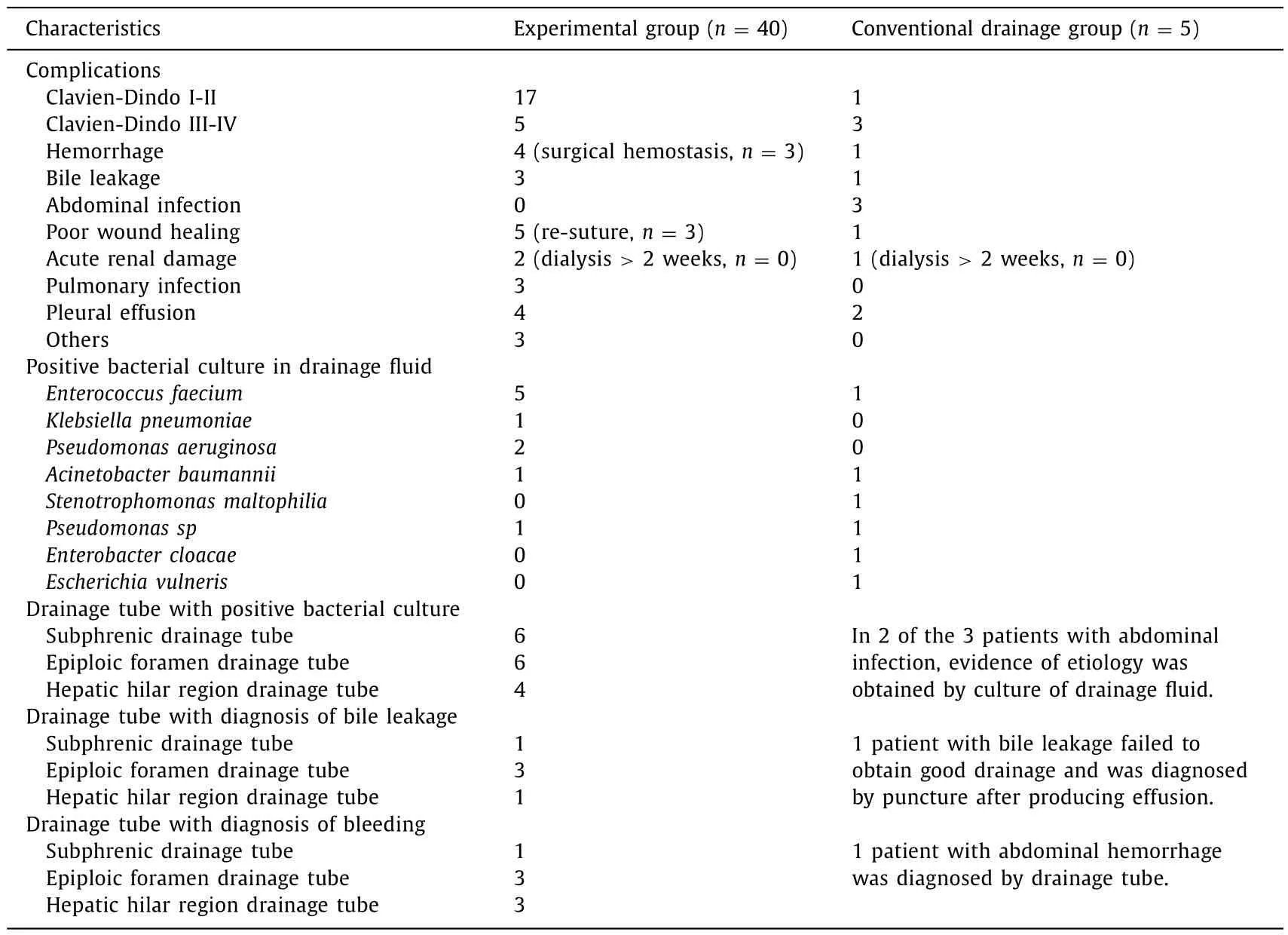
Table 2 Postoperative complications.
In conclusion, appropriate drainage tubes can be placed to detect bile leakage, bleeding and other complications, and can fully drain peritoneal fluid after modified piggyback orthotopic liver transplantation. Closed-circuit drains should be used to avoid infections [11]and the drainage tube should be placed in the best position to facilitate drainage of the surgical site. Due to the anatomical structures, we recommend thicker tubes for subdiaphragm and epiploic foramen drainages and thinner tubes for hepatic hilar region drainages.
Acknowledgments
None.
CRediT authorship contribution statement
Rui Tang:Conceptualization, Data curation, Formal analysis,Investigation, Writing - original draft.Li-Han Yu:Data curation.Jun-Wei Han:Data curation.Jing-Yi Lin:Investigation.Jin-Jie An:Investigation.Qian Lu:Funding acquisition, Supervision, Validation,Writing - review & editing.
Funding
This study was supported by the National Science and Technology Major Project of the Ministry of Science and Technology of China ( 2017ZX100203205 ).
Ethical approval
This study was approved by the Ethics Committee of Beijing Tsinghua Changgung Hospital and written informed consent was obtained from all participating patients.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2021年1期
Hepatobiliary & Pancreatic Diseases International2021年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- BCLC staging system and liver transplantation: From a stage to a therapeutic hierarchy
- Multidisciplinary management of patients with post-inflammatory pancreatic necrosis
- Liver transplantation for liver failure in kidney transplantation recipients with hepatitis B virus infection
- Transjugular portosystemic shunt for early-onset refractory ascites after liver transplantation
- Giant pseudoaneurysm of the splenic artery within walled of pancreatic necrosis on the grounds of chronic pancreatitis
- Hepatic isolated ectopic adrenocortical adenoma mimicking metastatic liver tumor