
Angioimmunoblastic T-cell lymphoma accompanied by pure red cell aplasia: A case report
2021-01-14 03:02:12TeikoKawahigashiIzumiKitagawaEriTanaka
Teiko Kawahigashi, Izumi Kitagawa, Eri Tanaka
Teiko Kawahigashi, Izumi Kitagawa, Department of General Internal Medicine, Shonan Kamakura General Hospital, Kanagawa 247-8533, Japan
Eri Tanaka, Department of Hematology, Shonan Kamakura General Hospital, Kanagawa 247-8533, Japan
Abstract BACKGROUND Angioimmunoblastic T-cell lymphoma (AITL) is a peripheral T-cell lymphoma,which is a rare subtype of lymphoma. Patients with AITL often have skin lesions,which are observed in 50% of all cases; the chief complaint of this patient was palpable purpura. AITL often complicates autoimmune or hematological disorders; however, among these, pure red cell aplasia (PRCA) is a very rare complication of AITL. We herein report a case of AITL with PRCA.CASE SUMMARY A 77-year-old Japanese man presented to our hospital with complaints of loss of appetite for 2 mo and a 10-d history of palpable purpura. On physical examination, the patient was afebrile but had bilateral multiple palpable purpuric lesions over the lower extremities, lower abdomen, and part of the upper extremities. Moreover, lymphadenopathy of the bilateral inguinal, cervical, and supraclavicular nodes was noted. Laboratory and imaging studies and skin biopsy were conducted but were inconclusive. Based on inguinal lymph node excisional biopsy, we diagnosed the patient with AITL. Subsequently, the patient developed progressive normocytic normochromic anemia that necessitated almost daily blood transfusion. The clinical presentations and results of bone marrow assessment were consistent with those of PRCA, which is associated with AITL. Chemotherapy was initiated but was not effective. The patient refused further chemotherapy and opted to continue receiving best supportive care.CONCLUSION PRCA is an extremely rare complication of AITL. As the pathophysiology remains unclear, further research is warranted.
Key words: Palpable purpura; Lymphoma; Pure red cell aplasia; Case report
INTRODUCTION
Angioimmunoblastic T-cell lymphoma (AITL) is an uncommon subtype of peripheral T-cell lymphoma, which comprises 1%-2% of all non-Hodgkin lymphomas[1].Cutaneous involvement is one of the most important presentations of AITL and is seen in up to 50% of cases. Our case showed palpable purpura[2]. Our patient not only developed a rare subtype of lymphoma, AITL, but also its very rare complication,pure red cell aplasia (PRCA).
CASE PRESENTATION
Chief complaints
A 77-year-old Japanese man presented to our hospital with complaints of loss of appetite for 2 mo and a 10-d history of palpable purpura.
History of present illness
The patient had developed progressive palpable purpura over his lower legs (Figure 1) without fever, chills, or other clinical signs.
History of past illness
The medical history included hypertension, hyperlipidemia, old myocardial infarction, and appendicitis. The patient was on regular treatment with medications,including aspirin, lansoprazole, enalapril, valsartan, and carvedilol. He had no notable family or social history.
Personal and family history
His family history was noncontributory.
Physical examination upon admission
On physical examination, the patient’s vital signs were normal: blood pressure,102/58 mmHg; heart rate, 94 bpm; and percutaneous oxygen saturation, 99% in room air. However, multiple palpable purpuric lesions were noted on bilateral lower extremities, the lower abdomen, and part of the upper extremities (Figure 1).Lymphadenopathy was noted in bilateral inguinal, cervical, and supraclavicular nodes, measuring up to 1 cm in diameter. No clinically relevant abnormalities were observed on the electrocardiogram and chest radiograph.
Laboratory examinations
Laboratory data on admission was shown in Table 1: White blood cells and platelet counts were normal but normocytic normochromic anemia was seen. An elevated level of serum lactate dehydrogenase has been found. Although several abnormalities were observed, none of them were specific to the diagnosis.
Further diagnostic work-up
We performed skin biopsy, which demonstrated superficial perivascular dermatitis.However, this did not help in diagnosis. Subsequently, a right inguinal lymph node excisional biopsy was performed, which showed vascular proliferation with high endothelial cells, including small-to-medium-sized atypical lymphocytes and follicular dendritic cells. Immunohistochemical analysis revealed the expression of Tcell markers (CD2, CD3, CD4, and CD5) with CD10. These characteristics were consistent with those of AITL.

Figure 1 Palpable purpura on the lower extremities.
Subsequently, several days after hospitalization, the patient developed progressive normocytic normochromic anemia. His hemoglobin levels remained much lower than normal at 4.9-6.0 g/dL, with normal white blood cell and platelet counts, similar to those on admission. His absolute reticulocyte count also remained extremely low at less than 10000/μL, necessitating blood transfusion support almost every day.Peripheral blood smear examination revealed a normochromic normocytic picture and there was no evidence of hemolysis. We performed bone marrow aspiration and biopsy for evaluation, which showed characteristic findings of relative erythroid hypoplasia. The myeloid and lymphoid series were essentially unremarkable,whereas the megakaryocytes were slightly increased in number and had normal morphology. Based on these findings, the patient was diagnosed with PRCA.
FINAL DIAGNOSIS
AITL and PRCA associated with AITL.
TREATMENT
Chemotherapy every 3 wk was urgently initiated with intravenous cyclophosphamide at 750 mg/m2, doxorubicin at 50 mg/m2, and vincristine at 1.4 mg/m2on day 1 with oral prednisone at 60 mg/d from days 1 to 5(cyclophosphamide, doxorubicin, vincristine, and prednisone). However,chemotherapy offered limited clinical benefit with partial regression of the lymphadenopathy; moreover, blood transfusions were required almost every day.
OUTCOME AND FOLLOW-UP
The patient refused further chemotherapy in view of his age and disease status, and opted to continue with best supportive care, including a blood transfusion, at another local hospital.
DISCUSSION
Skin lesions are one of the most important manifestations of AITL, affecting the skin in approximately 50% of cases. This poses a diagnostic challenge, particularly before obtaining lymph node biopsies[2]. In this case, although there was no evidence of tumor cell involvement and our institutional pathologist did not mention the possibility of lymphoma in the skin biopsy report, a negative skin biopsy is often observed in AITL patients with skin lesions. Previous reports showed the histological findings of AITL cutaneous lesions can be quite variable[3]. Martelet al[3]described several histological findings of AITL, such as vasculitis without lymphocyte cytological atypia. Palpable purpura of our patient can also be one of the manifestations of lymphoma because there are no other special reasons for it.
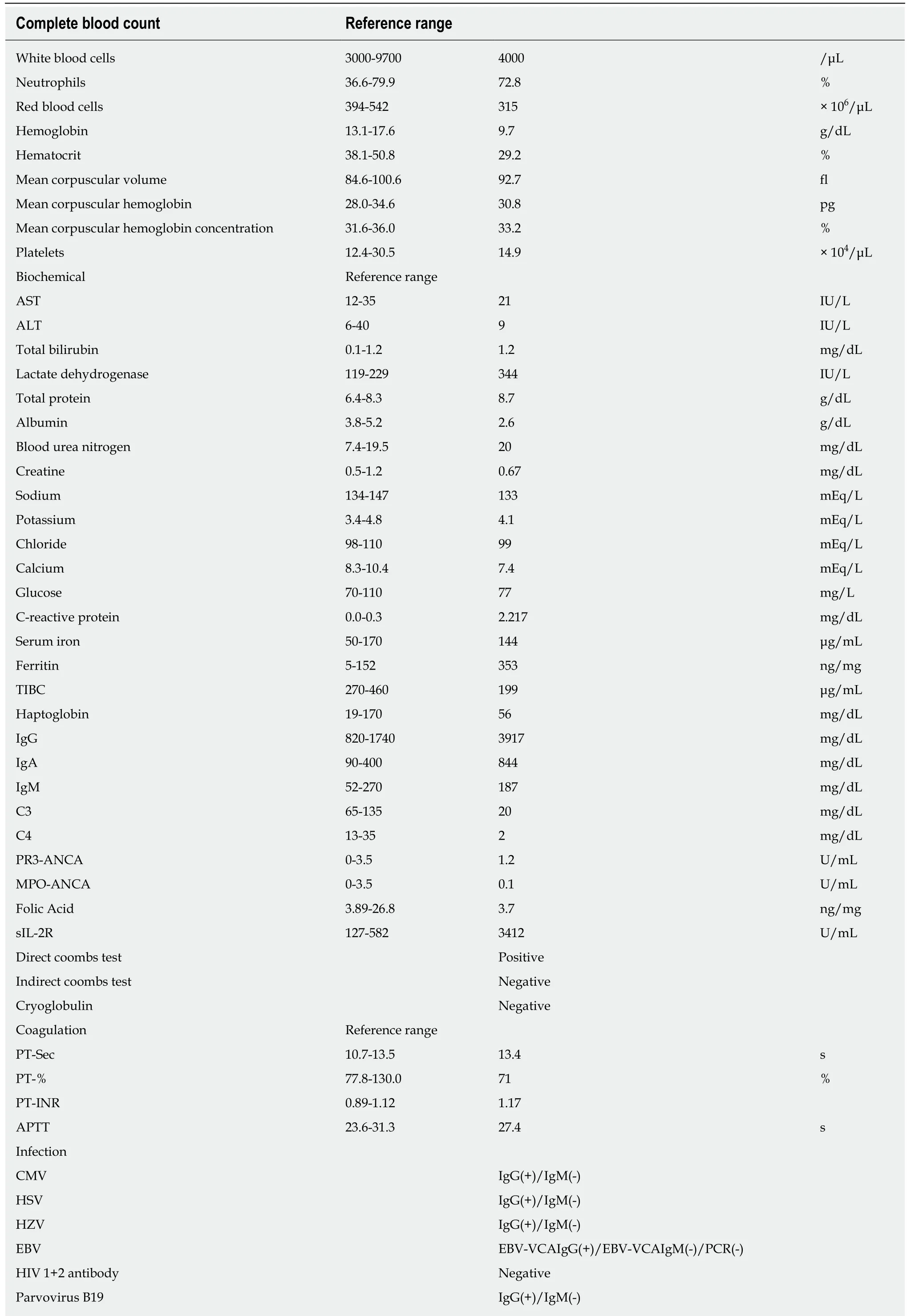
Table 1 Laboratory examinations
If AITL was suspected, immunohistological studies might help; some immunological markers, such as CXCL13, PD-1, Bcl-6, and CD10, are known to be seen in AITL[1,2]. As a matter of course, lymph node biopsy is the most important tool for diagnosis. Although immunohistological studies of our case did not show any of these markers, except for CD10, we diagnosed AITL owing to its characteristic pathological findings, namely, high endothelial cell venules and follicular dendritic cells[1]. In addition, this patient was diagnosed with PRCA. The following criteria are used to diagnose PRCA: Normocytic normochromic anemia, absolute reticulocyte count < 10000/μL (or reticulocyte percentage < 0.5%), normal white blood cell and platelet counts, in the absence of concurrent disorder, normocellular bone, with erythroblasts total < 1%, no significant abnormalities in the myeloid, lymphocytic, or megakaryocyte lineages. Meeting all of these criteria results in a diagnosis of PRCA and our patient met all of them[4].
Patients with lymphoma appear to have an increased risk of various autoimmune conditions, both hematological and non-hematological[5]. Among them, AITL is often accompanied by various immunological and hematological diseases, such as autoimmune hemolytic anemia (AIHA), vasculitis, and autoimmune thyroid disease[6].This may be associated with the fact that AITL is thought to arise from CD4+ T-cells,which play an important role in the adaptive immune system, especially within the germinal centers[7]. Clonal rearrangements of T-cell receptor genes have already been demonstrated in most cases of AITL[7]. However, previous reports suggested that not only disturbance of the T cellular immunity but also proliferation of B cells contribute to the histologic and clinical picture in most cases[7]. One study showed that neoplastic T cells may promote antibody production by B-cells through excessive cytokine release. They demonstrated that the immune system in AITL is substantially activated, and an array of cytokines, such as interferon gamma, interleukin (IL)-6, IL-12, and tumor necrosis factor-alpha, are upregulated[8]. Because of this immune system dysregulation, we suppose that small amounts of antigens are sufficient to initiate an inflammatory reaction[8]. Multiple interactions among T-cell, B-cells, and multiple cytokines would contribute to the abnormal immune reaction in AITL.
PRCA, an autoimmune disorder resulting in isolated depletion of the erythroid series, has been reported in association with AITL, but it is extremely rare[6,9]. A PubMed search yielded just a few additional reported cases of PRCA associated with AITL and they are summarized in Table 2 (10 reports were found, but 3 were excluded due to lack of availability of the full-text article). Interestingly, previous reports have demonstrated that almost all patients showed a positive direct Coombs test[6], which suggests an autoreactive antibody role[9]; this coincides with the positive test result found in our patient. In this case, a coexisting AIHA should be considered because of the severe anemia and positive direct Coombs test. However, we do not think that the patient has AIHA, based on the clinical findings: First, there was no evidence of hemolysis, such as jaundice, splenomegaly, elevated levels of indirect bilirubin, and decreased levels of haptoglobin. Second, the peripheral blood smear findings were not consistent with those of AIHA. There was no evidence of hemolysis or microspherocytosis. Third, the patient’s other clinical findings were not consistent with those of AIHA. For example, he showed a very low absolute reticulocyte count and near-complete absence of erythroblasts from an otherwise normal marrow. Those findings were inconsistent with AIHA. In patients with PRCA, cyclosporine A should be routinely prescribe, although we did not do so. Previous reports have suggested that PRCA associated with AITL is improved only with the treatment of AITL, which is chemotherapy[5,6,9]. Therefore, we started treatment with chemotherapy for AITL,but no direct treatment of PRCA. However, the chemotherapy was not sufficiently effective for this patient, for both AITL and PRCA. Further research is needed to investigate optimal treatment strategies for the management of these patients.
The pathogenesis remains uncertain because of the limited number of reported cases of PRCA with AITL[6,9], although it is reasonable to assume the possibility of multifactorial pathogenic involvement. Previous reports have suggested that AITL might trigger autoimmune alterations that lead to PRCA[5]. Another study demonstrated that malignant B-cell clones might produce autoreactive antibodiesagainst erythroid progenitors, and neoplastic T-cells might directly or indirectly inhibit the erythroid differentiation of hematopoietic stem cells[9].
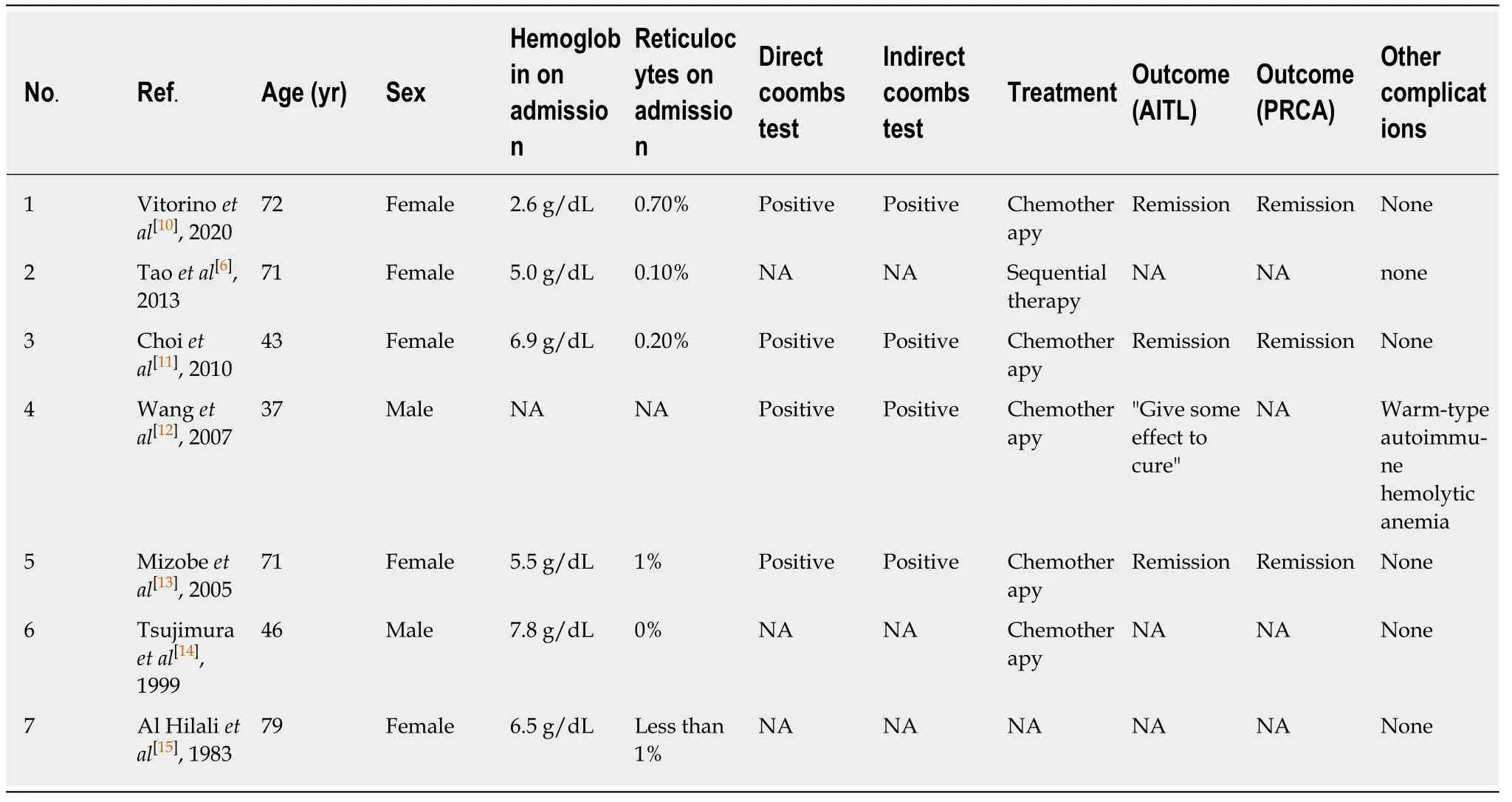
Table 2 Summaries of previous case reports of pure red cell aplasia associated with angioimmunoblastic T-cell lymphoma
CONCLUSION
Owing to its rarity and nonspecific symptoms, the diagnosis of AITL is often challenging. It is sometimes misdiagnosed as an infection or another hematological disease. Detailed and specific diagnostic investigations, including excisional biopsies of lymph nodes, may be useful. Furthermore, the etiopathogenesis of PRCA is of interest, because the mechanisms underlying lymphoma-associated PRCA have not yet been elucidated. Therefore, further case studies and laboratory-based research is necessary to ascertain the pathogenesis of PRCA in AITL.
 World Journal of Clinical Oncology2020年6期
World Journal of Clinical Oncology2020年6期
- World Journal of Clinical Oncology的其它文章
- Immune response activation following hyperthermic intraperitoneal chemotherapy for peritoneal metastases: A pilot study
- National Comprehensive Cancer Network guidelines compliance of a sarcoma service: A retrospective review
- Preoperative markers for the prediction of high-risk features in endometrial cancer
- Role of microRNA dysregulation in childhood acute leukemias:Diagnostics, monitoring and therapeutics: A comprehensive review
- Lingual lymph nodes: Anatomy, clinical considerations, and oncological significance
- Active surveillance in low risk papillary thyroid carcinoma