
Case fatality rate of coronavirus disease 2019 (COVID-19) in Iran-a term of caution
2020-07-21 01:06:38VahidRahmanianMohammadHasanRabieeHamidSharifi
Vahid Rahmanian, Mohammad Hasan Rabiee, Hamid Sharifi
1Zoonoses Research Center, Jahrom University of Medical Sciences, Jahrom, Iran
2Department of Epidemiology, Faculty of Veterinary Medicine, University of Tehran, Tehran, Iran
3HIV/STI Surveillance Research Center, WHO Collaborating Center for HIV Surveillance, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
Coronavirus disease 2019 (COVID-19) has spread to 72 countries by the time of writing this report on 4th March 2020[1]. On 20th February 2020, the first two confirmed deaths from COVID-19 were reported in Iran. Till 4thMarch 2020, 2 922 confirmed and 92 death cases have also been reported till 4th March 2020 in Iran(Figure 1)[1].
A key question that remains unanswered or controversial among the public, media, and researchers is the exact COVID-19 case fatality rate (CFR) in Iran. Why does the CFR in Iran appear to be higher compared to the rest of the world until now? Or why the fatality rate is high at the beginning of the epidemic in Iran?
For an epidemic of an emerging disease such as COVID-19,CFR is one of the most important epidemiological values. Little knowledge regarding various methods to estimate the CFR and their limitations can lead to misleading and misinterpretations and eventually may lead the decision-makers to make the wrong decisions.
In general, the fatality rate is calculated as follows[2]:
Case fatality (%)=(No. of deaths of individuals during a specific period of time after disease onset or diagnosis)/(No. of individuals with the specified disease)×100
At the beginning of the COVID-19 epidemic in Iran, it is tempting to calculate the CFR by the above formula. However, a simple statistical analysis of the mortality rate obtained from these reports would be misleading if, at the time of analysis, the outcome of a negligible proportion of patients is unknown (detection bias). Generally, this bias can happen as a result of a systematic error during screening,evaluation, diagnosis and outcome confirmation[3].
This means that COVID-19 patients with mild symptom or asymptomatic cases are not diagnosed. The current situation is like an iceberg which its tip is only visible and just the clinical symptoms are apparent. But infections without clinical symptoms are also important,particularly in the network of disease transmission[2]. Therefore, the simple calculation at the onset of the epidemic does not represent the true CFR and might be overestimated[4].
Time interval between detection and death/recovery and the degree of underreporting will vary over time as well as between cities and countries. It is currently impossible to estimate precisely the CFR in Iran. Figure 2 illustrates this uncertainty.
At the beginning, the CFR may also be overestimated. For instance,in a study using the database of Jin Yin-tan Hospital and Tongji Hospital in Wuhan, they conducted a retrospective multi-center study of 68 death cases (68/150, 45%) with laboratory-confirmed infection of COVID-19[5]. In the other studies by Huanget al.and Chenet al.in Wuhan, CFR was estimated to be 15% up to 2nd February and 11%up to 20th February, respectively[6,7]. In a report of 72 314 cases from the Chinese Center for Disease Control and Prevention updated on 11th February, the overall CFR was reported to be 2.3%[8]. Variations in mortality in the current epidemic in China supports our analysis and inference.
The comparison of CFR between different countries and regions is questionable[4] because the number of cases screened by the surveillance systems can affect the denominator of the fatality fraction (see the above equation). In an area where the active surveillance system with mass screening could be performed, the CFR could be lower. But due to economic, cultural and other factors,it is impossible to implement an active surveillance system in some areas and resultantly CFR could be overestimated..
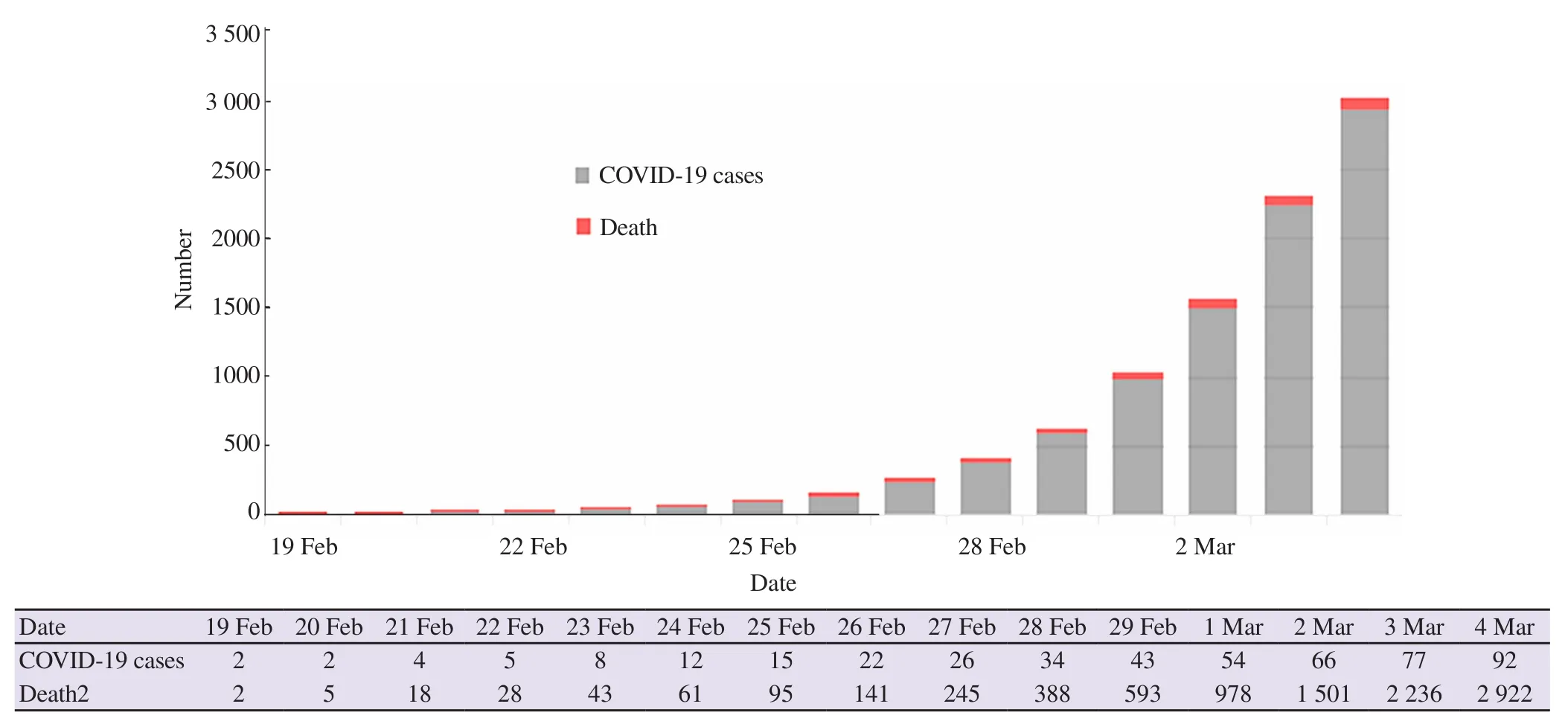
Figure 1. Frequency distribution of confirmed cases and deaths of COVID-19 in Iran on 4th March 2020.
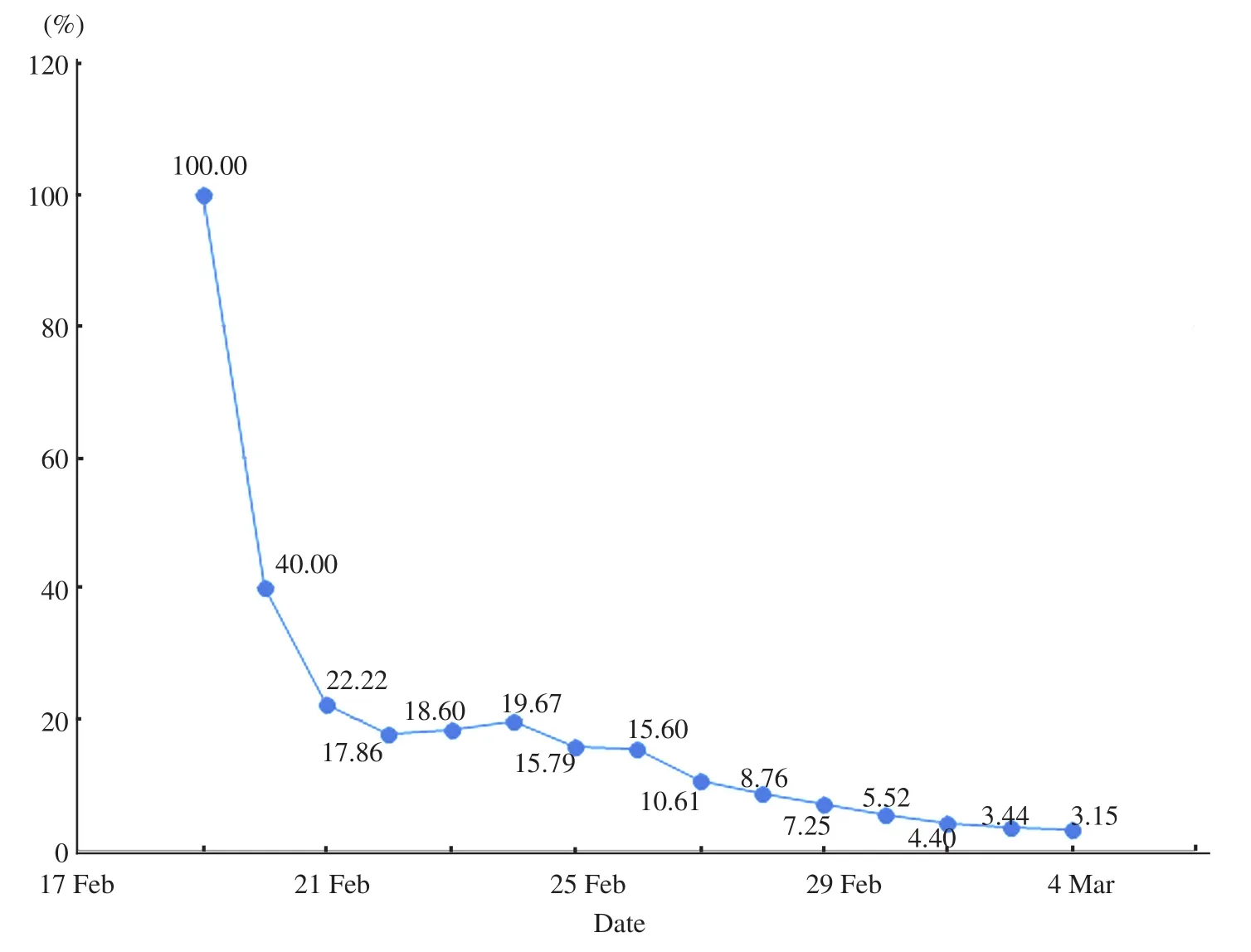
Figure 2. Frequency distribution of CFR of COVID-19 in Iran on 4th March 2020.
The sensitivity of diagnostic tests may vary along with the development of the disease[3,9]. Depending on the stage of the disease and the disease course, different diagnostic test should be performed.In addition, considering the heterogeneous population such as age, underlying disease,etc. in different countries and regions, it is recommended to calculate and interpret CFR for various subgroups. As the study of China with 72 314 cases, the overall fatality rate was reported to be 2.3%, 14.8% in patients aged≥80 years, 8.0% in patients aged 70-79 years and 49.0% of critical cases[8]. Accurate estimate and analysis of the trends in the proportion of deaths can be used to evaluate the effectiveness of new treatments. In conclusion, number of undiagnosed mild or asymptomatic cases, type of surveillance system, the sensitivity of diagnostic tests and population heterogeneity can affect the fatality rate. Therefore, the interpretation of the fatality rate at the beginning of an epidemic should be cautious, and the estimates will be close to actual at the end of the epidemic.
Eventually, it is highly recommended to use various methods and compare them with the current methods. For example, prediction of the fatality rate using the modified Kaplan-Meier estimator enables us to consider censored data and thus be able to detect changes more rapidly at the beginning of the epidemic.
Acknowledgements
Hereby, the authors extend their gratitude to the research deputy of Jahrom University of Medical Sciences for financial support and confirmation of the project (Project identification code IR.JUMS.REC.1398.120).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Authors’ contributions
VR, and MR conceived and designed the study. VR, and MR were responsible for literature search and screening. MR were responsible for data collection and analyses. VR, MR, contributed to data interpretation. VR and MR drafted the manuscript and HSH,critically revised the manuscript.
 Asian Pacific Journal of Tropical Medicine2020年7期
Asian Pacific Journal of Tropical Medicine2020年7期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Will Africa experience a spike in COVID-19 cases?
- Effect of the Songkran festival on COVID-19 transmission in Thailand
- Leishmania donovani infection in Eastern Sudan: Comparing direct agglutination and rK39 rapid test for diagnosis-a retrospective study
- Predicting factors contributing to knowledge, attitudes and practices relating to Zika virus infection among the general public in Malaysia
- Prevalence and genotype distribution of Enterobius vermicularis among kindergarteners in Shiraz and Khorramabad cities, Iran
- Seroprotection after hepatitis B vaccination amongst infants aged between 12 and 24 months in Ho Chi Minh City, Vietnam