Adaptive radiation therapy of breast cancer by repeated imaging during irradiation
2020-06-15 06:29:16OmerSagerFerratDincoglanSelcukDemiralBoraUysalHakanGamsizFatihOzcanOnurhanColakYeldaElcimEsinGundemBaharDiricanMuratBeyzadeoglu
World Journal of Radiology 2020年5期
Omer Sager,Ferrat Dincoglan,Selcuk Demiral,Bora Uysal,Hakan Gamsiz,Fatih Ozcan,Onurhan Colak,Yelda Elcim,Esin Gundem,Bahar Dirican,Murat Beyzadeoglu
Abstract
Key words: Breast cancer;Adaptive radiation therapy;Tumor bed boost;Computed tomography;Imaging;Replanning
INTRODUCTION
Breast cancer is the most frequent cancer among females and also a leading cause of cancer related mortality worldwide. A multimodality treatment approach may be utilized for optimal management of patients with combinations of surgery,radiation therapy (RT) and systemic treatment. RT composes an integral part of breast conserving treatment (BCT),and is typically used after breast conserving surgery(BCS) to improve local control. Recent years have witnessed significant improvements in the discipline of radiation oncology which allow for more focused and precise treatment delivery. Adaptive radiation therapy (ART) is among the most important RT techniques which may be utilized for redesigning of treatment plans to account for dynamic changes in tumor size and anatomy during the course of irradiation. In the context of breast cancer,ART may serve as an excellent tool for patients receiving breast irradiation followed by a sequential boost to the tumor bed. Primary benefits of ART include more precise boost localization and potential for improved normal tissue sparing with adapted boost target volumes particularly in the setting of seroma reduction during the course of irradiation. Herein,we provide a concise review of ART for breast cancer in light of the literature.
MASTECTOMY AND BREAST CONSERVING TREATMENT FOR BREAST CANCER MANAGEMENT
Both mastectomy and BCT are widely used therapeutic options for management of patients suffering from breast cancer. Selection of surgical modality as BCS or mastectomy is based on several factors including patient and tumor characteristics,assessment of outcomes in terms of cosmesis,treatment morbidity and local control,and patient preferences. In terms of efficacy,BCT and mastectomy provide comparable results which have been supported by data from randomized trials and collaborative group studies. In this context,BCT has been alternatively used for management of patients with breast cancer. Recent studies also support the utility of BCS and RT as a viable alternative to mastectomy with encouraging results.
UTILITY OF RADIATION THERAPY AS PART OF BREAST CONSERVING TREATMENT
Use of RT as part of BCT is increasing in line with accumulating evidence and improvements in the discipline of radiation oncology including sophisticated delivery techniques and modernized treatment equipment. Although omission of RT after BCS may be considered for a very highly selected subgroup of patients given the relatively lower local recurrence rates after BCS and endocrine treatment,RT is widely recognized as an integral part of BCT particularly to decrease the rates of local recurrence.
CONVENTIONALLY FRACTIONATED RADIATION THERAPY OF THE INTACT BREAST: TO BOOST OR NOT TO BOOST
Irradiation of the intact breast with conventionally fractionated RT as part of BCT typically includes whole breast irradiation (WBI) followed by a sequential tumor bed boost directed at the lumpectomy cavity. Main rationale of adjuvant RT following BCS is reduction of local recurrence. Utility of RT for breast cancer management has been assessed in a comprehensive metaanalysis. This metaanalysis reported a substantial reduction in the 10-year first recurrence rate from 35% to 19.3%,and incorporation of adjuvant RT also resulted in a breast cancer survival gain of 3.8% at 15 years,suggesting substantial benefit of adding RT after surgical management.Since local recurrence comprises a critical pattern of recurrence for breast cancer patients affecting prognosis,achieving durable local control rates is a pertinent goal of management. Given the tendency of breast tumors to recur primarily at the original tumor site,delivery of a boost RT dose to the lumpectomy cavity has been utilized for achieving improved local control rates. Rationale for boost RT includes elimination of microscopic tumor cells located at the primary tumor site to improve local control. Delivery of boost dose to the lumpectomy cavity may be performed by use of several techniques including external photon beams,external electron beams,and brachytherapy.
DEFINITION OF THE BOOST TARGET VOLUME
Definition of the boost target volume is a critical component of breast cancer RT.Surgical scar and clips,ultrasonography,mammography,Computerized Tomography(CT),Magnetic Resonance Imaging (MRI),clinical examination findings may be incorporated for determining the localization of tumor bed boost. However,there is no consensus on this critical issue with wide variations among clinical practices worldwide. Clearly,all methods have their advantages and drawbacks which renders a complementary or integrative approach more feasible to achieve precise target volume localization.
THE CONCEPT OF ADAPTIVE RADIATION THERAPY
ART refers to redesigning of treatment plans with respect to dynamic changes in tumor size and anatomy during the course of irradiation. There have been several applications of ART for a variety of indications including breast cancer,head and neck cancers,prostate cancer,and several other cancers throughout the human body.Primary objective of ART is achieving an improved therapeutic ratio. Accounting for volumetric and anatomical changes during the course of irradiation has great potential for improving treatment outcomes. This pertinent goal of RT may be achieved by incorporating smaller boost target volumes when substantial reduction in tumor burden is confirmed on periodical imaging during the RT course. Indeed,this rationale has been tested in the setting of RT after induction chemotherapy for limited-stage small cell lung cancer. The authors concluded that irradiation of the postchemotherapy volumes instead of baseline prechemotherapy volumes did not decrease locoregional control. While chemotherapy may confer substantial shrinkage of tumor volumes particularly for chemosensitive cancers,RT may also achieve reduction in tumor burden which may be exploited by use of ART techniques.Besides tumor shrinkage,replanning for boost RT may provide additional advantages for precise target localization accounting for the potential changes in patient anatomy due to weight loss or edema.
ADAPTIVE RADIATION THERAPY OF THE INTACT BREAST BY REPEATED IMAGING DURING THE COURSE OF IRRADIATION
For breast cancer patients receiving conventionally fractionated RT over 5-6 wk followed by a sequential tumor bed boost,ART may be utilized for more precisely focused boost RT. Replanning for the tumor bed boost may prevent excessive normal tissue exposure particularly for patients having seroma at the initiation of WBI.Several studies have reported on volumetric changes in the lumpectomy cavity during te course of breast irradiation. Data from selected studies incorporating ART for breast cancer by use of repeated imaging during the course of breast irradiation are summarized in Table 1.
A consistent finding of the aforementioned studies is the dynamic nature of the tumor bed during the course of breast irradiation. In this context,ART may be exploited to optimize normal tissue sparing particularly in the presence of substantial seroma reduction during RT by using reduced boost target volumes. Another potential benefit of repeated imaging may be avoidance of boost localization inaccuracies due to dynamic changes during the course of breast irradiation which may allow for improved precision in boost RT. These potential benefits of ART should be considered thoroughly for management of patients with breast cancer to achieve an improved therapeutic ratio. Figure 1 shows axial CT images of a patient acquired at initial CT-simulation (on the left) for WBI planning and repeated CT-simulation (on the right) for tumor bed boost planning.
CONCLUSION
ART with repeated imaging during the course of irradiation may serve as an excellent tool for patients receiving breast RT followed by a sequential boost to the tumor bed.Utility of ART with widely accepted hypofractionated breast irradiation protocols,frequency of imaging for treatment plan adaptation,selection of patients for ART or routinization of the technique for every patient are areas of active investigation. There is accumulating evidence supporting the utility of ART for breast cancer management,however,future trials are needed for validation of dosimetric and clinical results of ART with repeated imaging at different time points during the course of breast irradiation.
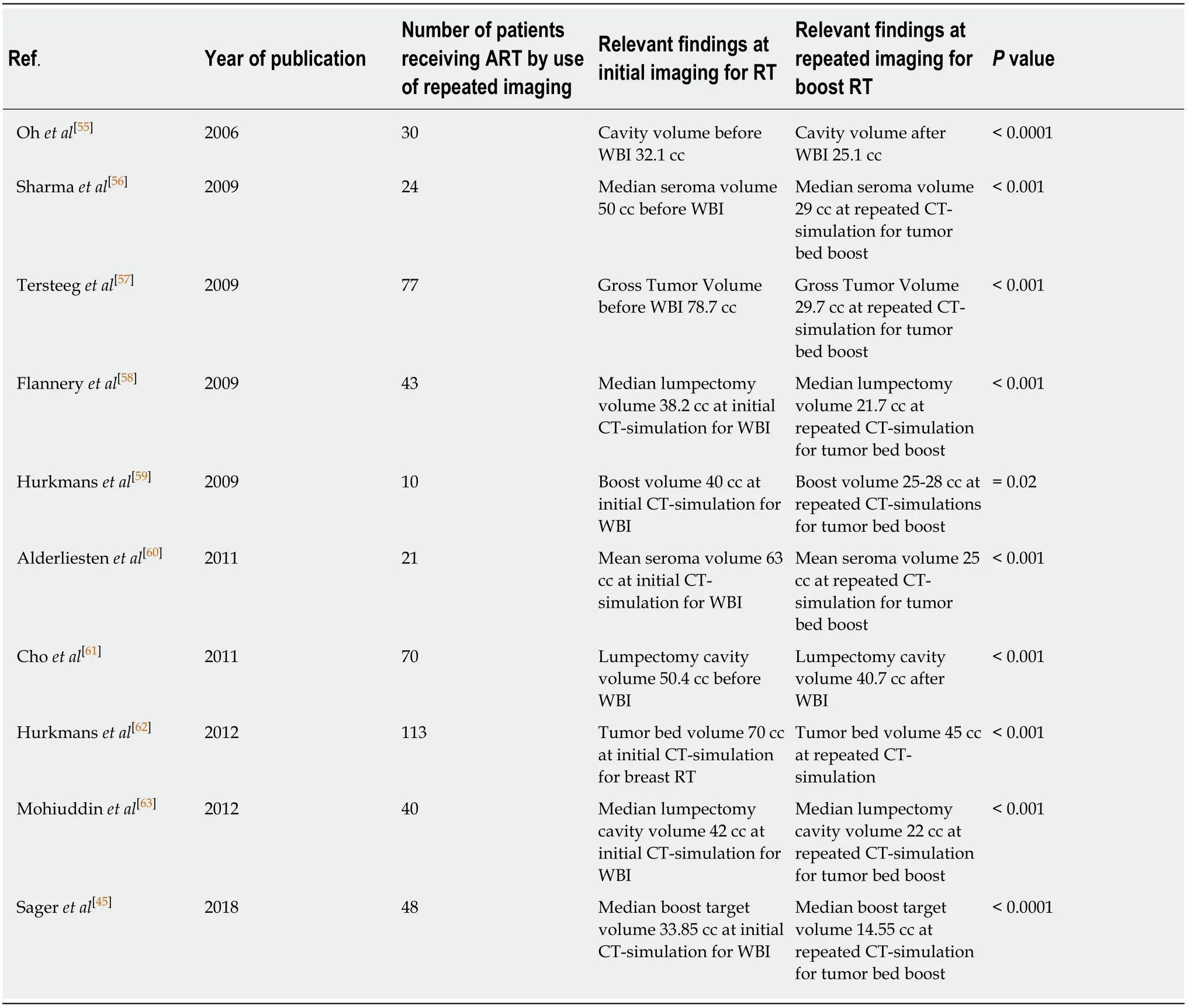
Table1 Selected studies incorporating adaptive radiation therapy for breast cancer by use of repeated imaging during the course of breast irradiation
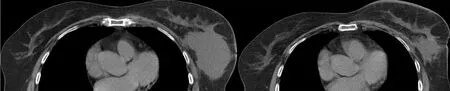
Figure1 Axial computed tomography images.