
Thoracic hydatid disease:A radiologic review of unusual cases
2020-04-23 06:03:54MnahiBinSaeedanIbtisamMusallamAljohaniKhalefaAliAlghofailyShukriLoutfiSubhaGhosh
World Journal of Clinical Cases 2020年7期
Mnahi Bin Saeedan,Ibtisam Musallam Aljohani,Khalefa Ali Alghofaily,Shukri Loutfi,Subha Ghosh
Mnahi Bin Saeedan,lbtisam Musallam Aljohani,Department of Radiology,King Faisal Specialist Hospital and Research Center,King Faisal Specialist Hospital and Research Center,Riyadh 11211,Saudi Arabia
Khalefa Ali Alghofaily,Medical Imaging Department,Qassim University,College of Medicine,Buraydah 52571,Saudi Arabia
Shukri Loutfi,Medical Imaging Department,Chest Radiology Section,King Abdulaziz Medical City,Riyadh 12746,Saudi Arabia
Subha Ghosh,Imaging Institute,Section of Thoracic Imaging,Cleveland Clinic,Cleveland,OH 44195,United States
Abstract
Key words: Hydatid;Thoracic;Cysts;Imaging;Unusual;Extra-pulmonary
INTRODUCTION
Hydatid disease or echinococcosis is a zoonotic disease transmitted from animals to humans.It is caused by tapeworm parasites and most prevalent in rural sheep-raising areas of the Middle East,Mediterranean regions,South America,Africa,Australia,and New Zealand.Human disease is most commonly caused by echinococcus granulosus and rarely echinococcus multilocularis.Dogs and sheep are the most common primary and intermediate hosts respectively,and human transmission is caused after ingestion of food or water contaminated with the parasite's eggs,or by direct handling of animal hosts[1-3].
Hydatid disease may affect any organ-system and anatomical site of the human body.The liver is most commonly affected site in about 75% of cases followed by the lungs.Hydatid cysts may cause symptoms due to direct mass effect or complications related to cyst rupture or superinfection[1,2].Cyst rupture may result in life-threatening anaphylactic reactions due to the antigenic properties of the cyst fluid[3,4].Intrathoracic and extra-pulmonary hydatid disease is uncommon and may involve the pleura,mediastinum,heart,diaphragm,and chest wall[1,2].
Unusual locations or complications of hydatid disease in the chest may pose a diagnostic challenge or influence treatment options.The aim of this article is to review imaging findings of unusual locations and complications of hydatid disease involving the chest with emphasis on clinical implications.
HYDATID CYST STRUCTURE AND PATHOGENESIS
Understanding the structure of Hydatid cyst and review of the parasite's life cycle is relevant to understanding imaging findings and pathogenesis of disease spread.Hydatid cyst is composed of the outer pericyst,the middle ectocyst,and the inner endocyst.The outer pericyst is a dense fibrous protective shell around the parasite that is formed by the reactive inflammatory host tissue.The acellular elastic laminated middle membrane is the ectocyst.The endocyst is the inner single germinal epithelial layer.The endocyst may form internal protrusions that eventually become daughter cysts within the larger mother cyst[1,3].
The echinococcus granulosus life cycle requires both a definitive canine host (most commonly dogs) and an intermediate host (usually sheep).Echinococcus granulosus eggs are excreted into the host faeces.Humans can become accidental hosts after ingesting food or water contaminated with parasite eggs.The larvae get released from the ingested eggs and gain access to the liver through the intestinal mucosa via mesenteric veins and the portal vein.About 75% of hydatid infections affect the liver.In about 15% of the cases,larvae bypass the liver filtration to gain access to the lungs.Hematogenous spread of echinococcus granulosus to any part of the body can also occur[1,3].
CLINICAL OVERVIEW OF EXTRAPULMONARY AND INTRATHORACIC HYDATID CYSTS
The extrapulmonary intrathoracic hydatid cysts may be silent with no symptoms and may present with symptoms commonly related to mass effect and compression of adjacent organs.Hydatid cyst rupture can cause anaphylactic shock and even death.Imaging findings of hydatid cysts are variable,ranging from purely cystic lesions to solid appearing lesions.Diagnosis of such cases can be challenging and usually based on clinical data including history of exposure or immigration from endemic area as well as supportive radiologic and serology findings[2,5,6].Casoni's intradermal skin test and indirect haemagglutination test (IHA) may detect the presence of antibodies to the parasite.Casoni's intradermal test is still used for its simplicity,though it has a variable sensitivity (57%-93%) and limited specificity.The IHA test is one of the most sensitive serological tests for the diagnosis of hydatid disease.IHA test reported sensitivity ranging from 66% to 100% and it is used as a screening test[7].Percutaneous transthoracic aspiration should be avoided or performed with caution,because it may result is allergic reactions or cause spreading of disease.Surgical removal of hydatid cyst is the treatment of choice for most patients.Medical therapy with mebendazole or albendazole is used as a complement to surgical treatment.Medical therapy is a primary treatment in patients with recurrent hydatidosis,patients who may not tolerate surgery,or patients with small cysts[5,6].
IMAGING FINDINGS
Hydatid cysts are generally classified into four types based on their imaging appearance[2].
Type I or simple cysts
Simple hydatids cysts appear as well-defined and anechoic masses on ultrasound and may include hydatid sand and septa.On computed tomography (CT),they are homogeneous lesions of fluid attenuation.On magnetic resonance imaging (MRI),simple hydatid cysts show fluid signal intensity with homogeneous low signal on T1-weighted images and high signal on T2-weighted images,and have a dark rim on both sequences.
Type II or cysts with daughter cysts and cyst matrix
Daughter cysts appear as smaller cysts within the largest mother cyst.On imaging,daughter cysts are commonly located peripherally within the mother cyst.Daughter cysts tend to be lower in attenuation on CT and iso-intense or hypointense compared to the maternal matrix.Occasionally,daughter cysts can be irregular in shape and occupy most of the mother cyst.The higher attenuation surrounding maternal matrix fluid may resemble septae,resulting in a “rosette” appearance.
Type III or calcified cysts
Total calcification of hydatid cysts reflects death of hydatid cysts.Calcifications appear as echogenic areas on ultrasound with posterior shadowing,hyperattenuated areas on CT,and hypo-intense areas on MRI.
Type IV or complicated Cysts
Complications of hydatid cysts include rupture and/or superinfection.Cyst degeneration,response to treatment,or trauma are suggested etiologies of cyst rupture.Hydatid cyst rupture can be contained or communicate with surrounding structures.In contained rupture,floating membranes can manifest as serpentine linear structures of low attenuation on CT and low signal on MRI within the cyst matrix.This imaging sign is highly suggestive of hydatid cyst and has earned the moniker‘‘water-lily sign''.The presence of intra-cystic air suggests direct or communicating rupture with or without superimposed infection.
MEDIASTINAL HYDATID CYST
Hydatid cyst involving the mediastinum is very uncommon with reported incidence of 2.6% in patients with hydatid disease.Mediastinal hydatid cysts can be primary with no evidence of other organ involvement or a result of ruptured lung hydatid cyst[8].Primary intra-thoracic extra pulmonary hydatid cyst can be explained by hematogenous spread of hydatid scolices that bypass the filtration processes in both liver and lung,or via diaphragmatic lymphatic drainages to parasternal lymph nodes anteriorly or intercostal lymph nodes posteriorly[9].
The mediastinal hydatid cysts can cause symptoms depending on the size and location of the cyst and the involvement or mass effect on adjacent structures.Presenting symptoms are non-specific and may include chest pain,cough,shortness of breath,and dysphagia.Chest pain is reported as a common presenting symptom of mediastinal hydatid cysts.Hydatid cysts can be solitary or multiple and can involve anterior,middle,or posterior mediastinal compartments,though the posterior mediastinum is most commonly affected[8].
Cross sectional imaging with CT and MRI provides valuable diagnostic information about the cysts including morphologic features,densities,signal changes,locations,and relationship with surrounding structures.On imaging,hydatid cysts in the mediastinum can have variable imaging appearances ranging from unilocular cyst to multivesicular cyst with or without calcification.Calcifications are better detected on CT.The inherent superior contrast resolution of MRI for cystic lesions makes it invaluable in assessing for the presence of daughter cysts and resolving them from the mother cyst matrix (Figure 1)[2].
Hydatid disease should be considered in the differential diagnosis of mediastinal cystic lesion especially in patients from an endemic area or if associated with hydatid cysts elsewhere in the body[8].Hydatid cysts in the mediastinum should be differentiated from other mediastinal cystic lesions such as benign congenital cysts(i.e.,bronchogenic,esophageal duplication,neuroenteric,pericardial,and thymic cysts),meningocele,mature cystic teratoma,and lymphangioma,as well as tumors with predominant necrotic or cystic components such as thymomas,germ cell tumors,and mediastinal carcinomas[10].
Treatment of mediastinal hydatid cyst is usually surgical and includes cystectomy with total or partial pericystectomy.The surgical approach depends of the cyst location and involvement of any associated surrounding structures[8].
PULMONARY ARTERY EMBOLIZATION OF HYDATID CYSTS
Pulmonary arterial embolization of hydatid cysts is a rare complication.Hepatic echinococci may rupture into the inferior vena cava,and daughter vesicles may cause embolisms in the pulmonary arteries spontaneously or during liver surgery[11,12].Right sided cardiac hydatid cysts can rupture directly into the pulmonary arteries[1,13].Pulmonary embolism with hydatid cysts can present acutely with coughing,hemoptysis,and chest pain[13,14]while some cases may present with subacute presentation and may develop pulmonary hypertension[14].
Diagnosis can be made on pulmonary CT angiography where non enhancing hydatid cysts cause widening of the lumen of pulmonary arteries.MRI displays the cystic nature of lesions better than CT.Cystic nature of the pulmonary artery filling defects as well as the lack of enhancement distinguish this entity from pulmonary thromboembolism and primary or secondary pulmonary arterial tumors (Figure 2).The presence of associated cardiac or hepatic hydatid cysts are supportive findings[12,15,16].Though surgical treatment may be recommended for low risk patients,some patients have been treated medically with variable outcomes (resolution,stability,or development of pulmonary hypertension)[15-17].
CARDIAC HYDATID CYST
Cardiac involvement by hydatid disease is rare with reported incidence of 0.23% out of 842 thoracic hydatid disease cases[18].The cardiac hydatid cysts can be asymptomatic or result in symptoms related to localization,size,and complications.Symptoms are non-specific and may include chest pain,dyspnea,and palpitations.Cardiac hydatid disease depending on location,can cause acute ischemic stroke,arrhythmias,pericardial reaction and pain,and pulmonary hypertension[19-22].
The left ventricle is the most frequently involved site (50%-60%),though the interventricular septum,right ventricle,pericardium (Figure 3),and atria can be involved[2,14].The cysts may be single or multiple,uniloculated or multiloculated,and thin or thick walled.Presences of calcification of the cyst wall,daughter cysts,and detached floating membranes are suggestive imaging features of hydatid cysts[23].The hydatid cysts can simulate solid mass on imaging and can be difficult to differentiate from heart tumors[24].Transthoracic echocardiography can suggest the initial diagnosis.CT and MRI can provide additional details of the location and extension of intra-cardiac hydatid cysts.CT best shows wall calcification.MRI delineates the exact anatomic location and signal characteristic of the internal and external structures(Figure 3).MRI can depict characteristic cystic appearance with low-signal and highsignal changes on T1W and T2W images respectively,and a hypo-intense peripheral ring on T2 weighted images which represents the pericyst[23,25].Intra-cardiac hydatid cyst may lead to severe symptoms or even sudden death due to complications,and treatment is usually surgical[14].
TRANS-DIAPHRAGMATIC EXTENSION
Hepatic hydatid disease with diaphragmatic involvement or extension into the thoracic cavity is reported in 0.16%-16% of cases[26].The lack of a peritoneal covering over the bare area of the liver makes it less resistant to cyst growth and more vulnerable for trans-diaphragmatic extension of hepatic hydatid cysts[1].The presence of air within hepatic or diaphragmatic hydatid cysts should raise the possibility of bronchial communication especially if associated with parenchymal findings in the adjacent lung.Associated pleural effusions,atelectasis,or pulmonary consolidation are suggestive findings of thoracic involvement[4,27].
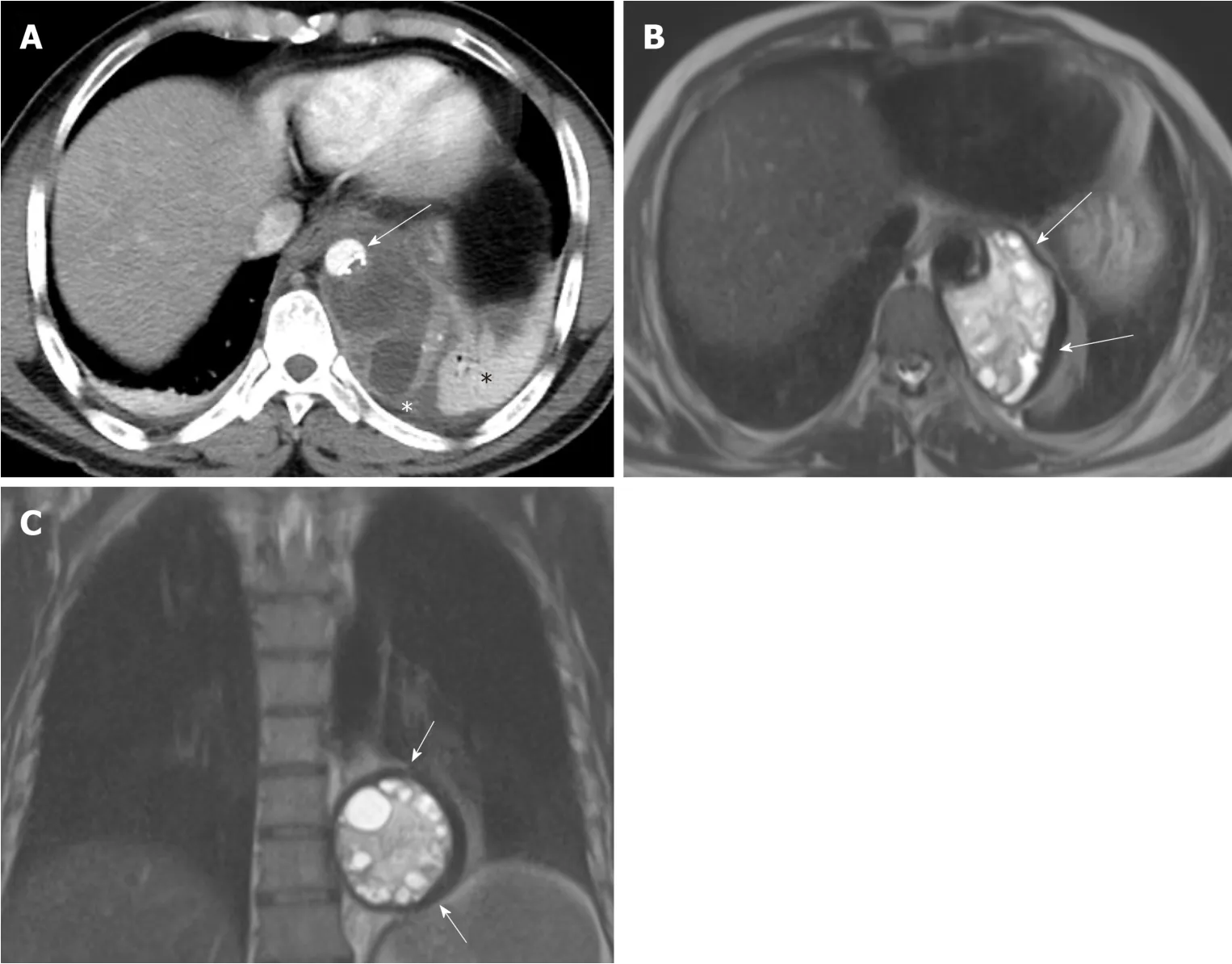
Figure1 A 48-year old male with mediastinal hydatid cyst presented with acute chest pain.
CT scan is valuable for detection and assessment of trans-diaphragmatic extension and extension of hepatic hydatid cysts into the thoracic cavity[26,28].Multi-planar imaging with sagittal and coronal reconstruction is very helpful in depicting transdiaphragmatic extension[1]and plays a role in accurate pre-surgical planning.There are proposed surgical grading of diaphragmatic or trans-diaphragmatic thoracic involvement in hepatic hydatid disease based on the degree of cyst evolution and involvement[26].Firm adherence between the diaphragm and the cyst surface without diaphragmatic perforation reflects grade 1.Diaphragmatic perforation with minimal invasion of the thoracic cavity is grade 2 (Figure 4).Grade 3 involves diaphragmatic perforation associated with either cyst growth inside the thoracic cavity or daughter vesicle formation.Involvement of the lung parenchyma either by communication between the cyst and the bronchial tree or compression of the lung parenchyma is considered grade 4[26].Formation of a broncho-biliary communication and fistula formation reflects grade 5 (Figure 5).Hydatid daughter cysts may be expectorated with sputum.Bile expectoration is a clinical warning sign of broncho-biliary fistula.Preoperative diagnosis of trans-thoracic extension with broncho-biliary fistula will potentially alter the surgical approach as a transthoracic approach is generally preferred in such cases.The surgical approach is complex and may include bronchial fistula ligation,lung segmentectomy or lobectomy,decortication,and diaphragmatic repair,as well as treatment of the underlying hepatic hydatid cysts.Placement of abdominal and thoracic drainage tubes may be necessitated[29,30].
INTRA-PLEURAL RUPTURE OF HYDATID CYST
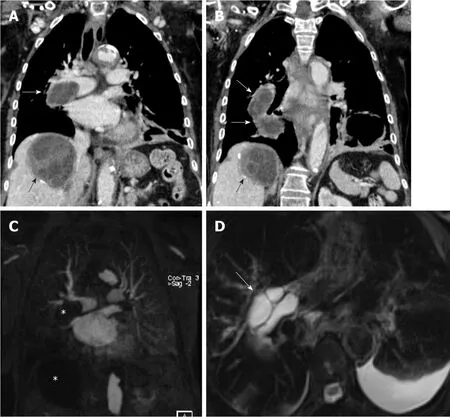
Figure2 An 82-year-old female with pulmonary artery hydatid cyst embolism presented with shortness of breath.
Lung tissue is mostly filled by air and allows hydatid cysts to increase in size particularly in children.Rupture is not an uncommon complication and more frequent in children (reported 26.7%)[31].Rupture can occur spontaneously when cyst increases to 7-10 cm in diameter or secondary to infection or trauma[32].Allergic reaction like urticaria or anaphylactic shock is rare complication of hydatid cyst rupture.Pulmonary hydatid cyst rupture can be contained or communicate with the bronchial tree or pleural cavity[31].Pleural necrosis secondary to pressure from peripherally located pulmonary cysts likely plays a role in the rupture of cysts into the pleural cavity[33].Chest pain,cough,shortness of breath,fever,sputum production and hemoptysis have been reported in patients with pleural hydatid disease with the latter two symptoms likely related to concomitant rupture to airways[34].
Rupture into pleural cavity can present with pleural effusion,pneumothorax or hydropneumothorax,empyema,pleural thickening,collapsed lung,and bronchopleural fistula[34,35].Ruptured hydatid cysts into the pleura can pose a diagnostic challenge for both radiologists and clinicians,especially if presenting acutely with no available prior images or evidence to suggest hepatic or lung hydatidosis.It can be misdiagnosed as empyema due to other infection such as tuberculosis[31,35].
Chest radiographs are usually the initial imaging exam and my show pleural effusion,pneumothorax,hydropneumothorax,and lung opacities.Lung opacities may represent atelectasis,pneumonia,or ruptured infected hydatid cysts.Chest CT exam are valuable in demonstrating pleural thickening and lung or pleural cysts,although ruptured cysts may collapse after spillage of cyst contents into the pleural cavity (Figure 6)[34,35].MRI may demonstrate detached membranes within the ruptured pleural cysts[36].The definitive diagnosis of intra-pleural rupture of hydatid cyst is sometimes made intra-operatively[35].
The primary treatment of pleural hydatid disease is surgical intervention.Cystostomy or cystectomy and capitonnage (obliterating the cavity by suturing the cavity walls) are commonly performed with or without pleural decortication[34,35].Bronchopleural fistula can be identified intraoperatively and subsequently repaired[35].Pulmonary resections (segmentectomy or lobectomy) is occasionally performed when the pulmonary parenchyma adjacent to the cyst is destroyed,unable to expand,or both[34].
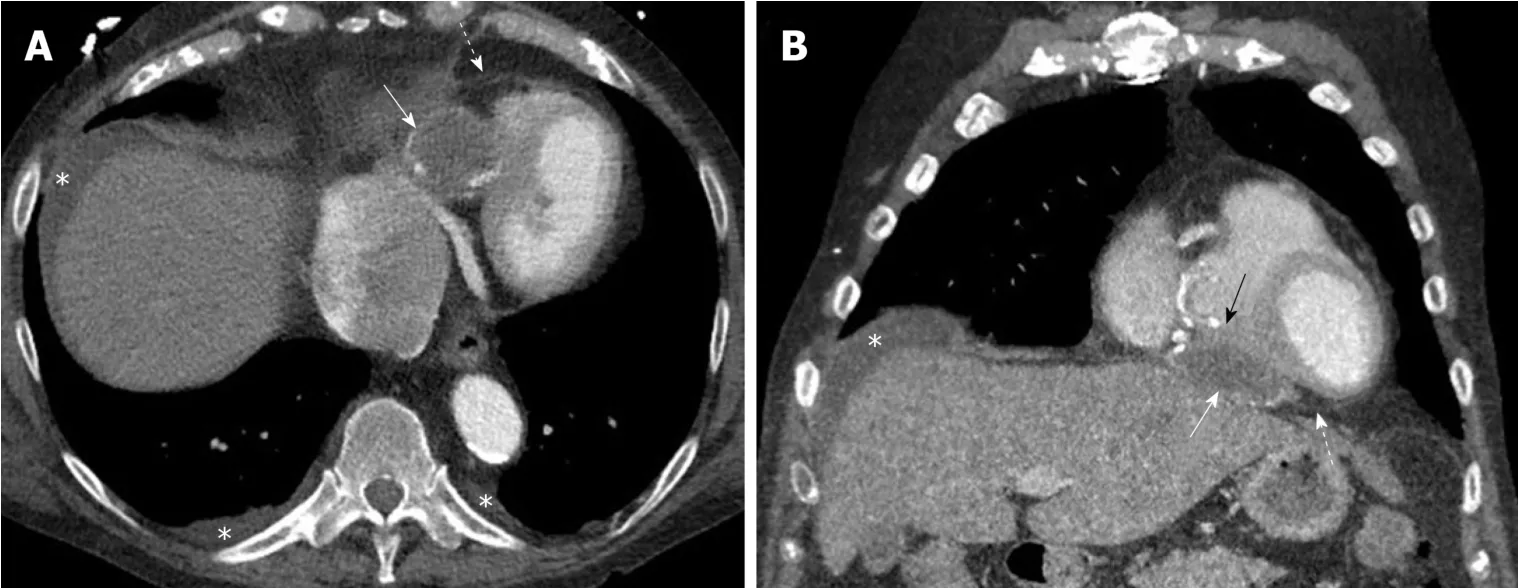
Figure3 Pericardial hydatid cyst.
CONCLUSION
The thoracic cavity can be affected by hydatid cysts in different ways.Although lungs are the most common affected site,hydatid cyst can be located in any part of the chest.Unusual location or complications can pose a diagnostic challenge and may influence treatment options.Radiologists and clinicians should consider hydatid disease when they encounter unusual cystic lesions in the chest especially in patients who lived in endemic areas or have evidence of hydatid disease elsewhere in the body.
Figure4 Hepatic hydatid cyst complicated by trans-diaphragmatic rupture in a 17 year old male patient.
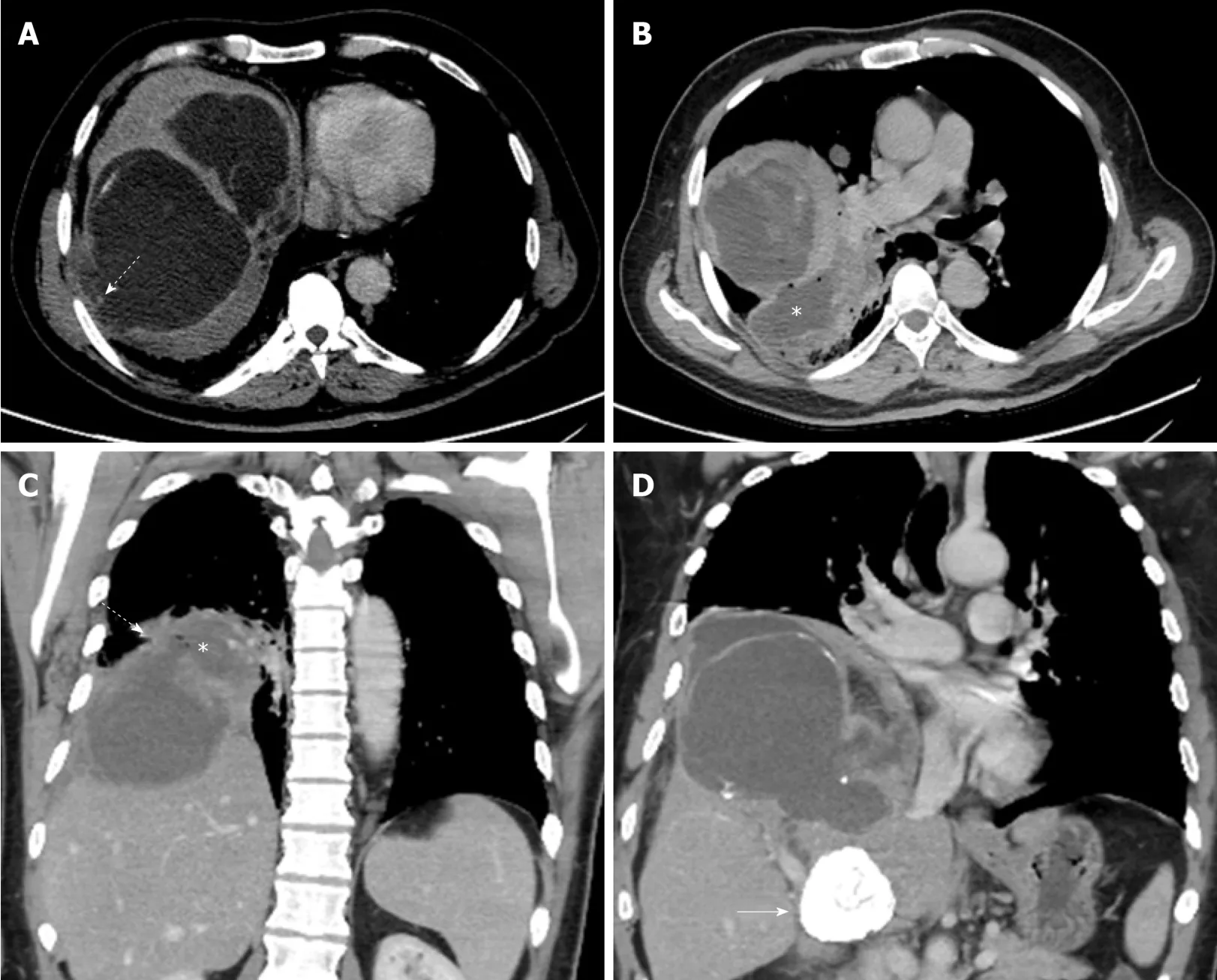
Figure5 A 42-year old male presented with liver hydatid cyst complicated by broncho-biliary fistula presented with coughing bile.
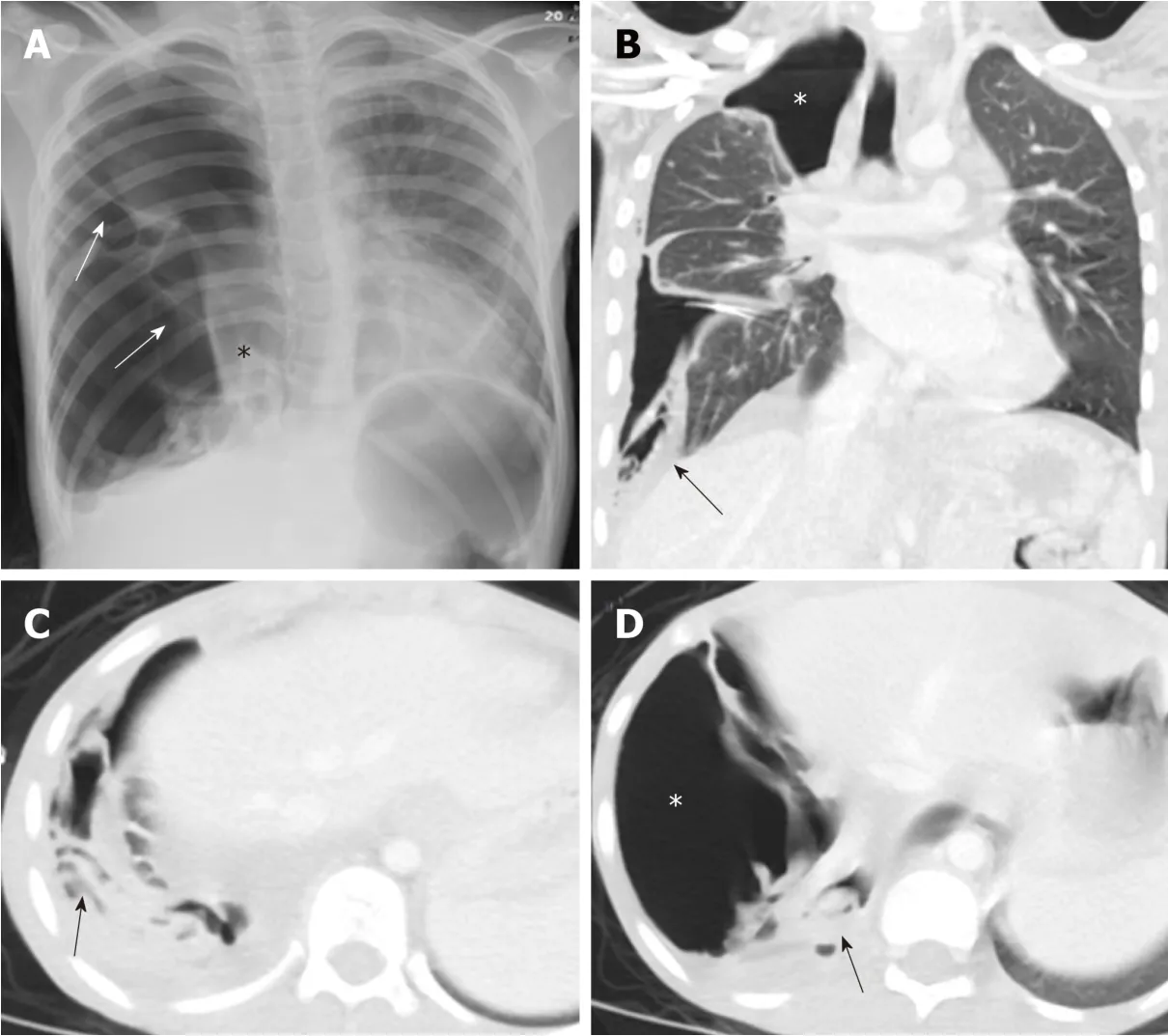
Figure6 A 10-year old female with spontaneous ruptured lung hydatid cyst presenting with pneumothorax and complicated by broncho-pleural fistula.
 World Journal of Clinical Cases2020年7期
World Journal of Clinical Cases2020年7期
- World Journal of Clinical Cases的其它文章
- CD56+ lymphoepithelioma-like carcinoma of the lung:A case report and literature review
- Systemic treatment for severe concentrated sulfuric acid burns in an adult male at high altitude:A case report
- Clinical effects of apatinib mesylate for treatment of multiple brain micrometastases:Two case reports
- Disseminated histoplasmosis in primary Sj?gren syndrome:A case report
- Severe venous thromboembolism in the puerperal period caused by thrombosis:A case report
- Multiple neurofibromas plus fibrosarcoma with familial NF1 pathogenicity:A case report