
Value of dynamic plasma cell-free DNA monitoring in septic shock syndrome:A case report
2020-04-22 07:13:16JingPingLiuShiChangZhangShiYangPan
World Journal of Clinical Cases 2020年1期
Jing-Ping Liu,Shi-Chang Zhang,Shi-Yang Pan
Jing-Ping Liu,Shi-Chang Zhang,Shi-Yang Pan,Department of Laboratory Medicine,the First Affiliated Hospital of Nanjing Medical University,Nanjing 210029,Jiangsu Province,China
Abstract
Key words: Septic shock;Acinetobacter baumannii;Cell-free DNA;Case report
INTRODUCTION
Septic shock is a subset of sepsis that often leads to metabolic disorders and multiorgan failure[1],resulting in hospital mortality rates greater than 40%[2].The mechanism of septic shock is complex and poorly understood.Septic shock is associated with cell necrosis and apoptosis.Plasma cell-free DNA (cfDNA) is free,extracellular DNA,which is mainly derived from apoptosisin vivoor from the degradation of genomic DNA from necrotic cells.The dynamic monitoring of plasma cfDNA levels can guide the treatment of septic shock.The aim of this study was to determine the efficacy of plasma cfDNA for monitoring septic shock.
CASE REPORT
Chief complaints
Abdominal pain,fever and chills.
History of present illness
A 29-year-old male patient presented at the Emergency Department of our hospital with complaints of abdominal pain,fever and chills on July 27,2017.The onset of disease was one day before presentation with bilateral swelling and pain in the gums.On the morning of admission,he had a sudden chill and a high fever with a peak of 39.8 °C.He suffered from intermittent right upper quadrant pain,accompanied by nausea and retching.
History of past illness
He had a history of a left lateral malleolus fracture subluxation 6 years ago and a history of allergies to penicillin and amoxicillin.He denied a history of smoking,drinking,hyperlipemia,and chronic diseases,such as coronary heart disease,hypertension and diabetes.
Physical examination upon admission
In the emergency room,he had a blood pressure of 80/50 mmHg and a heart rate of 130 beats/min.The right upper abdomen was prominent and tender at palpation without guarding and rebound tenderness.In addition,he had a positive Murphy's sign and liver percussion pain.
Laboratory testing
Laboratory tests showed leukocytopenia (2.38 × 109/L),a high percentage of neutrophils (83.2%),mild thrombocytopenia (68 × 109/L),abnormal blood coagulation function,a reduced international normalized ratio,hypokalemia,hyperbilirubinemia,elevated liver enzymes (both hepatocellular and cholestatic enzymes),an elevated procalcitonin (PCT) concentration (35.30 ng/mL),metabolic acidosis,and hyperlactatemia,suggesting progressive sepsis.On light microscopy,the peripheral blood smear showed a left shift of neutrophil nuclei,prominent toxic granulations and vacuolation in the neutrophil cytoplasm (Figure 1).Further laboratory results are shown in Table 1.Gram-negative bacilli were isolated from blood cultures.
Imaging examinations
A routine examination involving electrocardiography and a head CT scan showed no significant abnormalities.A multislice chest CT scan performed in the Department of Radiology showed little interstitial change in the lower lung.Scanning of the abdomen showed gallbladder wall edema with increased gallbladder density,swelling of the kidneys,and an enlarged pancreas.There was interlobular septal thickening on both sides and bilateral pleural effusion with lower lung insufficiencyof both longs,suggesting cardiac dysfunction with pulmonary edema (Figure 2).
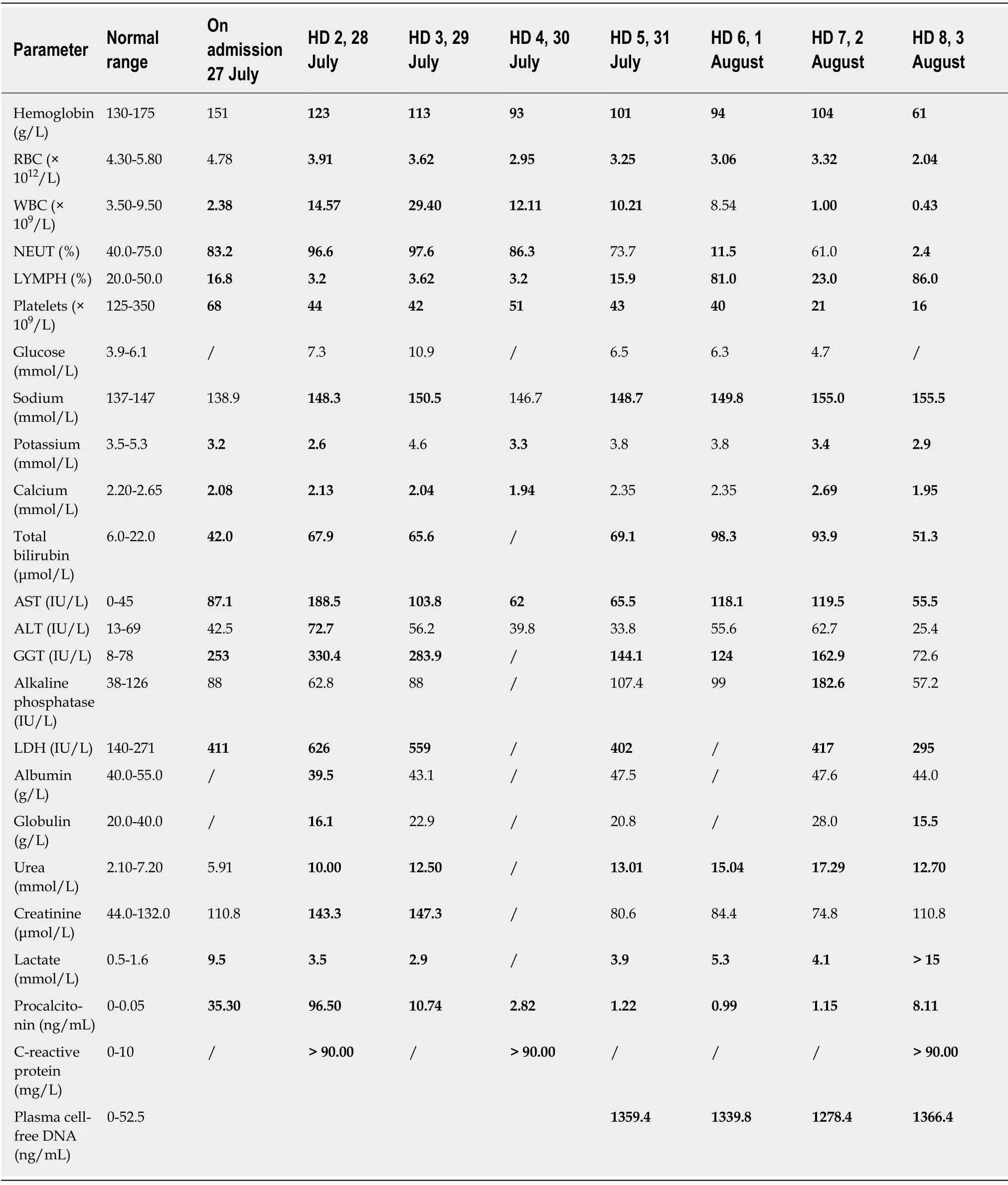
Table1 Laboratory data
FINAL DIAGNOSIS
Septic shock.
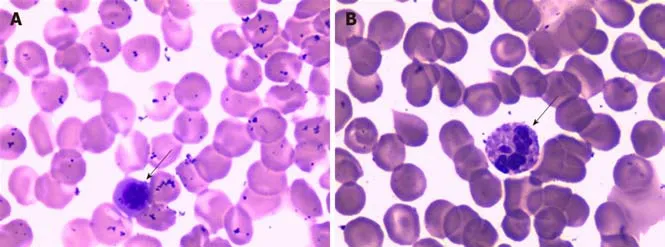
Figure1 The peripheral blood smear showed a left shift of neutrophil nuclei,prominent toxic granulations and vacuolation in the neutrophil cytoplasm(see arrows) (Wright stain ×1000).
TREATMENT
During the patient's stay in the Department of Infectious Diseases,he received catecholaminergic therapy,fluid replacement,plasma transfusion and antibiotics(imipenem).The general condition of the patient rapidly worsened.Seven hours after presentation at the hospital,a decision was made to admit him to the intensive care unit (ICU).Treatment consisting of intravenous administration of broad-spectrum antibiotic therapy (imipenem,ganciclovir,moxifloxacin and phosphate oseltamivir),plasma and cryoprecipitate was initiated.Despite this therapy,acute respiratory distress syndrome occurred within the next few hours.Intensive treatment,which included mechanical ventilation,the continuous infusion of catecholamines and pharmacological therapy,was started.The typical clinical signs of septic shock,such as facial flushing,mild cyanosis of the lips,and conjunctival and pharynx congestion,were observed.Gram-negative bacilli were isolated from blood cultures.The patient then received tigecycline combined with imipenem/cilastatin to treat the infection.The inflammation markers remained high [C-reactive protein (CRP) and PCT].
On the 3rdday,due to unresponsiveness of the patient to conventional intensive therapy and the presence of a life-threatening condition,continuous renal replacement and extracorporeal membrane oxygenation (ECMO) were performed as rescue therapies.A significant improvement was observed in terms of the laboratory findings.Marked decreases in white blood cells (WBCs) (29.40 × 109/L to 8.54 × 109/L)and PCT (96.50 ng/mL to 0.99 ng/mL) and a reduction in the catecholamine dosage were achieved three days later.
However,plasma cfDNA levels were constantly high,peaking at 1366.40 ng/mL(Figure 3).cfDNA levels were measured by a duplex real-time PCR assay with an internal control,which was developed as a novel method for the accurate quantification of plasma cfDNA in our previous study.Within the 95% confidence interval,the normal reference intervals were 0-52.5 ng/mL for males and 0-45.8 ng/mL for females[3].
On the 7thday,the patient developed facial flushing,with increased body temperature (39.6 °C) and heart rate (140-150 beats/min),and decreased WBCs (1.00 ×109/L) and central venous pressure (9-10 mmHg).To maintain his blood pressure,he received a fluid infusion and catecholaminergic therapy.Peripheral blood and bone marrow examinations showed granulocyte maturation disorders,which may have been caused by infection (Figure 4).Therefore,he received treatment with leukocyte drugs,such as granulocyte-colony stimulating factor.At night,his urine volume began to decrease,the urine color was deeper and the lactate level gradually increased to greater than 15 mmol/L.Metabolic acidosis,hypernatremia and hypokalemia followed.Then,cyanosis,a deep coma,bilateral scattered pupils,and lungs full of coarse wet rales were observed.Treatment with rapid liquid infusion,high dose norepinephrine and pituitary vasopressin and ECMO were ineffective.His arterial blood pressure continued to decline.
OUTCOME AND FOLLOW-UP
The patient died of septic shock at 00:10 on August 4,2017.

Figure2 Computed tomography scan.
DISCUSSION
We report a case of septic shock syndrome caused byAcinetobacter baumanniiandPantoea,which was characterized by high fever,chills and abdominal pain.The patient had fever,diarrhea,toothache and a history of self-administered intravenous drugs.The onset of septic shock was acute and progressed rapidly into a state of shock.His symptoms were significantly more severe than those of the bacteremia caused by the hospital-wide panresistantAcinetobacter baumannii.This effect was possibly associated with the endotoxemia of sensitive bacteria,which were lysed by antibiotics.
Any type of bacteria can cause septic shock,but this condition is mainly caused by gram-negative bacilli[4].Acinetobacter baumannii,a gram-negative coccobacillus,can act as an opportunistic pathogen in humans,affecting people with a range of different diseases.Acinetobacter baumanniiis becoming an increasingly important hospitalderived infection that can cause septic shock.Bacterial septic shock is frequently caused by the overproduction of inflammatory mediators as a result of the immune recognition of bacteria or bacterial products[5].The administration of effective antibacterial drugs as early as possible to control primary underlying diseases and improve shock by correcting metabolic acidosis and supplementing the blood volume are critical to treatment.In addition,a timely and effective evaluation of the patient's therapeutic response is also critical.Conventional microbiological cultures for diagnosing septic shock are usually time consuming,do not reflect the systemic inflammatory response or the onset of organ dysfunction and may sometimes be misleading,generating false-positive or false-negative results.
Some traditional indicators,such as body temperature,WBCs,and blood lactate levels,can reflect the condition and efficacy of treatment,but these indicators are not very reliable.The clinical manifestations of septic shock are highly variable[4].In this case,the WBC count was significantly reduced on admission and in the late stage of septic shock.This result may have been associated with the increased adhesion of leukocytes in severe infections.Thus,WBCs may have adhered to the vascular endothelium and may not have entered the circulation pool.
In septic shock,mitochondrial oxygen delivery is reduced due to hypoxia and hypoperfusion,and lactate synthesis increases,resulting in hyperlactatemia.Lactate plays an important role in assessing the severity of septic shock and objectively predicting the prognosis.In the 2017 Surviving Sepsis Campaign international guidelines and 2016 Sepsis-3 definitions,lactate levels were used to define patients with septic shock[2,6].A high level of blood lactate is associated with the mortality and prognosis of patients with septic shock,but it is not specific.Trauma,seizures,cardiac arrest and other conditions can also lead to increased levels of lactate.Normal lactate levels are not always a marker for good prognosis in septic shock[7].
Acute-phase proteins,such as CRP or PCT,can also be used as biomarkers of the severity and prognosis of patients with septic shock.CRP,a liver-derived protein,is an attractive marker for diagnosing septic shock due to its easy access and low cost.CRP is well correlated with the severity of infection.The CRP level of the patient in our case remained high throughout the entire course.However,the specificity of CRP is limited[8].A previous study demonstrated that CRP cannot reflect sepsis severity[9]because it fails to distinguish infectious from noninfectious inflammatory responses[10].Therefore,CRP could only be considered an inflammatory biomarker.
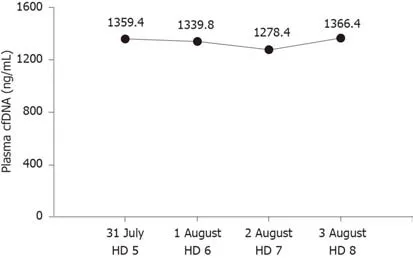
Figure3 Plasma cell-free DNA concentrations.
PCT,the precursor of the hormone calcitonin,is significantly elevated in septic shock patients;PCT has high specificity and is positively correlated with disease severity and mortality[11].Activation of the lymphatic system can produce large amounts of PCT during infections or when the body is otherwise stimulated.The halflife of PCT is 25-30 h[12],and PCT is increased earlier than CRP and other inflammatory factors in patients with bacterial infections.Septic shock patients can have a rapid decline in PCT in response to effective treatment with antibacterial agents,suggesting that PCT has important clinical implications for monitoring disease progression.In this case,PCT was significantly reduced starting on day 3,which made physicians mistakenly think that the patient was getting better.However,the patient's condition worsened.We hypothesized that the decline in PCT may have been due to organ failure,which was caused by septic shock.
In addition to these classic biomarkers,cfDNA,which was first described in 1948[13],has the potential to be a useful marker in septic shock.CfDNA is released into the circulation through cell lysis,necrosis,apoptosis and active DNA release,resulting in higher concentrations of cfDNA in patients with microbial infections,trauma,cancer and other clinical conditions[14].Although elevated levels of cfDNA are not specific to a single disease,elevated cfDNA has been shown to be an extremely sensitive and promising prognostic marker in septic shock[15].This observation may be associated with the shorter half-life of cfDNA[16,17]than that of PCT and CRP.According to Ahmed,cfDNA is a good prognostic predictor for patients in the ICU and,to a lesser extent,is a good marker of septic shock[18].However,the inevitable loss of cfDNA during extraction has become a considerable detriment,hindering its clinical applications.We previously developed a duplex real-time PCR assay with an internal control as a novel method for the accurate quantification of plasma cfDNA,which can eliminate preanalytical errors and increase the precision and accuracy[3].Our previous studies showed the clinical value of plasma cfDNA levels,as measured by this novel method,in several conditions.CfDNA levels can be useful not only in evaluating chemotherapy effects and guiding treatment in advanced lung cancer patients,but also in assessing liver injury in hepatitis B patients[19-21].In this case,cfDNA remained high until the patient died,suggesting that cfDNA could be used to monitor disease progression more effectively than PCT.Although the death of patients with septic shock in our hospital is rare,the conclusion of our study is based on only one case.In future,we will conduct large-scale clinical trials to confirm the value of cfDNA in septic shock.
CONCLUSION
Using a single biomarker for the diagnosis or prognosis of septic shock is not practical.Therefore,cfDNA could be a promising marker that complements PCT,CRP,lactate and other inflammatory factors to better manage patients with septic shock.
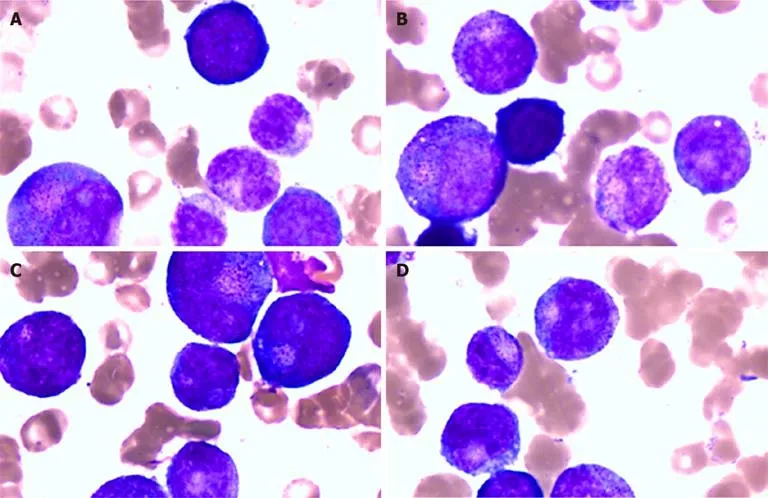
Figure4 The bone marrow smear showed granulocyte maturation disorders.
 World Journal of Clinical Cases2020年1期
World Journal of Clinical Cases2020年1期
- World Journal of Clinical Cases的其它文章
- Cluster headache as a manifestation of a stroke-like episode in a carrier of the MT-ND3 variant m.10158T>C
- Primary intestinal extranodal natural killer/T-cell lymphoma,nasal type:A case report
- Six families with balanced chromosome translocation associated with reproductive risks in Hainan Province:Case reports and review of the literature
- Clinical characteristics on manifestation and gene mutation of a transient neonatal cyanosis:A case report
- Sarcomatoid intrahepatic cholangiocarcinoma mimicking liver abscess:A case report
- Unusual presentation of bladder neuroblastoma in a child:A case report