
Inflammatory pseudotumor-like follicular dendritic cell sarcoma: A brief report of two cases
2019-12-14 07:12:16BiXiZhangZhiHongChenYuLiuYuanJunZengYanChunLi
Bi-Xi Zhang,Zhi-Hong Chen,Yu Liu,Yuan-Jun Zeng,Yan-Chun Li
Abstract
Key words: Inflammatory pseudotumor-like follicular dendritic cell sarcoma; Epstein-Barr virus; Liver; Spleen; Case report
INTRODUCTION
Follicular dendritic cell (FDC) sarcoma/tumor is a rare malignant tumor of follicular dendritic cells,which are mesenchymal cells in the lymphoid follicles with antigen presenting ability.It is considered a low-grade sarcoma that can involve lymph nodes or extranodal sites[1-5].In 1996,Sheket al[6]reported the first case of primary FDC sarcoma in the liver.The histology was similar to an inflammatory pseudotumor and it was related to Epstein-Barr virus (EBV)-related clonal proliferation[6].Inflammatory pseudotumor-like FDC sarcoma was first described as a distinctive variant of FDC sarcoma and associated with EBV in 2001[7].There have been 48 previously reported cases of inflammatory pseudotumor-like FDC sarcoma,which occurs almost exclusively in the liver and spleen (Table 1).Ancillary tests,including detection of immunohistochemical markers of FDC such as CD21,CD23,or CD35 and EBV probebasedin situhybridization,are required for this diagnosis.Here we report two cases of inflammatory pseudotumor-like FDC sarcoma in the liver that were treated by 3D laparoscopic right hepatectomy and open right hepatectomy separately.
CASE PRESENTATION
Chief complaints
Case 1:A 31-year-old woman was admitted to hospital for evaluation of a four-week history of anorexia.
Case 2:A 48-year-old man stumbled across a liver mass through a routine ultrasound examination.
History of present illness
Unremarkable.
History of past illness
Case 1:Her past medical history was chronic hepatitis B for more than 10 years without antiviral treatment.
Case 2:Unremarkable.
Personal and family history
Unremarkable.
Physical examination upon admission
Case 1:Physical examination revealed mild tenderness to palpation in the right upper quadrant.
Case 2:Physical examination was unremarkable.
Laboratory examinations
Case 1:Laboratory tests showed seropositivity for HBsAg,HBeAb,and HBcAb.Furthermore,serum level of hepatitis B virus-DNA was lower than detection limit.
Case 2:Laboratory tests were unremarkable.
Imaging examinations
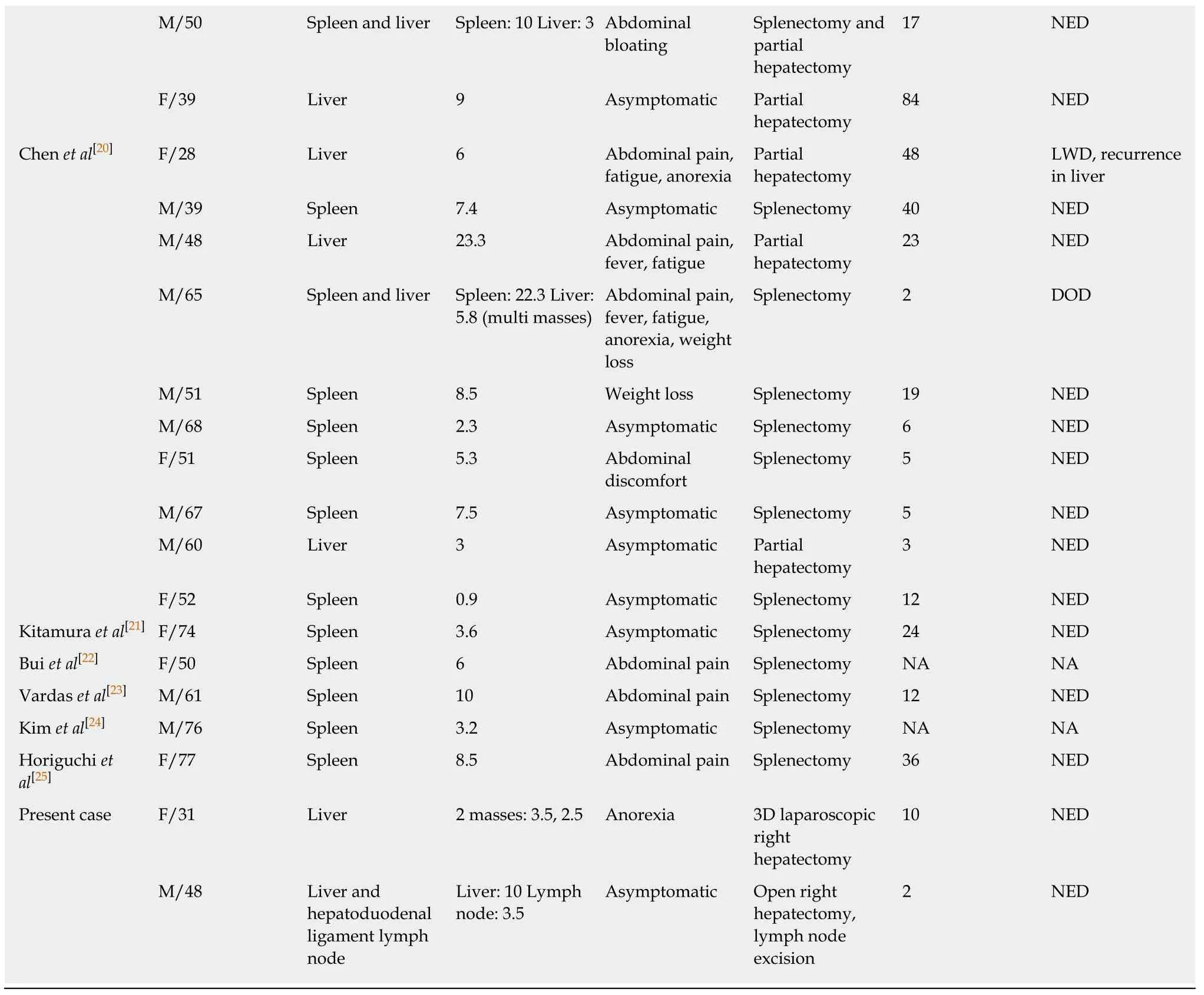
Case 1:Abdominal magnetic resonance imaging revealed two well-circumscribed masses in the right posterior lobe of the liver (Figure 1).
Case 2:An abdominal computed tomography examination revealed an ill-defined 10 cm mass in the right lobe of the liver accompanied with enlargement of hepatic portal lymph nodes (Figure 2).
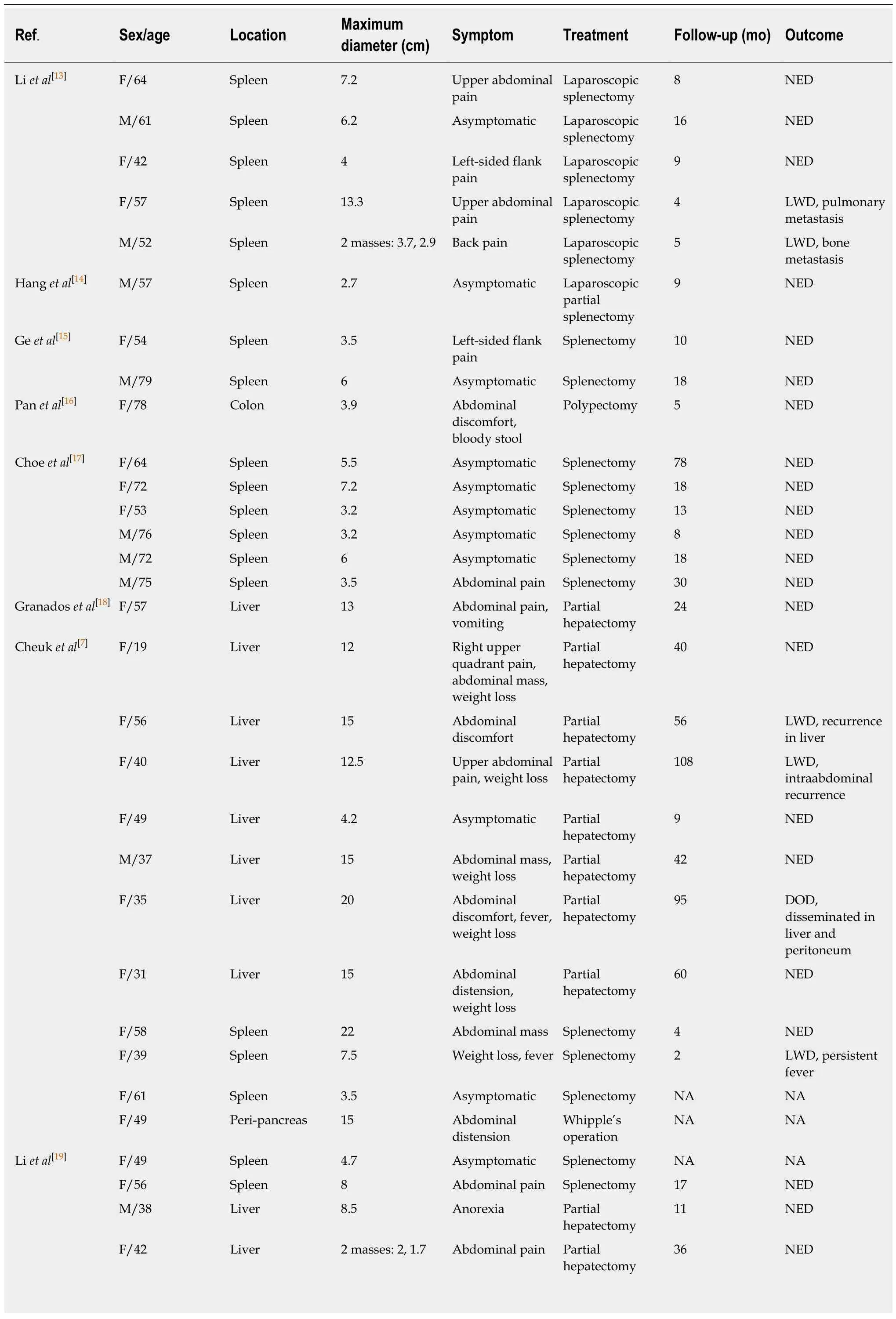
Table 1 Review of inflammatory pseudotumor-like follicular dendritic cell tumor/sarcoma
M: Male; F: Female; NED: No evidence of disease; DOD: Dead of disease; LWD: Live with disease; NA: Not available.
FINAL DIAGNOSIS
Case 1
EBV-positive inflammatory pseudotumor-like FDC sarcoma in the liver (Figure 3).
Case 2
EBV-positive inflammatory pseudotumor-like FDC sarcoma in the liver with hepatoduodenal ligament lymph node involvement (Figure 4).
TREATMENT
Case 1
3D laparoscopic right hepatectomy.
Case 2
Open right hepatectomy combined with regional lymphadenectomy.
OUTCOME AND FOLLOW-UP
Case 1
Follow-up for 10 mo showed no recurrence or metastasis.
Case 2
Follow-up for 2 mo showed no recurrence or metastasis.
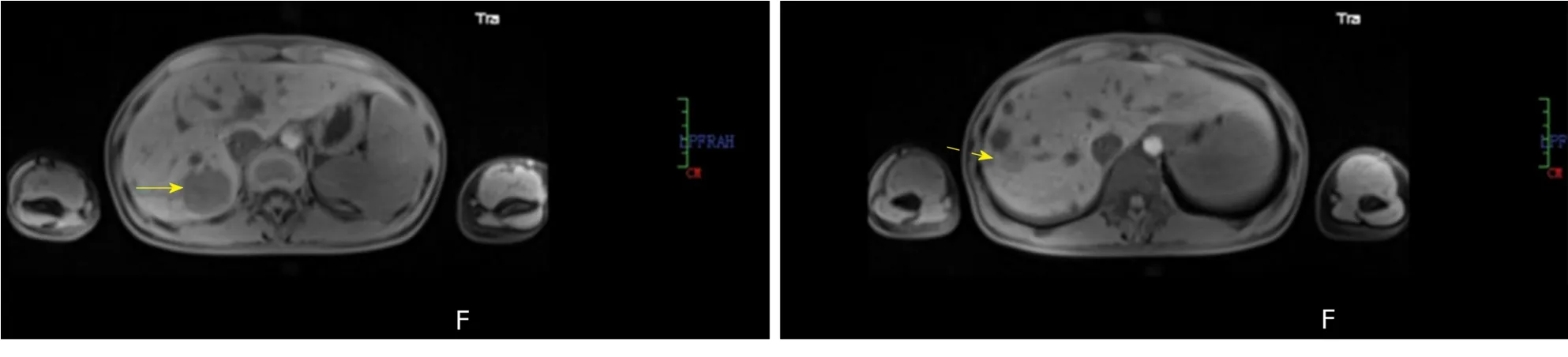
Figure 1 Magnetic resonance imaging.
DISCUSSION
FDC sarcoma is a neoplastic proliferation of spindled to ovoid cells exhibiting morphological and immunophenotypic features of FDCs.Histologically,FDC sarcomas are classified into two types: (A) Conventional FDC sarcoma consisting of spindled to ovoid cells forming fascicles,storiform arrays,whorls,diffuse sheets,or vague nodules with an array of small lymphocytes; and (B) Inflammatory pseudotumor-like FDC sarcoma composed of neoplastic spindled cells that are dispersed within a prominent lymphoplasmacytic infiltrate[3].To date,48 cases of inflammatory pseudotumor-like FDC sarcoma have been reported in the Englishlanguage literature,located in the liver (16/48),spleen (32/48),colon (1/48),and peripancreas (1/48),respectively.These cases included 19 males and 29 females(male/female ratio of 1: 1.5),with a mean age of 55 years (range,19-79 years).Clinical manifestations include abdominal pain,abdominal bloating,abdominal mass,weight loss,fever,fatigue,and anorexia,but most cases are asymptomatic (Table 1).
The origin of FDC sarcoma remains controversial.Phenotypic marker studies andin vitroexperiments with fibroblast-like cell lines have developed FDCs from fibroblast-like cells[8].The neoplastic cells are often positive for FDC markers,such as CD21,CD23,and CD35,with the staining ranging from extensive to very local.FDCs appear to be closely related to bone marrow stromal progenitors,with several myofibroblast features[9].Two studies examining the transcriptional profile of FDC sarcoma have revealed: (A) A peculiar immunological microenvironment enriched in follicular helper T cells and Treg populations,with special relevance to the inhibitory immune receptor programmed cell death protein 1 and its ligands,programmed cell death-Ligand 1 and programmed cell death-Ligand 2; and (B) The highly specific expression of the genes encoding for FDC secreted peptide and serglycin[10-11].
Conventional FDC sarcomas are negative for EBV,whereas the inflammatory pseudotumor-like variant consistently shows EBV in the neoplastic cells[7].EBVencoded small RNA was detected in both of the present cases byin situhybridization.EBV-encoded latent membrane protein 1,which has been found to have an oncogenic role,has been identified in 74% (26/35) cases of inflammatory pseudotumor-like FDC sarcomas by immunohistochemical staining[7,17,19-21,25].Recently,Takeuchiet al[12]reported increased numbers of EBV-infected cells in IgG4-related lymphadenopathy,compared with other reactive lymphadenopathy or extranodal IgG4-related disease,which suggests that there may be a relationship between IgG4-related disease and EBV[12].Interestingly,Choeet al[17]reported that significant numbers of IgG4-positive plasma cells were found in six cases of EBV-positive inflammatory pseudotumor-like FDC sarcoma of the spleen,suggesting that EBV plays a critical role in inflammatory pseudotumor-like FDC sarcoma and IgG4-related sclerosing disease[17].Generally,the pathogenic mechanism of EBV in inflammatory pseudotumor-like FDC sarcoma remains unclear and further investigation is required.
FDC sarcoma is usually treated by complete surgical excision,with or without adjuvant radiotherapy or chemotherapy.A pooled analysis of the literature revealed local recurrence and distant metastasis rates of 28% and 27%,respectively.Large tumor size (≥ 6 cm),coagulative necrosis,high mitotic count (≥ 5 mitoses per 10 highpower fields),and significant cytological atypia are associated with a worse prognosis[2,5].Regarding the prognosis of patients with inflammatory pseudotumorlike FDC sarcoma,based on the literature reports of inflammatory pseudotumor-like FDC sarcoma with a median follow-up period of 17 mo,35 patients had no evidence of disease.Five patients exhibited distant metastasis and two had local recurrence,with traits similar to large tumors and multiple masses.One of the current cases presented with liver and hepatoduodenal ligament lymph node involvement,suggesting that inflammatory pseudotumor-like FDC sarcoma presents an increased risk of lymph node metastasis.Complete surgical excision combined with regional lymphadenectomy may be effective in reducing the postoperative recurrence and metastasis and improving the long-term survival rates.
Figure 2 Abdominal computed tomography examination.
CONCLUSION
In conclusion,there is little specificity in the clinical manifestations of inflammatory pseudotumor-like FDC sarcoma.EBV probe-basedin situhybridization and detection of immunohistochemical markers of FDC play important roles in the diagnosis and differential diagnosis of inflammatory pseudotumor-like FDC sarcoma.Radical surgical resection is the main therapeutic intervention for inflammatory pseudotumor-like FDC sarcoma,especially for cases with lymph node involvement,and patients require long-term post-surgical follow-up.
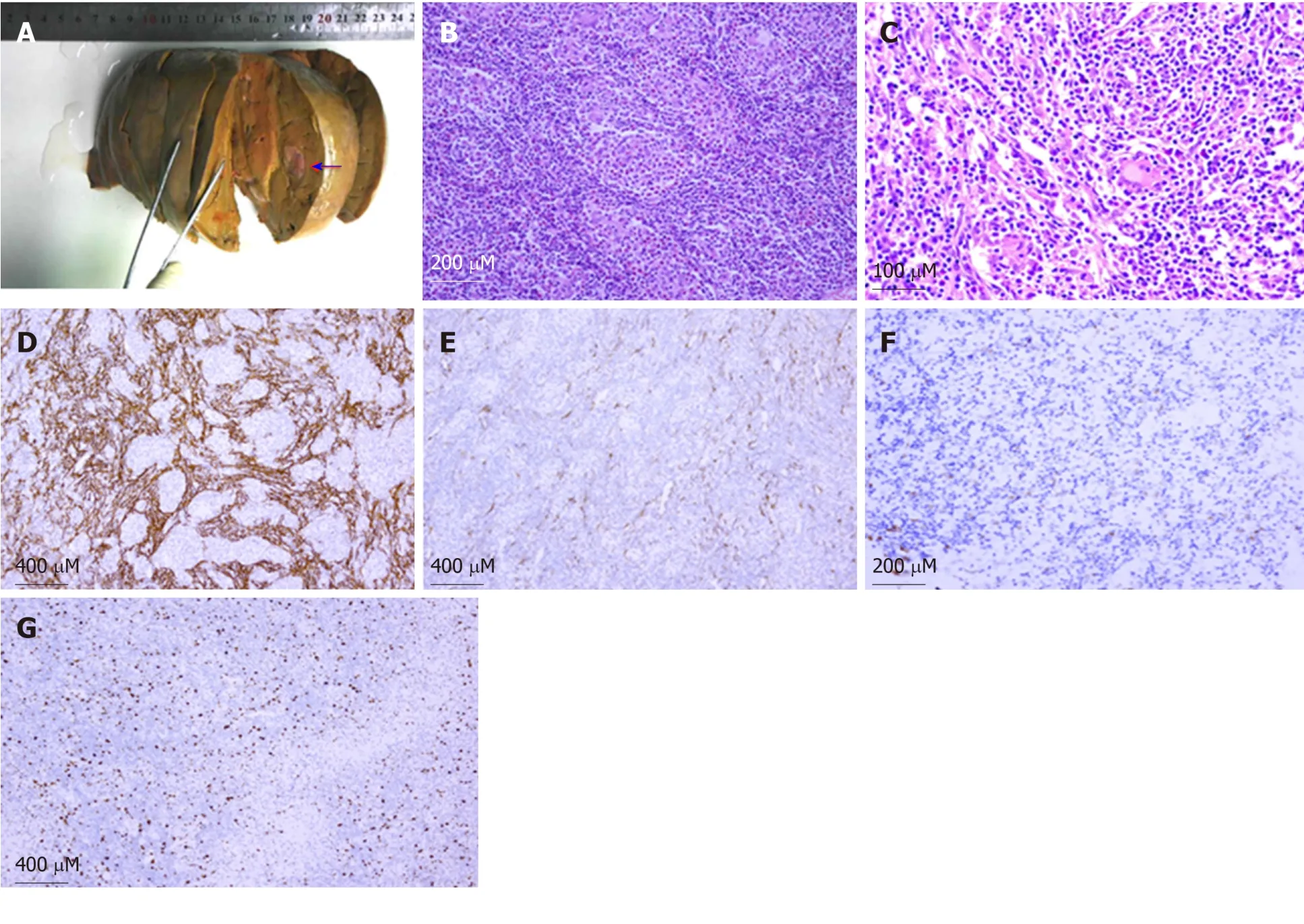
Figure 3 Epstein-Barr virus-positive inflammatory pseudotumor-like follicular dendritic cell sarcoma in the liver.
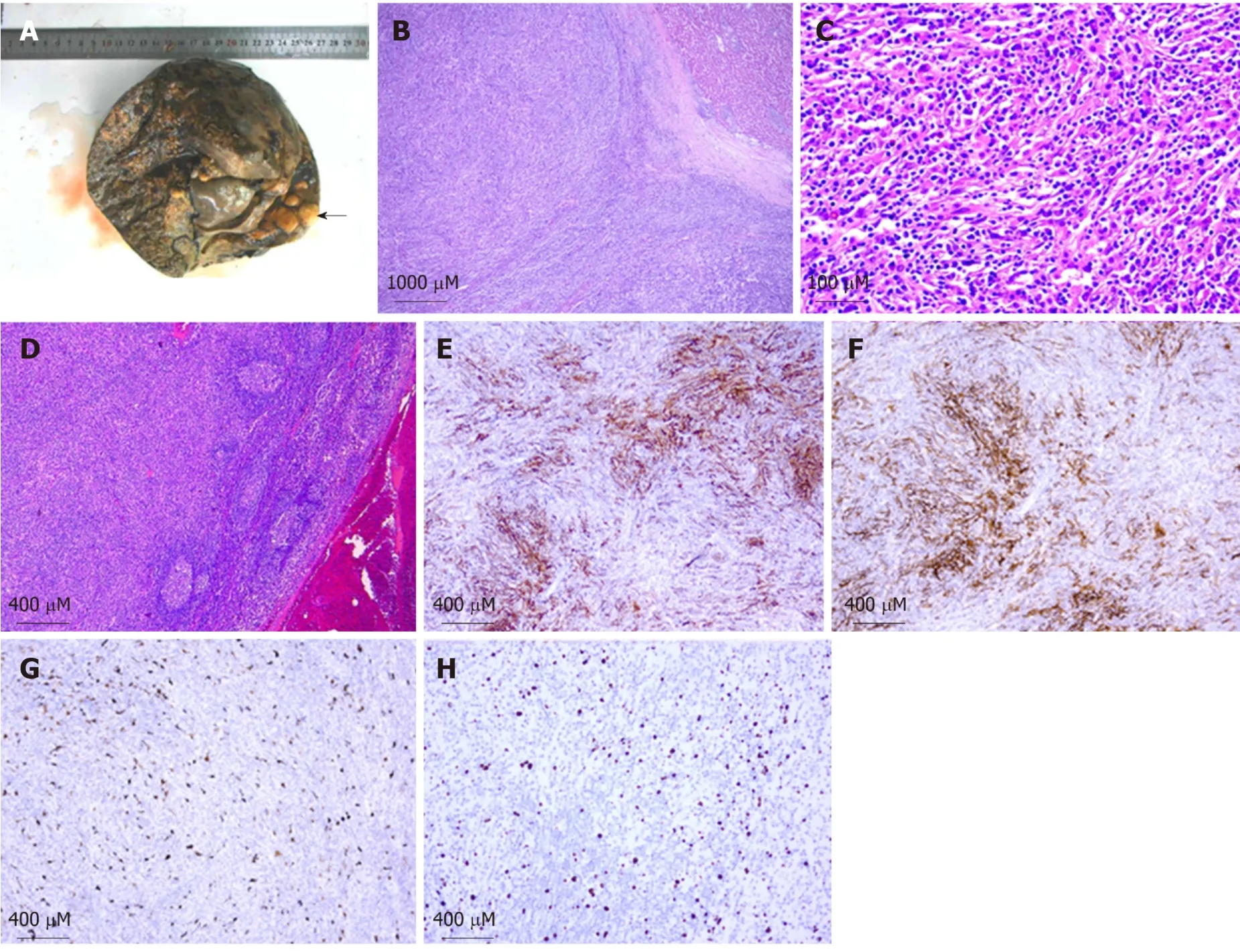
Figure 4 Epstein-Barr virus positive inflammatory pseudotumor-like follicular dendritic cell sarcoma in the liver with hepatoduodenal ligament lymph node involvement.
 World Journal of Gastrointestinal Oncology2019年12期
World Journal of Gastrointestinal Oncology2019年12期
- World Journal of Gastrointestinal Oncology的其它文章
- Current status of the genetic susceptibility in attenuated adenomatous polyposis
- Deep learning with convolutional neural networks for identification of liver masses and hepatocellular carcinoma: A systematic review
- Analysis of factors potentially predicting prognosis of colorectal cancer
- Multi-parameter ultrasound based on the logistic regression model in the differential diagnosis of hepatocellular adenoma and focal nodular hyperplasia
- Impact of regular enteral feeding via jejunostomy during neo-adjuvant chemotherapy on body composition in patients with oesophageal cancer
- Difference in failure patterns of pT3-4N0-3M0 esophageal cancer treated by surgery vs surgery plus radiotherapy