
Leukocytoclastic vasculitis caused by hepatitis C virus in a liver transplant recipient: A case report
2019-05-17 02:29:28GustavodeSousaArantesFerreiraAndreLuisCondeWatanabeNataliadeCarvalhoTrevizoliFernandoMarcusFelippeJorgeLuizGustavoGuedesDiazMillaCarolinaCostaLafetaAraujoGabrieladeCamposAraujoAmandadeCastroMachado
World Journal of Hepatology 2019年4期
Gustavo de Sousa Arantes Ferreira, Andre Luis Conde Watanabe, Natalia de Carvalho Trevizoli,Fernando Marcus Felippe Jorge, Luiz Gustavo Guedes Diaz, Milla Carolina Costa Lafeta Araujo,Gabriela de Campos Araujo, Amanda de Castro Machado
Abstract
Key words: Hepatitis C; Liver transplantation; Leukocytoclastic vasculitis;Immunosuppression; Direct-acting antivirals; Case report
INTRODUCTION
Hepatitis C is a chronic liver disease caused by infection with the hepatitis C virus(HCV). According to the Global Hepatitis Report 2017, around 71 million people worldwide carry the HCV infection[1]. As this disease leads to liver fibrosis, cirrhosis and/or hepatocellular carcinoma (HCC), it is currently one of the most common causes for liver transplant worldwide, being the main cause of liver transplant in the United States and Europe[1,2].
Recurrence of HCV after liver transplantation is a common event, occurring in practically all patients who were not successfully treated prior to the surgical procedure[3,4]. Diagnosis is made by either liver biopsy or detection of HCV in the bloodviapolymerase chain reaction (PCR). While the timing to recurrence varies among individuals, the manifestations of the HCV infection after the transplant are typically more aggressive than with the original infection due to the posttransplantation immunosuppressive drug regimen[3-5].
Infection by HCV is not limited to the liver and extrahepatic manifestations can include mixed cryoglobulinemia, insulin resistance, and depression, as well as cardiovascular, renal and dermatological diseases[6]. Among the dermatological manifestations in particular, the more common are late cutaneous porphyria,cryoglobulinemic vasculitis, lichen planus, psoriasis, erythema multiforme, erythema nodosum, and necrolytic acral erythema[7].
春深花正艷(曹香玲) ...................................................................................................................................5-59
Leukocytoclastic vasculitis is an inflammatory syndrome that affects small-sized vessels, and the most prominent histological features are leukocytoclasia (neutrophil fragmentation) and fibrinoid necrosis[8]. It can develop secondary to drugs, infection,collagen disease, or cancer. The most common clinical presentation is a palpable purpura in the lower extremities[8,9], although cutaneous manifestations can also include petechiae, nodules or ulcers. Ultimately, skin biopsy is necessary for diagnostic confirmation[10,11].
Cases of leukocytoclastic vasculitis in organ transplant patients have been reported,but none of those previous cases have cited HCV recurrence as the underlying cause.
CASE PRESENTATION
A 61-year-old female with cirrhosis due to chronic HCV infection, cirrhosis and HCC,underwent liver transplant.
At the time of transplantation, the patient's model for end-stage liver disease(MELD) score was 6 and Child-Pugh classification was grade A (5 points). Three years prior to the procedure, the patient had undergone treatment with pegylatedinterferon and ribavirin for 1 year, achieving no sustained virologic response. The interferon had been discontinued, but the ribavirin had been continued as monotherapy for another 6 mo. At the end of treatment, the patient's HCV RNA load was undetectable by PCR and the treatment had been considered effective. A screening ultrasound of the patient's abdomen, however, showed a suspicious nodule in the liver. Computerized tomography (CT) scan revealed a hypervascular lesion with rapid washout, suggestive of HCC, measuring 38 mm × 36 mm in the liver segment IVA. This lesion had close contact with the middle hepatic vein and retrohepatic inferior vena cava, and was deemed to be unresectable.
The patient was submitted to orthotopic liver transplantation with a graft from a cadaveric donor (37-year-old male). Total ischemia time was 4 h and 41 min, with no intraoperative complications and no need for blood product transfusions. She was discharged from the intensive care unit 2 d after the procedure and from the hospital 8 d after the transplant.
Chief complaints
At 5 mo after the surgery, the patient returned to the emergency room complaining of pain, swelling and redness on both lower extremities, associated with fever, diarrhea and vomiting.
History of present illness
The patient reported that the skin lesions appeared 17 d before she presented to the emergency room, and they had gradually increased in extension during that period.She had already presented to another institution and given treatment for a presumptive diagnosis of cellulitis, consisting of cephalexin and then amoxicillin-clavulanate for 1 wk. The treatment induced no improvement and her clinical condition worsened, as she developed diarrhea, vomiting and loss of appetite.
History of past illness
The patient had no previous history of skin disease and no significant comorbidities,other than HCV infection and the recent transplant. She reported contact with ticks 1 wk before the lesions appeared.
Physical examination
A painful palpable purpura was observed on both lower extremities, affecting the lateral and posterior aspect of the lower legs (Figure 1). The patient was admitted to the hospital for investigation, and intravenous cefepime was started. In addition, a short course of doxycyclin was administered, to address the history of contact with ticks.
Laboratory testing
Blood and urine cultures were obtained, yielding negative results. Biochemical tests showed normal leukocyte and platelet counts, and levels of blood urea nitrogen,creatinine, aspartate aminotransferase and alanine aminotransferase within the normal range (NR). Remarkable findings were anemia (hemoglobin concentration of 8.6 g/dL) and hypocomplementemia [C3 52 mg/dL (NR: 90-170), C4 < 2 mg/dL (NR:12-36), total complement CH50 < 60 U/CAE (NR: 60-265)]. Tests for anti-RO, anti-LA,anti-DNA, anti-RNP, FAN, anti-SM, ANCA and lupic anticoagulant antibodies and cryoglobulins, as well as cytomegalovirus and Zika virus (by PCR), were negative.
Imaging examination
During investigation, CT scans of chest and abdomen were carried out, as well as an echocardiogram. The CT showed a small volume of ascites, diffuse thickening of bowel walls, and a small bilateral pleural effusion (Figure 2). The echocardiogram was normal, with an ejection fraction of 67.45% and no pericardial effusion.
MULTIDISCIPLINARY EXPERT CONSULTATION
A skin biopsy was obtained from the patient's left leg and investigated by histological analysis carried out by Dr. Silvia Conde Watanabe, an expert in skin pathologies.
FINAL DIAGNOSIS
Histology of the skin biopsy showed discrete acanthosis, and neutrophil and erythrocyte exocytosis in the epidermis (Figures 3 and 4). The superficial and mediumdermis showed a moderate perivascular and interstitial inflammatory infiltrate, with a predominance of neutrophils. Focal vasculitis was also found, characterized by smallsize vessels surrounded by polymorphonuclear leukocytes and fibrinoid necrosis of their walls, along with eosinophil leukocytoclasia. A liver biopsy was also performed,and showed chronic hepatitis with moderate activity, suggesting HCV recurrence in the graft; METAVIR score of A2F1 was assigned. HCV PCR yielded 11460 copies/mL and identified the genotype as 1A.

TREATMENT
A 12-wk antiviral regimen was initiated, consisting of sofosbuvir (400 mg/d),daclatasvir (60 mg/d) and ribavirin (1000 mg/d). The patient experienced no adverse effects associated with the treatment. After 10 d, all skin lesions showed appreciable regression, and the patient remained afebrile.
OUTCOME AND FOLLOW-UP
At the 6-mo follow-up after finishing the 12-wk treatment, the patient remained well and with normal graft function. Blood tests detected no HCV, and there was no fever or any other sign of vasculitis.
DISCUSSION
Reportedly, half of the patients infected with HCV develop chronic liver disease[12]and about 30% progress to hepatic cirrhosis, with many eventually needing a liver transplant[4]. After the transplant, there is a 50% recurrence rate of the virus within the first year, and recurrence within 5 years is an almost a universal phenomenon[4].
Besides the characteristic effects on the liver, HCV can affect other organs and systems as well. Indeed, 10%-15% of patients infected with HCV develop symptomatic extrahepatic disease[13]. A small portion (2%-4%) present to clinic with leukocytoclastic vasculitis, accounting for 8%-19% of all leukocytoclastic vasculitis cases[13,14].
The most frequent HCV subtype found in cases of human HCV infection is genotype 1, corresponding to roughly 70%-75% of the cases in the United States alone[12]. Unfortunately, this is also the subtype with the greatest resistance to interferon, requiring longer treatment duration and greater doses[7]. No studies in the current literature, however, have reported on the association of leukocytoclastic vasculitis with any particular HCV genotype.
The treatment of HCV-related leukocytoclastic vasculitis focuses on the virus itself,aiming to reduce or eradicate it[10,11]. Prednisone has been used successfully in some cases of vasculitis, but it has no curative effect and can increase the HCV viral load and associated damage to the liver[15]. One case of successful treatment with tiaprofenic acid and topical clobetazole has been reported from India, with the outcome being complete resolution after 3 wk of treatment[12].

Figure 2 Computerized tomography scan showing a small volume of ascites and diffuse thickening of bowel walls (white arrow).
The most important differential diagnoses of leukocytoclastic vasculitis are other vasculitis conditions, pigmented purpuric dermatosis, acute meningococcemia,disseminated gonococcal infection, disseminated intravascular coagulation,monoclonal paraproteinemia, thrombotic thrombocytopenic purpura, Gardner-Diamond syndrome, atrial myxoma, cholesterol embolism and infectious emboli[16].
CONCLUSION
The challenge of correctly diagnosing HCV-associated leukocytoclastic vasculitis after liver transplantation lies in the great number of immunological and infectious agents that can cause similar skin lesions in immunosuppressed patients. Skin biopsy is of great importance in investigating these cases. Once specific treatment is initiated against HCV, the patient usually experiences a rapid recovery and has a favorable prognosis.
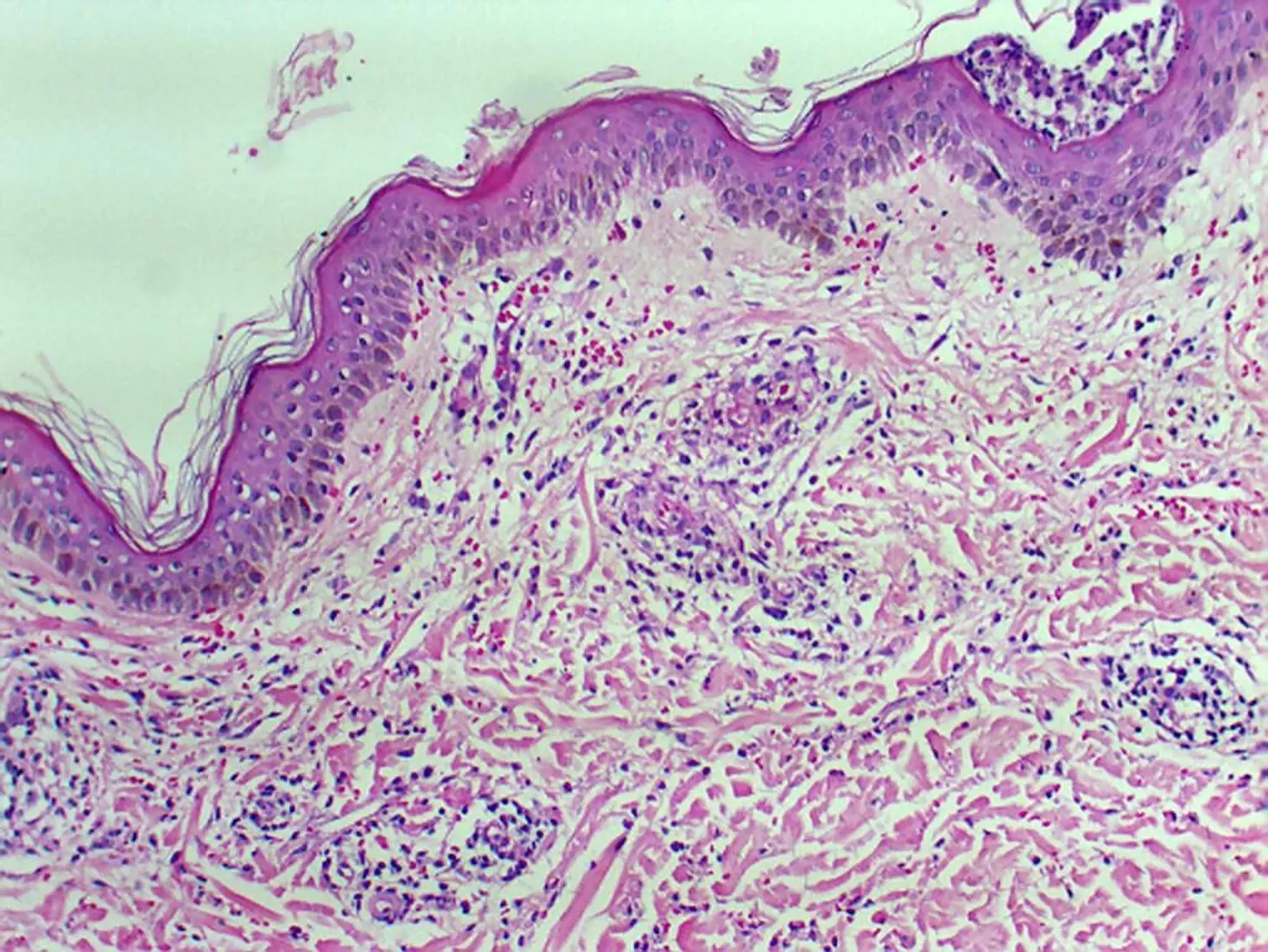
Figure 3 Focal vascular damage with mild perivascular neutrophilic infiltrate and fragmentation of the neutrophils resulting in nuclear dust(leukocytoclasis), suggestive of Urticarial vasculitis (HE 100 x).
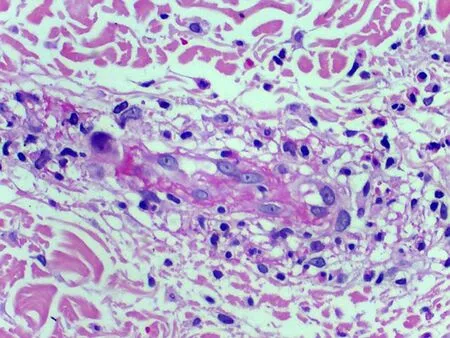
Figure 4 Perivascular neutrophilic infiltrate (HE 40 x).
 World Journal of Hepatology2019年4期
World Journal of Hepatology2019年4期
- World Journal of Hepatology的其它文章
- Yes-associated protein at the intersection of liver cell fate determination
- Nonalcoholic fatty liver disease prevalence in an Italian cohort of patients with hidradenitis suppurativa: A multi-center retrospective analysis
- Effectiveness of venous thromboembolism prophylaxis in patients with liver disease
- Being accompanied to liver discharge clinic: An easy measure to identify potential liver transplant candidates among those previously considered ineligible
- Beneficial effects of losartan or telmisartan on the local hepatic renin-angiotensin system to counter obesity in an experimental model
- MicroRNAs contribute to ATP-binding cassette transporter- and autophagy-mediated chemoresistance in hepatocellular carcinoma