
Combination of propofol and dezocine to improve safety and efficacy of anesthesia for gastroscopy and colonoscopy in adults:A randomized,double-blind,controlled trial
2019-04-18 07:23:14XueTingLiChaoQunMaSiHuaQiLiMinZhang
World Journal of Clinical Cases 2019年20期
Xue-Ting Li,Chao-Qun Ma,Si-Hua Qi,Li-Min Zhang
Xue-Ting Li,Si-Hua Qi,Li-Min Zhang,Department of Anaesthesiology,The Fourth Affiliated Hospital,Harbin Medical University,Harbin 150001,Heilongjiang Province,China
Chao-Qun Ma,Department of Neurosurgery,Harbin 242 Hospital,Harbin 150066,Heilongjiang Province,China
Abstract
Key words:Anesthesia;Dezocine;Propofol;Gastroscopy;Colonoscopy
INTRODUCTION
Gastroscopy and colonoscopy are important and common endoscopic methods for the diagnosis and treatment of gastrointestinal and colorectal diseases.Gastroscopy is used to visualize the upper part of the gastrointestinal tract(i.e.,up to the duodenum)[1,2],while colonoscopy is used to examine the large intestine and the distal part of the small intestine[3-6].However,endoscopy is usually associated with adverse reactions such as nervousness,nausea,vomiting,choking cough,and pain[7,8].Severe discomfort,such as vomiting,coughing,or body movement,may lead to aggravation of a pre-existing condition or even interruption of examination or treatment,especially in some critically ill patients with physiological dysfunction(e.g.,cardiovascular or respiratory disease)[9].The optimal methods for inducing analgesia and sedation in gastroscopy and colonoscopy are areas of ongoing debate;nevertheless,determining an appropriate regimen of sedation and analgesia is important.It has been reported that the administration of intravenous anesthetics can effectively eliminate patient anxiety,inhibit upper airway reflex,and improve patient comfort during endoscopy,which has led to an increase in patient willingness to undergo follow-up endoscopic examination or treatment[10].Previous studies have confirmed the efficacy of general anesthesia in endoscopy.The use of propofol in combination with opioids has been reported to improve sedation and analgesia with regard to recovery time,sedative effect,pain,and discomfort[11,12].The aim of the present trial was to evaluate the effects of propofol combined with dezocine,sufentanil,or fentanyl in gastroscopy and colonoscopy.Based on novel molecular targets of dezocine[13]and our preliminary observations in clinical practice,wehypothesized that a better performance may be achieved with a combination of propofol and dezocine.We observed the incidence of reflex coughing,nausea,and vomiting,cardiovascular and respiratory depression,body movement under sedation,and recovery quality when using propofol alone or combined with dezocine,sufentanil,or fentanyl.
MATERIALS AND METHODS
Study design and setting
This prospective,randomized,double-blind,controlled trial was conducted with the approval of the Medical Ethics Committee of the Fourth Affiliated Hospital of Harbin Medical University(Harbin,Heilongjian,China),and was registered with the Chinese Clinical Trial Registry(http://www.chictr.org.cn/index.aspx;Registration number ChiCTR1800017630;August 7,2018).Stratified randomization was used to assign candidate subjects to one of four groups(Figure 1)according to sex and body mass index(BMI)(two groups).Computer-generated random group numbers were printed and placed into separate sealed envelopes.When recruiting a subject who met the inclusion criteria,the assistant anesthetists assigned the patient to a group according to the number in the envelope.Both anesthesiologists and patients were blinded to the regimen.The drugs were prepared by the assistant anesthetists,labelled with numbers,and then injected by the anesthesiologist.The anesthesiologist was responsible for recording intraoperative and postoperative indexes.In cases of emergency,the anesthesiologist was to be notified of the study group to which the patient belonged by the assistant anesthetist.
Patients with American Society of Anesthesiologists class I or II,18-85 years of age,and undergoing both gastroscopy and colonoscopy were recruited.Written informed consent for anesthesia was obtained from each participant before anesthesia.Individuals > 85 or < 18 years of age,and those who were pregnant,had a BMI > 30 kg/m2,experienced active gastrointestinal bleeding,had a history of bronchial asthma or chronic obstructive pulmonary disease,upper airway infection in the previous 2 weeks,or had impaired kidney or liver function,drug abuse,sleep apnea,a known hypersensitivity to propofol or opioid,or an expected operation duration > 60 min were excluded from the study.Furthermore,participants were excluded after recruitment if the anesthesia protocol or endoscopic procedure was changed - even temporarily - for any reason.The structure of the study is illustrated in Figure 1.
Anesthesia
The sample size was estimated according to the χ2test of the incidence of the primary study end points and the incidence of hypotension and hypoxemia(30%)during endoscopy.The number of observations allowed detection of a small to moderate effective size(approximately 20%)with a 5% chance of a type I error and 90% power.The test of power remained at 80% or higher if up to 20% of subjects drop out from the study.
A total of 516 patients were recruited for this study(Figure 1).After exclusion,400 patients were randomly divided into one of four groups for sedation,with 100 subjects in each group:Dezocine(intravenous 1.0-2.5 mg/kg propofol + 0.05 mg/kg dezocine);sufentanil(1.0-2.5 mg/kg propofol + 0.10 μg/kg sufentanil);fentanyl(1.0-2.5 mg/kg propofol + 1.0 μg/kg fentanyl);and control(1.0-3.0 mg/kg propofol + 2-3 mL saline).All drugs,except for propofol,were diluted with saline.Dezocine was diluted to 1 mg/mL,sufentanil to 2.5 μg/mL,and fentanyl to 20 μg/mL.
Peripheral venous access was secured using a 22-gauge intravenous needle in the dorsum of the right hand before the patients entered the operating room.A left-side position was taken,oxygenviaa nasal cannula(3 L/min)was administered,and normal saline was infused at a rate of 10 mL/kg/h in the operating room.The bispectral index(BIS),electrocardiogram,non-invasive blood pressure,and pulse oxygen saturation(SpO2)were continuously monitored.
After entering the operating room,the patients were administered one of the three opioids or saline.Ten minutes later,propofol was administered intravenously for induction and maintenance of anesthesia.When the eyelash-conditioned reflex disappeared,the entire body relaxed,and BIS reached 40-60,gastroscopy was performed.A BIS of 40-60 is usually considered to indicate sufficient depth of general anaesthesia.All patients underwent colonoscopy after gastroscopy.During the course of the procedure,no opioids were administered intraoperatively,and anesthesia depth(BIS 40-60)was mainly controlled using propofol.During the course of the procedure,vasoactive drugs were used to maintain the variation range of mean arterial pressure(MAP)and heart rate(HR)less than 20% of pre-induction values.
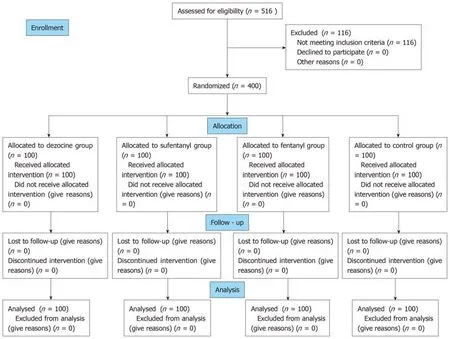
Figure 1 CONSORT 2010 flow diagram.
Intraoperative indexes included the induction time it took for the patient to lose consciousness(from injection of propofol until the eyelash conditioned reflex disappeared),the induction dosage of propofol,additional dosage of propofol,the total dosage of propofol,the incidence of reflex coughing,body movement,respiratory depression,the use of jaw thrust,the need for vasoactive drugs,duration of the procedure,and Steward score [0-6 points:An unresponsive immobile patient whose airway requires maintenance(score = 0)to a fully recovered patient(score =6)][14]when the patient wake up(open eyes as the anesthesiologist called the patient’s name or lightly tapped the patient on the shoulder).The postoperative indexes included awakening time from pulling out the colonoscope to waking up of the patient,the patient’s postoperative pain score [0-10 points,no pain(score = 0)to unbearable pain(score = 10)] at 30 min in the observation room,and the incidence of nausea and vomiting within a 24-h period.BIS,MAP,HR,SpO2,and respiratory rate(RR)were recorded at time points T1(before dosing),T2(disappearance of eyelash reflex),and T3(patient waking up).
Statistical analysis
Data were analyzed using SPSS version 22.0(IBM Corporation,Armonk,NY,United States)for Windows(Microsoft Corporation,Redmond,WA,United States),and are expressed as the mean ± SD,or number and percentage.Group comparisons regarding age,weight,height,operation duration,propofol dosage,and awakening time were performed using one-way analysis of variance(ANOVA).Values of MAP,HR,and SpO2were compared using repeated-measures ANOVA.Categorical data were compared using the chi-squared test or Fisher’s exact test.Correlation analysis was conducted on propofol dosage and some additional clinical benefits.P< 0.05 was considered to be statistically significant.
RESULTS
A total of 516 patients scheduled to undergo selective painless gastroscopy andcolonoscopy were initially assessed for eligibility between August 13,2018 and March 30,2019.Of these,116 patients were excluded for the following reasons:>85 years of age(n= 26);<18 years of age(n= 8);body weight > 30% of ideal body weight(n= 12);tachycardia(n= 19);bradycardia(n= 25);and upper airway infection in the previous 2 wk(n= 26).No severe adverse event leading to study withdrawal was observed.Ultimately,a total of 400 patients(n= 100 in each group)were enrolled in this study(Figure 1).
Demographic information
Demographic information,including sex,age,weight,height,and operation duration,were similar among the groups(P> 0.05)(Table 1).The size,shape,location,and number of polyps were similar among the groups(P> 0.05).The endoscopists were equally skilled and were similar among the groups(P> 0.05).
Propofol dosage,awakening time,Steward score,and postoperative pain score
As shown in Table 2 and Figures 2 and 3,the induction dosages,additional dosages,and total dosages of propofol in the dezocine,sufentanil,and fentanyl groups were significantly lower than those in the control group(P< 0.01).The additional dosage and total dosage of propofol in the dezocine group were significantly lower than those in the sufentanil and fentanyl groups(P< 0.01).The awakening time in the dezocine and sufentanil groups was significantly shorter compared with the control group(P< 0.01),and the awakening time in the dezocine group was significantly shorter than that in the sufentanil group(P< 0.01).Steward scores after eye opening in the dezocine and sufentanil groups were significantly higher compared with the control group(P< 0.01),and Steward score after eye opening in the dezocine group was significantly higher than that in the sufentanil group(P< 0.01).Postoperative pain scores in the dezocine group were significantly lower than those in other groups(P< 0.01).Postoperative pain scores in the sufentanil and fentanyl groups were significantly lower than those in the control group(P< 0.01).However,there were no statistical differences in awakening time or Steward score after eye opening between the fentanyl and control groups(P> 0.05).Moreover,correlation analysis showed that awakening time(r = 0.392,P< 0.001)and Steward score(r = -0.306,P< 0.001)were correlated to the total dosage of propofol.
BIS,MAP,HR,SpO2,and RR among the groups
Compared with the dezocine group,BIS was comparatively lower at T3 in the sufentanil,fentanyl,and control groups(P< 0.01)(Table 3;Figure 4A).Compared with T1,MAP and HR decreased after anesthesia induction in the fentanyl and control groups at T2(P< 0.01),and gradually increased as the operation progressed,but was still lower than the baseline value in the fentanyl and control groups at T3(P< 0.01).Compared with the dezocine and sufentanil groups,MAP was comparatively lower in the fentanyl and control groups at T2(P< 0.01)(Table 3;Figure 4B).Compared with T1,SpO2and RR decreased after anesthesia induction in the sufentanil,fentanyl,and control groups at T2(P< 0.01),and gradually increased as the operation progressed;however,there were no significant statistical differences among the four groups at T3(P> 0.05).Compared with the dezocine group,SpO2and RR were comparatively lower at T2 in the sufentanil,fentanyl,and control groups(P< 0.01)(Table 3;Figure 4C and D).
Use of vasoactive drugs and side effects
As shown in Table 4,usage of vasoactive drugs,rates of hypopnea,jaw thrust,and body movement in the dezocine group were significantly lower than those of other groups(P< 0.01).Moreover,correlation analysis showed that usage of vasoactive drugs was correlated to total dosage of propofol(r = 0.204,P< 0.001).However,no statistically significant differences in reflex coughing,nausea,or vomiting were observed among the four groups(P> 0.05).Furthermore,no patient in any group experienced therapy interruption,aspiration,or intra-operative awareness.
DISCUSSION
This study aimed to identify a comparatively satisfactory anesthetization regimen for painless gastroscopy and colonoscopy.The combination of propofol and dezocine can decrease propofol dosage,reduce the risk for the development of inhibitory effects on the cardiovascular and respiratory systems,increase analgesic effect,decrease body movement,shorten awakening time,and improve awakening quality.
The duration of gastroscopy and colonoscopy is typically approximately 45 min,and addition of propofol is needed.However,high additional dosage of propofol cansignificantly prolong recovery time,increase the risk for post-procedure respiratory depression and hypoxemia,and the workload for recovery management.Dezocine can also decrease the additional dosage of propofol in patients undergoing gastroscopy and colonoscopy,and reduce the side effects of propofol.
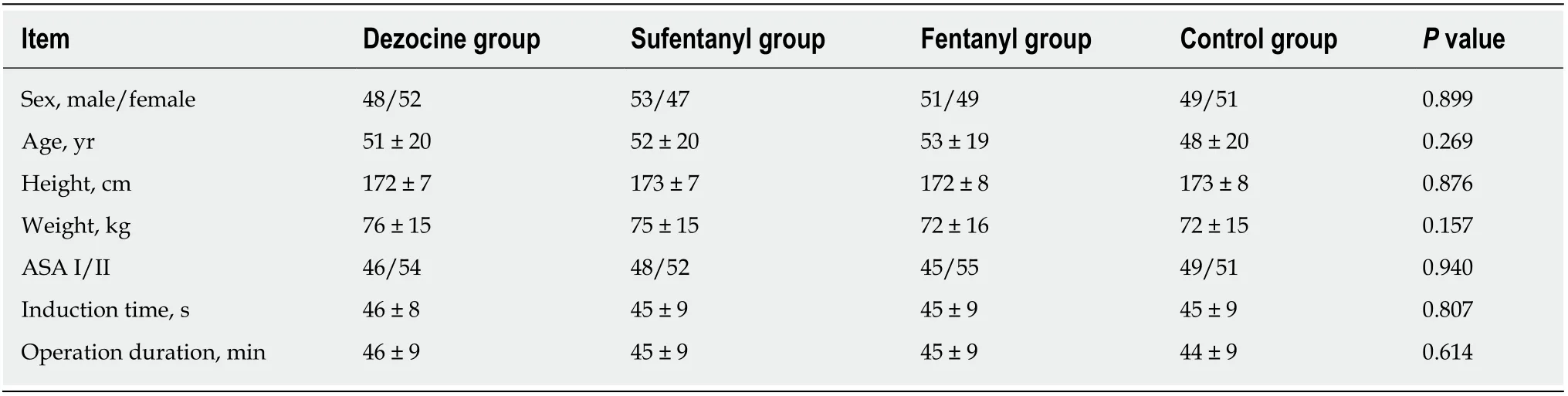
Table 1 Demographics of the four groups
In recent years,painless electronic endoscopy has been widely used in clinical practice,reducing discomfort and suffering in patients undergoing gastroscopy or colonoscopy[1,3].Presently,the generally used anesthetic drug is propofol,which is an intravenously administered sedative with a favourable sedative effect,rapid onset,and short duration of action,which results in a decreased level of consciousness and lack of memory of events[4,11,12,15].Propofol also strongly inhibits the contraction of gastrointestinal smooth muscle,antagonizes the vomiting reflex,and reduces cough and physical movement[3,16-18].However,because it lacks an obvious analgesic effect,the dosages of propofol are relatively high in painless gastroscopy and colonoscopy.High dosages of propofol usually cause inhibitory effects on the cardiovascular and respiratory systems.Similar to other opioids,dezocine has been reported to decrease anesthetic requirements by up to 50%[19].
Dezocine belongs to a class of opioid receptor agonist and antagonist drugs that exhibit strong affinity for both the mu and kappa receptors,but relatively weak interactions with the delta receptor[13,20,21],and has been used in procedures requiring propofol sedation[22]and postoperative pain management[20].Because dezocine is a partial mu receptor agonist and a kappa receptor antagonist[13,23],common side effects observed in opioids with full agonism,such as sufentanil and fentanyl,are significantly reduced.Dezocine,however,exhibits a “ceiling effect” for respiratory depression(a notorious and fatal side effect caused by commonly used clinical opiates).In anin vitrostudy,dezocine inhibited norepinephrine and serotonin reuptake in a concentration-dependent manner through two novel molecular targets(the norepinephrine transporter and serotonin transporter)[13].The interaction of dezocine with three major opioid receptors and two novel molecular targets helped to elucidate the mechanisms underlying the pharmacological effects of dezocine.
The major limitation of this study was its single-center design,which may limit the generalizability of the results.Therefore,multicenter,prospective,randomized studies will be needed to further assess the clinical effect of propofol combined with dezocine in painless gastroscopy and colonoscopy.
In conclusion,this study demonstrated that anesthesia with propofol combined with dezocine is an adequate regimen of anesthesia and analgesia for gastroscopy and colonoscopy,which can increase the patient cooperation,quality and safety of the examination and treatment,and patient and physician satisfaction with anesthesia.
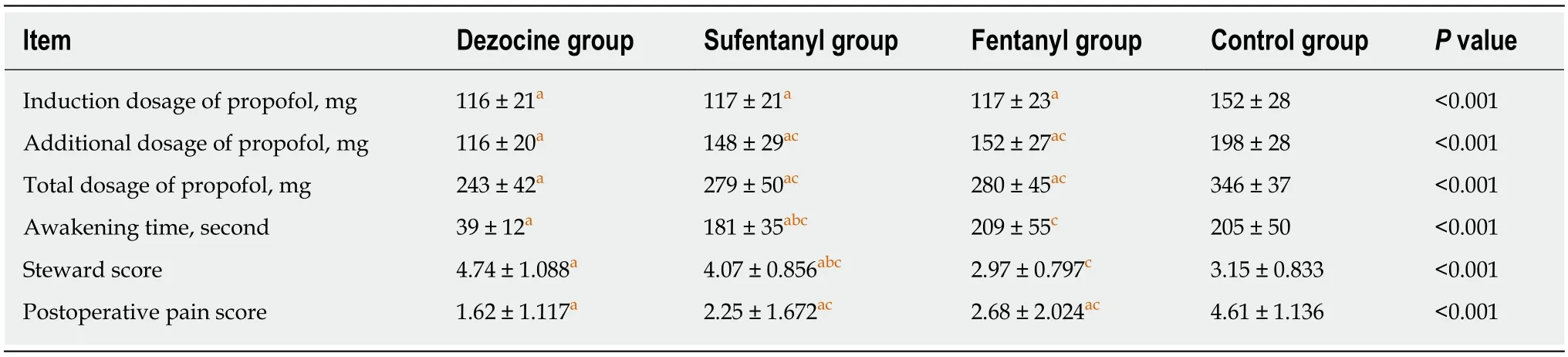
Table 2 Comparison of propofol dosage,awakening time,steward score,and postoperative pain score among the groups

Table 3 Comparison of intraoperative indexes in the four groups(x ± s)

Table 4 Usage of vasoactive drugs and side effects
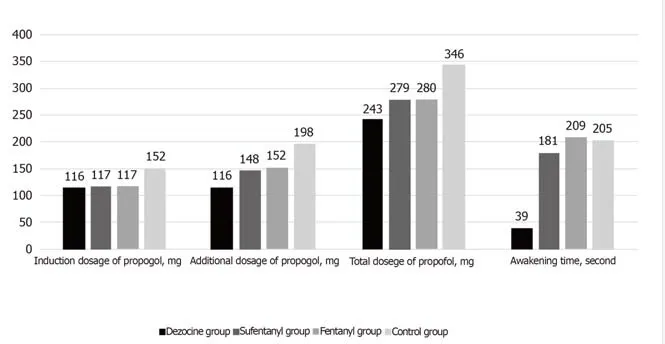
Figure 2 Dosage of propofol and awakening time among groups.

Figure 3 Steward score and postoperative pain score among groups.
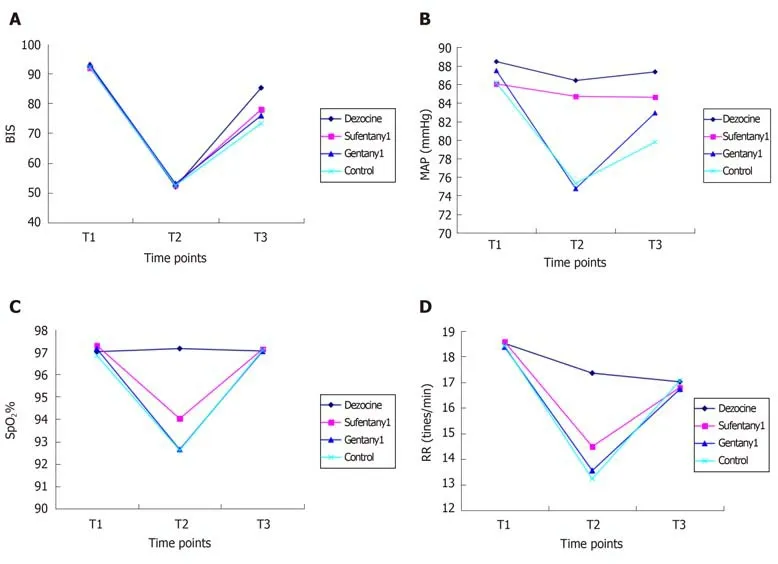
Figure 4 Variety of indexes at different time points in the four groups.
ARTICLE HIGHLIGHTS
Research background
Endoscopy is usually associated with severe adverse reactions.
Research motivation
The optimal methods for inducing analgesia and sedation in endoscopy are areas of ongoing debate.
Research objectives
To evaluate the effects of propofol combined with dezocine,sufentanil,or fentanyl in painless gastroscopy and colonoscopy.
Research methods
Patients were randomly assigned to one of four groups for anesthesia:intravenous dezocine,sufentanil,fentanyl,or saline.
Research results
Propofol dosage,bispectral index,Steward score,awakening time,postoperative pain score,mean arterial pressure,pulse oxygen saturation,rates of hypopnea,jaw thrust,body movements,and usage of vasoactive drugs in the dezocine group were significantly better than those of the other three groups.
Research conclusions
The combination of propofol and dezocine can decrease propofol dosage,reduce the risk for the development of inhibitory effects on the respiratory and cardiovascular systems,increase analgesic effect,decrease body movement,shorten awakening time,and improve awakening quality.
Research perspectives
Anesthesia with propofol combined with dezocine is an adequate regimen of anesthesia and analgesia for gastroscopy and colonoscopy,which can increase the patient cooperation,quality and safety of the examination and treatment,and patient and physician satisfaction with anesthesia.
ACKNOWLEDGEMENTS
The authors are grateful to their colleagues in the Department of Gastroenterology for their help.
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Rh-incompatible hemolytic disease of the newborn in Hefei
- Ureteral Ewing’s sarcoma in an elderly woman:A case report
- Anaplastic lymphoma kinase-negative anaplastic large cell lymphoma masquerading as Behcet's disease:A case report and review of literature
- Synchronous quadruple primary malignancies of the cervix,endometrium,ovary,and stomach in a single patient:A case report and review of literature
- Sister Mary Joseph’s nodule in endometrial carcinoma:A case report
- Alternative technique to save ischemic bowel segment in management of neonatal short bowel syndrome:A case report