
A huge pancreatic lipoma mimicking a well-differentiated liposarcoma:A case report and systematic literature review
2019-03-14 04:11:22RenYiXiaoXingYaoWeiLinWang
World Journal of Clinical Cases 2019年16期
Ren-Yi Xiao, Xing Yao, Wei-Lin Wang
Abstract
Key words: Pancreatic Lipoma; Liposarcoma; Pancreas; Case report
INTRODUCTION
Mesenchymal tumors of the pancreas are rare, and are classified by their histological origin; they represent only 1%–2% of all pancreatic tumors[1].Of these rare tumors, fatoriginating tumors (lipomas and liposarcomas) are the rarest.Intrapancreatic lipomas were found in only 0.012% of all patients undergoing routine cross-sectional imaging[2].A pancreatic lipoma must be distinguished from focal fat replacement,lipomatous pseudohypertrophy, and liposarcoma[3].For the surgeon, the most important differential diagnosis is liposarcoma, which is generally easily identified on imaging [such as computed tomography (CT)].Here, we report a huge asymptomatic pancreatic lipoma mimicking a well-differentiated liposarcoma pathologically confirmed after performing the Whipple procedure.Additionally, we found that no systematic retrospective review of pancreatic lipoma status has appeared since 2010[4].Thus, we reviewed the literature in terms of clinical manifestations and treatments.
CASE PRESENTATION
Chief complaints
A 59-year-old female presented with a pancreatic mass that had been identified during a medical examination 10 d prior.
History of present illness
She was asymptomatic and didn’t undergo any treatment at other hospitals.
History of past illness
The patient had a free previous medical history.
Personal and family history
Her medical history and family history were unremarkable.
Physical examination
she was 160 cm tall and weighed 64 kg.Her abdomen was soft and nontender with no palpable mass.
Laboratory examinations
The laboratory data were:Alanine transaminase 95.2 U/L ( reference < 40 U/L);aspartate transaminase 67.2 U/L ( reference < 35 U/L); conjugated bilirubin 7.3 μmol/L ( reference < 6.8 μmol/L); γ-glutamyl transferase 91.4 U/L ( reference < 45 U/L); carbohydrate antigen 19-9 46.0 U/mL ( reference < 39 U/mL); and serum ferritin, 423 ng/mL ( reference < 367.1 ng/mL).
Imaging examinations
Abdominal ultrasonography revealed a hypoechoic flaky lesion of maximum diameter 5.2 cm in the head of the pancreas.Subsequent contrast-enhanced CT revealed a 6.4 cm × 6.0 cm near-circular heterogeneous fat-containing lesion (?109 ±19.2 HU on contrast-enhanced CT compared to 47.9 ± 14.9 HU for the liver) in the head of the pancreas (Figure 1).The borders were indistinct and a few fibroreticular septa were evident within the lesion.The surrounding parenchyma was slightly enhanced, and the lesion was not clearly distinguishable from the pancreas.The adjacent tissues were partially compressed, including the head of the pancreas, the duodenum, and certain blood vessels (the inferior vena cava, portal vein, and superior mesenteric artery/vein).The pancreatic duct and intrahepatic bile ducts were not obviously dilated.By reference to the CT data only, we first considered that the mass might be a liposarcoma derived from the retroperitoneum.On magnetic resonance imaging, the mass was of high signal intensity on T2-weighted axial imaging, being isointense to the subcutaneous and intra-abdominal fat.And the fat-suppressed T1-and T2-weighted images revealed signal intensity losses, indicating that the mass was composed principally of adipose tissue (Figure 2).A few fibroreticular septa were evident within the lesion.The boundary between the lesion and the pancreas was unclear.Thus, the mass was most likely a well-differentiated liposarcoma derived from retroperitoneal fat.Magnetic resonance cholangiopancreatography revealed no dilatation or stenosis of the intrahepatic bile duct or pancreatic duct, but the middle and lower parts of the common bile duct were partially compressed.An abnormal 6.2 cm × 6.0 cm circular mixed/fatty signal emanated from the head of the pancreas(Figure 3).On positron-emission tomography/CT, the lesion had the density of fat,exhibited low fluorodeoxyglucose uptake, excluded evident distant metastasis, and was thus thought to be a non-malignant fat-derived tumor first, but it still cannot be distinguished from a well-differentiated liposarcoma.
Treatment
Given the huge size and the compression of the middle and lower parts of the common bile duct and important blood vessels, we suggested surgery even if the lesion was benign.We planned total surgical excision, but found that the upper part of the mass was tightly connected to the pancreas and could not be completely excised.We feared that complete removal would increase the risk of injury to the pancreatic duct and superior mesenteric vein, which might trigger a major intraoperative hemorrhage and a postoperative pancreatic fistula that could erode the superior mesenteric vein and cause a massive hemorrhage or other complications.Thus, we switched to a pancreatoduodenectomy.
FINAL DIAGNOSIS
The final pathological examination confirmed a giant lipoma of the pancreas; the largest diameter was 13.0 cm (Figure 4).Two lymph nodes near the pancreas and three around the stomach evidenced chronic lymphadenitis.Pathology also revealed chronic cholecystitis with cholesterol polyps.
OUTCOME AND FOLLOW-UP
Postoperatively, we controlled an elevated blood glucose level, abnormal liver function, and hyperamylasemia, and the patient was discharged to home with a peritoneal drainage tube on postoperative day 25.She followed regularly to the department of general surgery.
LITERATURE REVIEW

Figure 1 Computed tomography scans before treatment.
In the time since the first report[5], 169 cases of pancreatic lipoma have been reported in 48 articles[1-3,5-49], including 10 in Chinese.Most cases were diagnosed by imaging(such as CT); only 22 were confirmed by pathology, 16 of which underwent surgery and 6 endoscopic ultrasound/fine needle aspiration (FNA).Only 2 patients underwent both FNA and surgery; these exhibited massive vascular compression by the tumor[34]and elevated serum bilirubin and alkaline phosphatase levels[15].However, the FNA data were not described.Some have argued that pancreatic lipomas are not rare[2,22].The sexes of 162 of the 169 cases were identified:87 males and 75 females.Their ages ranged from 11 months to 88 years.Lipomas are most commonly found in the middle-aged and elderly, possibly because they undergo physical examinations more often than do the young.The pancreatic lipoma locations were:The head (n= 70); the head and the uncinate process (n= 1); the uncinate process (n= 15); the head and neck (n= 2); the neck (n= 9); the neck and body (n= 1);the body (n= 30); the body-tail junction (n= 3); the tail (n= 34); and not mentioned (n= 4) .Only a few tumors were of diameter > 50 mm:< 50 (n= 150); 50–100 (n= 9); and> 100 mm (n= 3).Most patients were asymptomatic and required only follow-up or conservative treatment (n= 132); only 16 required operations, including pancreatoduodenectomy (7), tumor enucleation from the head (3), subtotal pancreatectomy and splenectomy (1), pancreatic tail resection (1), biliary bypass (1),and not mentioned (3).In patients who underwent surgery, postoperative complications were mentioned in only two cases; these were an elevated blood glucose level and a pancreatic fistula.
DISCUSSION
A pancreatic lipoma is a rare solid tumor, the etiopathogenesis of which remains unclear although lipomas located in the pancreatic head have been considered to be adipose tissue trapped during posterior rotation of the ventral pancreatic bud[22,48].
CT is the most useful radiological method to diagnose pancreatic lipoma[4].The density of a liposarcoma in CT is higher than that of normal fat and benign fatty masses, and indistinct borders[50], thick septa[48,51], a larger size[48,52](> 5 cm, and in most cases > 10 cm)[1], calcification[48,52]and rapid growth[48]are significant indicators of malignancy.Features of well-differentiated liposarcoma include large lesion size,presence of thick septa, presence of nodular and/or globular or non-adipose mass-like areas, and decreased percentage of fat composition[52].A lipoma is usually well circumscribed, of the density of normal fat, homogenous[4], noninvasive[50], stable and devoid of symptoms.However, it is not easy to distinguish a lipoma from a welldifferentiated liposarcoma due to the radiographic similarities between these two lesions[4](Table 1).
To our knowledge, our case is the first example of a suspected well-differentiated liposarcoma that was actually a pancreatic lipoma.The tumor of our present patient was around 6.2 cm × 6.0 cm in dimensions, indistinct from the pancreas, contained a few fibroreticular septa, and the surrounding parenchyma was slightly enhanced.We first thought that the mass was a well-differentiated liposarcoma derived from the retroperitoneum.Despite that positron emission tomography/CT showed low fluorodeoxyglucose uptake, the diagnosis was still uncertain.Thus, given the huge size and the compression of the middle and lower parts of the common bile duct and important blood vessels, we suggested surgery even if the lesion was benign.We planned total surgical excision, but found that the upper part of the mass was tightly connected to the pancreas and could not be completely excised.We feared that complete removal would increase the risk of injury to the pancreatic duct and superior mesenteric vein, which might trigger a major intraoperative hemorrhage and a postoperative pancreatic fistula that could erode the superior mesenteric vein and cause a massive hemorrhage or other complications.Thus, we switched to a pancreatoduodenectomy.
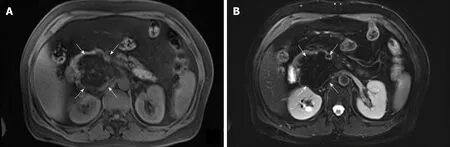
Figure 2 Magnetic resonance scans before treatment.
Pancreatic lipoma seems to exhibit no gender bias, is usually diagnosedviaCT or other imaging methods, and most commonly occurs in the head of the pancreas.The maximum diameter is often less than 5 cm.Generally, small, asymptomatic noncompressed lipomas require follow-up only.Very few cases exhibit significant shortterm changes, but the lipoma may grow in the long term[25].Patients may elect to undergo trans-duodenal core needle biopsy if the tumor is difficult to identify on imaging.Surgery is recommended if a malignancy is in play.However, it is sometimes difficult to distinguish lipomas from well-differentiated liposarcomas[53].A combination of FNA data and MDM2 genetic analysis improves the liposarcoma detection rate[54,55].In addition, short-term close follow-up may identify patients with enlarging lesions that require surgery.Compressive lesions, such as that of our present case, require excision; the choice of surgery varies by the intraoperative presentation.
CONCLUSION
In summary, pancreatic lipomas are rare, especially the huge ones, no obvious gender bias, and most commonly occur in the head of the pancreas.Small, asymptomatic non-compressed lipomas require follow-up only.Surgical excision should be considered when the tumor has compressed important tissues or is difficult to distinguish from a liposarcoma, the choice of surgery depends on the intraoperative presentation.
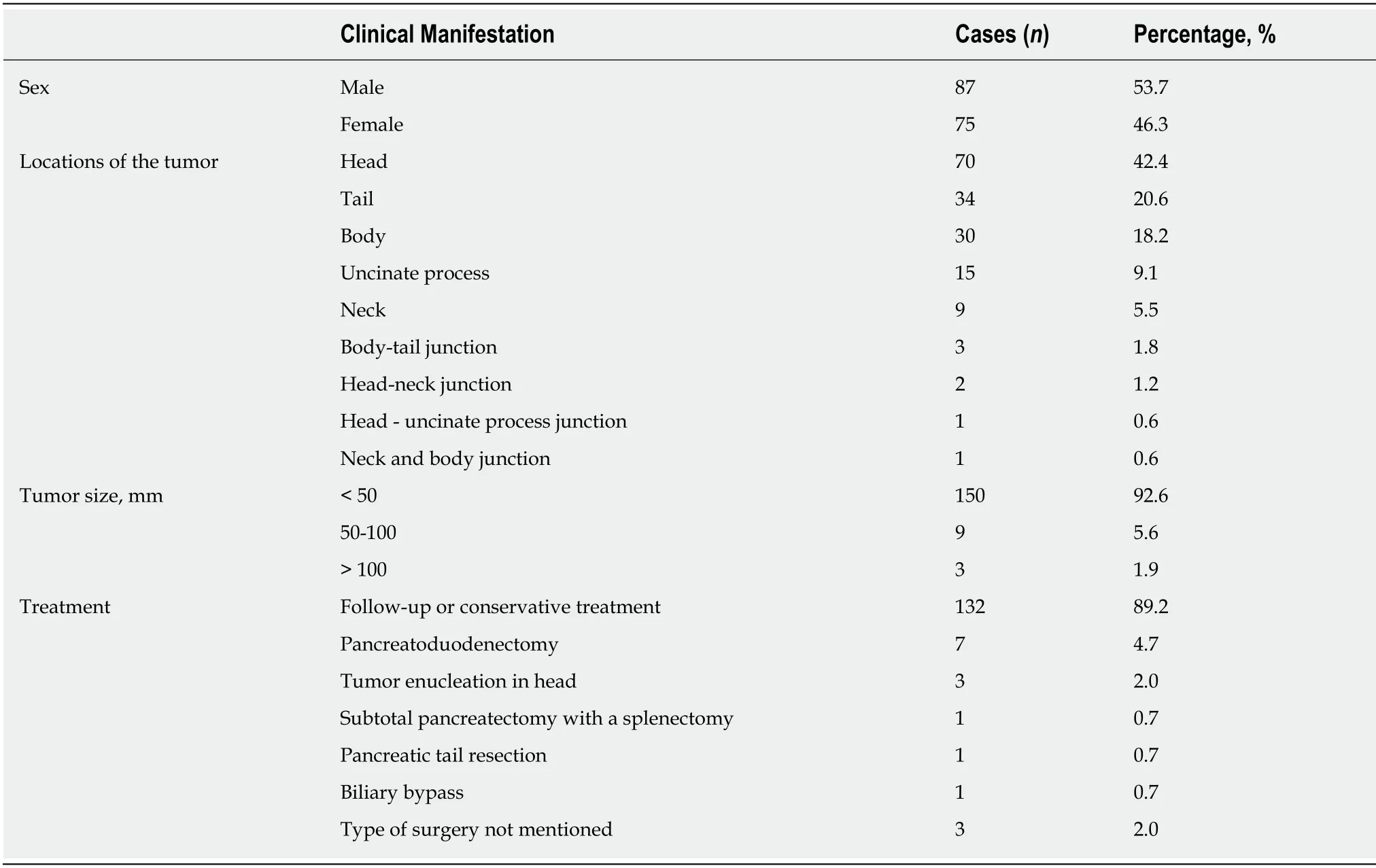
Table 1 Clinical features of pancreatic lipoma

Figure 3 Coronary magnetic resonance scan and magnetic resonance cholangiopancreatography before treatment.
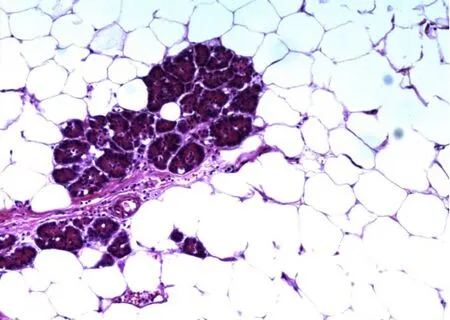
Figure 4 Final pathological examination.
 World Journal of Clinical Cases2019年16期
World Journal of Clinical Cases2019年16期
- World Journal of Clinical Cases的其它文章
- Malignant syphilis accompanied with neurosyphilis in a malnourished patient:A case report
- Ex vivo revascularization of renal artery aneurysms in a patient with solitary kidney:A case report
- Pseudothrombus deposition accompanied with minimal change nephrotic syndrome and chronic kidney disease in a patient with Waldenstr?m's macroglobulinemia:A case report
- Hepatocellular carcinoma successfully treated with ALPPS and apatinib:A case report
- Treatment of invasive fungal disease:A case report
- Acute pancreatitis connected with hypercalcemia crisis in hyperparathyroidism:A case report