
Role of abdominal drainage in bariatric surgery:Report of six cases
2019-03-14 04:11:18YangLiuMengYiLiZhongTaoZhang
World Journal of Clinical Cases 2019年16期
Yang Liu, Meng-Yi Li, Zhong-Tao Zhang
Abstract
Key words: Abdominal drainage; Morbid obesity; Bariatric surgery; Hemorrhage; Case report
INTRODUCTION
The prevalence of morbid obesity is increasing worldwide, and the number of bariatric surgery procedures is accordingly increasing each year[1].As in other abdominal surgeries, hemorrhage is a challenging issue for bariatric surgeons.Abdominal drainage allows for timely detection of hemorrhage, but it cannot prevent hemorrhage.Whether routine abdominal drainage is needed during bariatric procedures remains controversial[2].Few reports describe the role of abdominal drainage in the diagnosis and treatment of abdominal hemorrhage in bariatric surgery.We herein present six cases of abdominal hemorrhage in bariatric procedures performed in our center.
CASE PRESENTATION
Case 1
A 37-year-old man with a body mass index (BMI) of 33.73 kg/m2underwent laparoscopic sleeve gastrectomy (LSG) with cholecystectomy due to cholecystolithiasis.Abdominal hemorrhage was found on the first postoperative day, and the patient exhibited an accelerated heart rate of 100 to 120 beats per minute (bpm)compared with the preoperative baseline of 60 to 70 bpm.His blood pressure and urine volume remained steady, and conservative treatment was implemented (bed rest, hemostasis, and fluid infusion).The patient’s condition stabilized on postoperative day 4.His hemoglobin level decreased from 15.7 g/dL to 8.0 g/dL, and transfusion of 8 U of red blood cells was therefore performed.On postoperative day 8,800 mL of blood was percutaneously drained from a pelvic hematocele that had formed.The patient did not require a reoperation and was discharged on postoperative day 10.However, an encapsulated effusion was found in his abdominal cavity by abdominal magnetic resonance imaging at the 3-mo follow-up (Figure 1).Because he had no symptoms, conservative observation was still recommended.
Case 2
A 32-year-old man with a BMI of 33.46 kg/m2underwent LSG.Hemorrhage was found on the first postoperative day by routine blood tests and bedside ultrasound examinations.After 48 h of conservative treatment, his condition stabilized and his hemoglobin level decreased by 4.1 g/dL without a blood transfusion.However, he developed a fever of 39 oC on postoperative day 4.Physical examination revealed tenderness in the epigastrium without guarding or rebound.Antibiotics were administered and 200 mL of blood was percutaneously drained from a pelvic hematocele that had formed; however, the fever did not improve.Abdominal ultrasound findings were normal, but a computed tomography scan showed free air in the peritoneal cavity (Figure 2A).Considering the patient’s increasing generalized abdominal pain and fever, a reoperation was performed on postoperative day 6 to place a drainage tube and confirm whether gastric leakage was present.A large number of blood clots were found in the greater curvature of the stomach during the operation, but neither the location of the abdominal hemorrhage nor the presence of gastric leakage was found.The blood clots were thoroughly cleared and an abdominal drainage tube was placed on the greater curvature side of the stomach.The patient’s recovery was quite rapid after the second operation.On postoperative day 3, after the second surgery, no gastric leakage was detected by upper gastrointestinal radiography (Figure 2B), and oral liquid feeding was started.On day 10, the drainage tube was removed and the patient was discharged with no other complications.
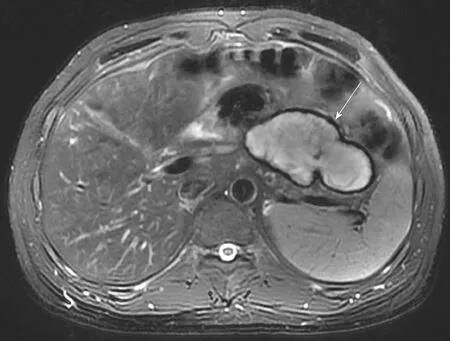
Figure 1 An encapsulated effusion was found in the abdominal cavity of the patient in Case 1 at the 3-mo follow-up.
Case 3
A 20-year-old woman with a BMI of 35.7 kg/m2underwent LSG.Hemorrhage was found on the first postoperative day by routine blood tests and bedside ultrasound examinations.After 12 h of conservative treatment, the patient’s vital signs remained unstable and her hemoglobin level declined from 14.1 to 7.9 g/dL.A computed tomography scan showed a large number of blood clots behind the stomach (Figure 3), which was a difficult area to drain percutaneously.A reoperation was performed for hemostasis and placement of a drainage tube.The location of hemorrhage was not found by laparoscopy.The blood clots were thoroughly cleared, and an abdominal drainage tube was placed on the greater curvature side of the stomach.During the second postoperative period, the patient’s recovery was quite rapid.On postoperative day 2, oral liquid feeding was started.On day 7, the drains were removed and the patient was discharged with no other complications.
Case 4
A 47-year-old man with a BMI of 32.8 kg/m2underwent laparoscopic Roux-en-Y gastric bypass (LRYGB).
Case 5
A 42-year-old man with a BMI of 30.2 kg/m2underwent LRYGB.
Case 6
A 32-year-old woman with a BMI of 30.9 kg/m2underwent laparoscopic single anastomosis gastric bypass.
In all of the last three cases, abdominal drainage was performed during the first surgery.Abdominal hemorrhage was found through the drainage tube on the day of the operation.The patients’ heart rate, blood pressure, and urine volume remained steady, and conservative treatment was implemented (bed rest, hemostasis, and fluid infusion).The hemorrhage stopped after the hemoglobin level decreased to 4.4, 3.1,and 6.1 g/dL, respectively, within 48 h.The amount of hemorrhage from the drainage tube was 480, 910, and 750 mL, respectively.In Case 4, 370 mL of blood was percutaneously drained from a pelvic hematocele that had formed.No patients required a reoperation, and no abdominal infection developed.
DISCUSSION
According to previous reports, the probability of abdominal hemorrhage after bariatric surgery ranges from 1.5% to 2.0%[3].In total, 343 metabolic procedures have been performed in our center this year, among which six cases of hemorrhage occurred (incidence of 1.7%).All six cases were treated by an experienced surgeon who had surgical experience with > 400 LSG procedures and > 100 gastric bypass procedures.The gastric staple line is reinforced by sutures in the LSG procedure, but not in the gastric bypass procedure.A review of the operative videos showed that the surgical process was relatively smooth in all six cases.The origin of hemorrhage was most likely to be the omental margin in the LSG procedure and the gastric staple line in the gastric bypass procedure.
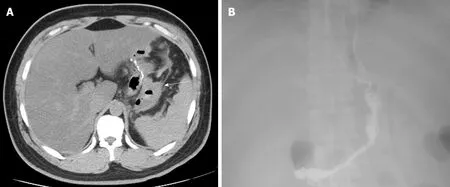
Figure 2 lmaging findings in Case 2.
The concept of enhanced recovery after surgery has gradually gained popularity in recent years[4,5].Day-case bariatric surgery has been adopted in some bariatric and metabolic centers[6].Changet al[7]suggested that omission of drainage may contribute to a shorter time to flatus passage.Doumouraset al[8]suggested that the use of routine abdominal drainage should be restricted to very select, high-risk cases.Drains can increase postoperative pain, lengthen the hospital stay, increase morbidity, and result in a marked peritoneal inflammatory response[9,10].The concept of no routine abdominal drainage is being advocated by increasingly more surgeons.
The hemorrhage in five of the six cases was controlled by conservative treatment(success rate of 83.3%).Abdominal hemorrhage was found through the drainage tube on the day of the operation in the three patients with abdominal drainage during the first surgery.Emergency treatment was initiated, and their conditions gradually stabilized within 48 h.No patients required a reoperation.Abdominal hemorrhage was found later in the patients without abdominal drainage.Although the hemorrhage was controlled by conservative treatment in Cases 1 and 2, reoperation and percutaneous drainage were performed for abdominal infection and pelvic hemorrhage.An obsolete encapsulated effusion that may require treatment in the future was left in the abdominal cavity of a patient (Case 1).The clinical outcomes of the six cases varied greatly depending on whether abdominal drainage was implemented.Therefore, we believe that it should be in a very prudent way to popularize no routine drainage in bariatric surgery.Hemorrhage cannot be prevented by abdominal drainage, but it can be detected in a timely manner, allowing for immediate implementation of the necessary treatment.When hemorrhage occurs, the greater clinical significance of drainage is to drain the hematocele and reduce the formation of blood clots behind the stomach; such clots developed in the three cases without abdominal drainage in the present study.Blood clots are a likely reason for reoperation because they may lead to the development of infections and are difficult to drain out by other drainage methods.
However, controlled studies with a larger sample size are needed to evaluate the significance of drainage in bariatric/metabolic surgery more objectively.
CONCLUSION
The possibility of controlling abdominal hemorrhage after bariatric/metabolic surgery by conservative treatment is high.When hemorrhage occurs, abdominal drainage can reduce the probability of reoperation by reducing the formation of blood clots behind the stomach; such clots may lead to the development of infections or persistent residue in the abdominal cavity.
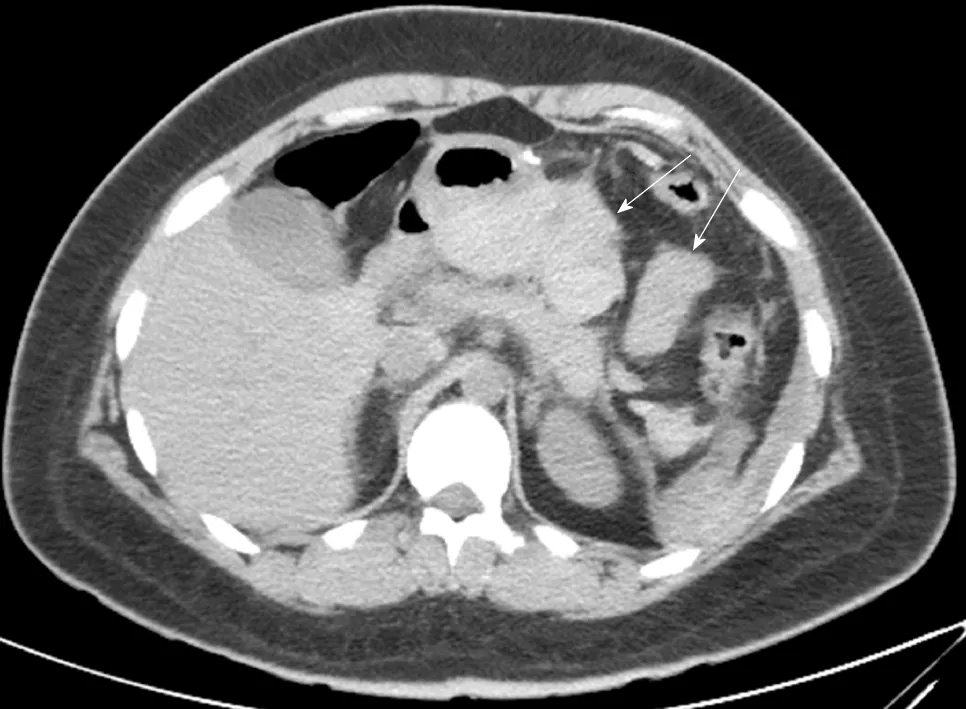
Figure 3 Blood clots behind the stomach were found in Case 3.
 World Journal of Clinical Cases2019年16期
World Journal of Clinical Cases2019年16期
- World Journal of Clinical Cases的其它文章
- Malignant syphilis accompanied with neurosyphilis in a malnourished patient:A case report
- Ex vivo revascularization of renal artery aneurysms in a patient with solitary kidney:A case report
- Pseudothrombus deposition accompanied with minimal change nephrotic syndrome and chronic kidney disease in a patient with Waldenstr?m's macroglobulinemia:A case report
- Hepatocellular carcinoma successfully treated with ALPPS and apatinib:A case report
- Treatment of invasive fungal disease:A case report
- Acute pancreatitis connected with hypercalcemia crisis in hyperparathyroidism:A case report