
A clinical analysis of acute pancreatitis in pregnancy
2017-06-19 17:22:21Ben-LanYin,Xiao-DongFu
A clinical analysis of acute pancreatitis in pregnancy
To the Editor:
Acute pancreatitis in pregnancy (APIP) is one of the acute abdomen in pregnancy. Once the disease deteriorated rapidly, it could be a serious threat to gravida and fetus. Although the incidence of APIP has been gradually increasing due to the life style change,[1]it is still a rare disease and the mechanism is not clear. Patients with APIP were often misdiagnosed and not managed properly.[2]
The present study included 31 APIP patients diagnosed from January 2005 to June 2015 and treated in our hospital. Diagnostic standard was the classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus.[3]Patients with hyperlipidemic acute pancreatitis were defined as those who had clinical presentations of acute pancreatitis, elevated triglyceride (>11.30 mmol/L in the absence of lactescent serum, or 5.65-11.30 mmol/L with lactescent serum).[4]
There were 15 (48.4%) mild cases, 1 in the first trimester, 3 in the second trimester and 11 in the third trimester; eight (25.8%) moderately severe cases, 3 in the second trimester and 5 in the third trimester; eight (25.8%) severe patients, 1 in second trimester and 7 in third trimester. Twelve (38.7%) were hyperlipidemic acute pancreatitis. Five (16.1%) caused by gallstones and 14 (45.2%) were idiopathic. Patients’ average age was 29.4 years old and average gestational time was 31.0 weeks. There were 10 primiparas (32.3%) and 21 multiparas (67.7%), all of which were monocyesis. On average, from 2005 to 2010, 1 case suffered from APIP yearly. From 2011 to 2012, 3.5 cases were treated yearly. From 2013 to 2014, 6.5 cases were administrated to hospital yearly. From January 2015 to June 2015, 5 cases were treated.
For clinical manifestation, all patients had different grade of abdominal pain, 27 cases had nausea and vomiting, 9 had radiating pain and 1 with dyspnea. Physical examination showed that 7 patients had fever (mean 38.4 ℃), 30 had abdominal tenderness. The laboratory examination (Table 1) showed that 22 patients had hypertriglyceridemia and hyperglycemia at the same time. The highest blood glucose level was 40.35 mmol/L. Ultrasound demonstrated that pancreatitis was detectable in 22 patients, 8 had no obvious abnormality and 1 pancreas was not well detected due to fetus’ factor.
Therapeutic strategies for patients with APIP are the same as regular pancreatitis: fasting, gastrointestinal decompression, positive fluid resuscitation and secretion inhibition of pancreatin and gastric acid. Antibiotics and nutrition support are also applicable. Patients with hyperglycemia were treated with insulin to control blood glucose. Albumin was used to ameliorate hypoproteinemia and reduce exudation around pancreas. If the patient has seroperitoneum, paracenteses is needed. Seventeen gravidas terminated their pregnancy in the third trimester, including 7 eutocia and 10 cesarean section, two of the patients with cesarean section had pancreatic drainage. Seven cases terminated the pregnancy in second trimester, 4 abandoned fetuses and demanded odinopoeia, 1 underwent odinopoeia due to intrauterine fetal death (IUFD). One case of first trimester didn’ t know she had pregnancy before hospitalization, so she chose induced abortion after improvement of the disease.
Among 8 patients of first and second trimester, 1 suffered from IUFD, 7 with mild and moderately severe pancreatitis, 5 demanded to terminate pregnancy and 2 continued the gravidity. In 23 patients of third trimester, 7 had severe pancreatitis, 4 had IUFD and 3 delivered live newborns; 16 cases had mild and moderately severe pancreatitis, their fetuses and newborns were all survived (Table 2).
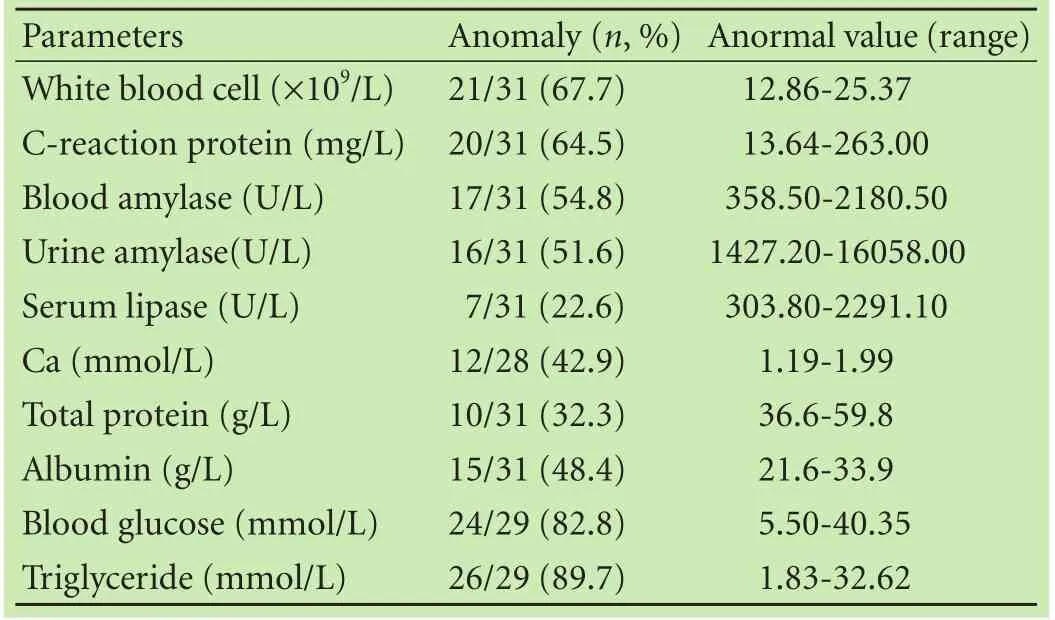
Table 1. Results of laboratory examination
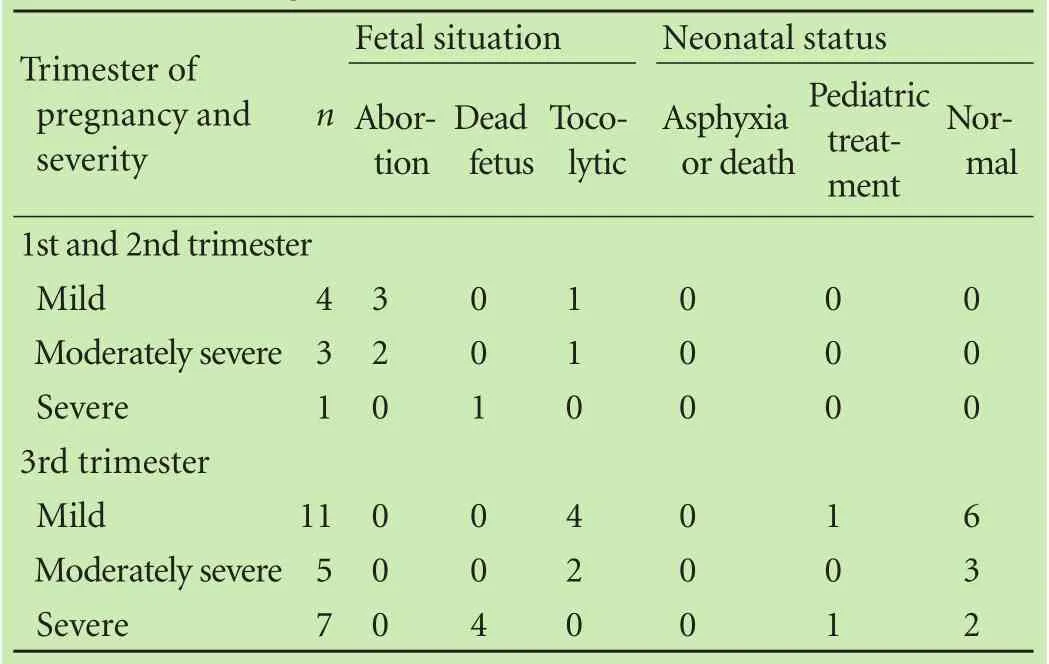
Table 2. Ending of fetuses and newborns in three trimesters
The primary endpoint of APIP was cure. Three patients with severe APIP died of multiple organ failure, septicemia or superinfection. One patient with severe APIP underwent cesarean section with pancreatic drainage. The baby was survived but the mother died because of septicemia. One patient was treated conservatively. However, when IUFD was diagnosed, the pregnancy was terminated and the patient was transferred to ICU, she died finally because of multiple organ failure. One case had hydrothorax and ascites, the IUFD was diagnosed before hospitalization. She was treated conservatively first and then paracenteses. She died due to the deterioration of the disease and superinfection. For the mild and moderately severe cases, all mothers survived no matter whether they terminated or continued pregnancy (Table 3).
Although there is no epidemiologic data up to now, the incidence of APIP is low. However, The number of pregnant patients with acute pancreatitis admitted to our hospital trend to be increasing, especially in recent three years.
The etiology of APIP is more complex and the current clinical research shows that the following factors may play a role. 1) Mechanical compression: during pregnancy, the enlarged uterus may squeeze the pancreas, resulting in pancreatic duct obstruction, pancreatic enzymes were activated by the pancreatic juice reflux. The enlarged uterus also may compress intestine and cause intestinal juice reflux into the pancreatic to activate pancreatic enzymes.[5]Additionally, the enlarged uterus may inhibit the peristalsis of bile duct which leads to cholestasis and sediment like stone formation and increases the risk of biliary pancreatitis; 2) the increase of blood viscosity: during pregnancy, the aggregation ability of red blood cell is increased and deformation ability of red blood cell is reduced, and triglyceride and cholesterol levels in blood are increased by the effect of human chorionic gonadotrophin in pregnancy, which increase the blood viscosity and jeopardize pancreatic blood circulation.[6]Patient with pregnancy is vulnerable to acute pancreatitis; 3) abnormal lipid and glucose metabolism: the high-fat-diet is reported to be an important inducer of APIP.[7]About 38.7% of our patients had hyperlipidemia which was consistent with the above view points. In addition, 22 of the patients with hyperlipidemia also had hyperglycemia, suggesting that abnormal lipid and glucose metabolism are related to APIP. Another study[8]from the United States pointed out that the most common cause of APIP is gallstone-related (>50%). But only 5 (16.1%) of APIP is gallstone-related in our study. The differences in two groups may reflect regional differences and also need more cases to clarify.

Table 3. Ending of mothers and length of hospital stay in different therapies
The diagnosis of APIP mainly depends on three aspects: clinical symptoms and signs, detection of activation of amylase in blood and urine and imaging analysis. Some authors have reported the misdiagnosis of APIP[2]and suggested that differential diagnosis of abdominal pain is important for uterine rupture, placental abruption and acute appendicitis. The activated amylase in blood and urine should be more than 3 times of the upper normal value. If the increased amylase does not reach the diagnostic criteria, the imaging findings are necessary for the diagnosis of APIP. However, for the late pregnancy or full-term, the image analysis may be not sensitive enough to the diagnosis and the clinical symptoms and signs are more helpful.
APIP may progress rapidly and threaten to maternal and fetal life. The common treatments include fasting, rehydration, inhibition of enzymes and gastric acid. The use of antibiotics is controversial. Some scholars believe that the infection should be controlled.[9]Seven of our patients had elevated white blood cells and temperature; these patients were treated with antibiotics.
There is no standard whether the pregnancy needs to be terminated in APIP patients. Some suggested conservative therapy.[10]The mild and moderately severe cases in our study had good outcomes no matter whether terminated pregnancy or conservative treatment before terminating or continuing the pregnancy. For the severe cases, these two therapies had little difference in mortality, but the length of hospital stay for the patients with terminated pregnancy (12.67 days) was significantly shorter than those with conservative treatment (29.80 days). Five out of 8 patients with severe APIP experienced IUFD. However, there was no IUFD in mild and moderate severe cases. Thus, for the severe cases, termination of pregnancy releases the mechanical compression of uterus, prevents IUFD and improves maternal and child outcomes. Mali[8]demonstrated that laparoscopiccholecystectomy or endoscopic sphincterotomy should be performed for gallstone-related pancreatitis.
The prevention of APIP should include: 1) control diet, body weight, hyperlipidemia and hyperglycemia; 2) For those with chronic cholecystitis or cholelithiasis, proper treatment should be performed before pregnancy.
In conclusion, APIP progresses rapidly and has serious consequences. The mild and moderately severe patients have good outcomes. For the patients with severe APIP, early termination of pregnancy decreases the mortality for both mother and fetus and improves outcomes.
Ben-Lan Yin and Xiao-Dong Fu
Department of Obstetrics and Gynecology, the Affiliated Hospital of Southwest Medical University, Luzhou 646000, China (Yin BL and Fu XD)
Contributors:FXD proposed the study. YBL performed the research, collected and analyzed the data and wrote the first draft. Both authors contributed to the design and interpretation of the study and to further drafts. FXD is the guarantor.
Funding:None.
Ethical approval:The study was approved by the Institutional Ethics Committee of our hospital.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Pitchumoni CS, Yegneswaran B. Acute pancreatitis in pregnancy. World J Gastroenterol 2009;15:5641-5646.
2 Pallavee P, Samal S, Gupta S, Begum J, Ghose S. Misdiagnosis of abdominal pain in pregnancy: acute pancreatitis. J Clin Diagn Res 2015;9:QD05-QD06.
3 Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102-111.
4 Yang N, Zhang DL, Hao JY. Coagulopathy and the prognostic potential of D-dimer in hyperlipidemia-induced acute pancreatitis. Hepatobiliary Pancreat Dis Int 2015;14:633-641.
5 Hernandez A, Petrov MS, Brooks DC, Banks PA, Ashley SW, Tavakkolizadeh A. Acute pancreatitis and pregnancy: a 10-year single center experience. J Gastrointest Surg 2007;11:1623-1627.
6 Ramin KD, Ramin SM, Richey SD, Cunningham FG. Acute pancreatitis in pregnancy. Am J Obstet Gynecol 1995;173:187-191.
7 Gürsoy A, Kulaksizoglu M, Sahin M, Ertugrul DT, Ozer F, Tutuncu NB, et al. Severe hypertriglyceridemia-induced pancreatitis during pregnancy. J Natl Med Assoc 2006;98:655-657.
8 Mali P. Pancreatitis in pregnancy: etiology, diagnosis, treatment, and outcomes. Hepatobiliary Pancreat Dis Int 2016;15:434-438.
9 Villatoro E, Mulla M, Larvin M. Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute pancreatitis. Cochrane Database Syst Rev 2010;(5):CD002941.
10 Li HP, Huang YJ, Chen X. Acute pancreatitis in pregnancy: a 6-year single center clinical experience. Chin Med J (Engl) 2011;124:2771-2775.
Published online May 3, 2017.
Xiao-Dong Fu (Email: dongerfu@163. com)
10.1016/S1499-3872(17)60017-1)
 Hepatobiliary & Pancreatic Diseases International2017年3期
Hepatobiliary & Pancreatic Diseases International2017年3期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Circulating autoantibodies to endogenous erythropoietin are associated with chronic hepatitis C virus infection-related anemia
- Crosstalk of liver immune cells and cell death mechanisms in different murine models of liver injury and its clinical relevance
- Patients with early recurrence of hepatocellular carcinoma have poor prognosis
- Hepatobiliary & Pancreatic Diseases International
- Traditional surgical planning of liver surgery is modified by 3D interactive quantitative surgical planning approach: a single-center experience with 305 patients
- Combined cavo-atrial thrombectomy and hepatectomy in hepatocellular carcinoma