
Acute airway emergency caused by an organic foreign body located in the laryngeal mucosa
2017-04-20 01:42:50FreyaDroegeAnkeSchlueterStefanHansenStephanLangNinaDominas
Freya Droege, Anke Schlueter, Stefan Hansen, Stephan Lang, Nina Dominas
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Essen, University Duisburg-Essen, Hufelandstrasse 55, 45147 Essen, Germany
Acute airway emergency caused by an organic foreign body located in the laryngeal mucosa
Freya Droege, Anke Schlueter, Stefan Hansen, Stephan Lang, Nina Dominas
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Essen, University Duisburg-Essen, Hufelandstrasse 55, 45147 Essen, Germany
World J Emerg Med 2017;8(2):155–156
INTRODUCTION
Organic material (e.g. nuts in children and bones or food in adults) is the most common foreign body inhaled by patients. Just one tenth of all foreign bodies in the airway are located in the larynx.[1]Laryngeal foreign bodies among adults are rarely seen but can be a life threatening event requiring immediate lifesaving intervention.[2,3]Here, we report an unusual case of a 56-year-old male patient presenting with sudden dyspnea due to a fulminant onset of massive laryngeal swelling. After securing the airway by tracheostomy, an organic foreign body (a fragment of the patient's own teeth) was successfully removed by direct laryngoscopy under general anesthesia.
CASE REPORT
A 56-year-old male was transferred from an external hospital, demonstrating sudden onset of massive laryngeal swelling, leading to a critical obstruction of the upper airway. The patient had a history of diabetes type II, arterial hypertension, reflux esophagitis as well as coronary heart disease with stent implantation one year ago (July 2014). Preoperatively, he had been taking the following medicines: Metoprolol 47.5 mg 1-0-1, Simvastatin 40 mg 0-0-1, Acetylsalicylic Acid 100 mg 1-0-0, Clopidogrel 75 mg 1-0-0, Phenprocoumon 3 mg, glimepiride 1 mg 0-1-0, Metformin 1000 mg 1-0-1, and Pantoprazol 40 mg 1-0-0. The initial treatment consisted of the intravenous administration of Prednisolone (Solu-Decortin?H) in a cumulative dose of 350 mg, Ranitidine 50 mg/5 mL and Dimetinden 4 mg/mL, but this was not sufficient to improve the patient's condition. And after transferring the patient to our clinic, the patient's condition worsened, resulting in a life threatening situation with a dramatic loss of oxygen saturation (<70%) and subsequent fainting. In order to save the patient's life a coniotomy was immediately performed, after which a stable respiratory situation was established, followed by a tracheostomy. Due to the massive mucosal swelling the presence of a foreign body or other cause could not be initially identif i ed during the endoscopy. Postoperatively the patient was monitored in an intensive care unit before being transferred back to our ENT department with stable vital parameters and without neurological def i cits. After one week the mucosal swelling decreased slowly and the computed tomography with radiocontrast (CT) scan of the head and neck displayed a hyperdense structure located in the epiglottis (Figure 1). Under general anesthesia a direct laryngoscopy was performed documenting a swollen epiglottis. Using blakesley forceps, a biopsy was performed resulting in emission of pus. We made an incision and drainage of the abscess andretrieved an organic structure. The foreign body measured 1 mm × 3 mm and could be part of the patient's tooth (Figure 1). One week postoperatively the patient completely recovered with a significant decrease of the laryngeal swelling. The tracheostomy was closed successfully, and we discharged the patient in good condition. The histological examination of the foreign body revealed a calcif i ed organic tissue e.g. part of the patient's tooth.
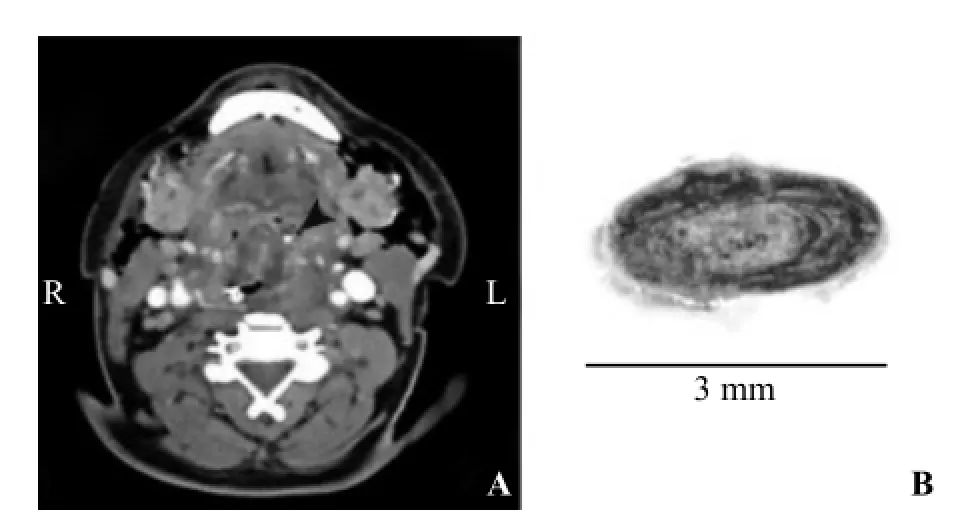
Figure 1. Organic foreign body located in the laryngeal mucosa. A: Axial computed tomography (CT) scan with radiocontrast of the head and neck displaying a hyperdense structure in the epiglottis (black arrow). B: Removed foreign body after fixation and paraffin embedding showing a calcif i ed organic body.
DISCUSSION
Various foreign bodies in the laryngeal mucosa can lead to a life threatening event. In adults, dental material can be found to cause massive swelling in the larynx.[4]The level and the degree of obstruction as well as the size and shape of the foreign body determine the patients' symptoms and prognosis. Coughing, choking, gagging, hoarseness, inspiratory stridor, cyanosis and decreased oxygen saturation may be common early signs of a laryngeal swelling.[5]
We report an unusual case of a massive sudden onset of laryngeal edema due to a small epiglottic foreign body presumably a dislocated part of the patient's tooth leading to a life threatening event with a dramatic loss of oxygen saturation. After stabilizing the patient's airway and starting a calculated antibiotic therapy the mucosal edema persisted. The computed tomography (CT) scan with radiocontrast of the head and neck displayed a hyperdense structure located in the epiglottis. Under general anesthesia the delayed arising epiglottic abscess was incised so the organic foreign body could be removed. In the histological preparation the structure was described as a calcified organic body. Thus we assume the removed foreign body could be a dislocated part of the patient's tooth.
CONCLUSION
This case highlights that even if no typical medical history of inhaling a foreign body is shown, parts of patients' teeth can lead to a life threatening laryngeal edema. Even small foreign bodies measuring just 1 mm × 3 mm can cause a massive laryngeal edema demanding skilled medical staff to rescue the patient's life.
Funding: This research received no specific grant from any funding agency, commercial or not-for-prof i t sectors.
Ethical approval: The authors assert that all procedures contributing to this work comply with the ethical standards of the Helsinki Declaration.
Conflicts of interest: The authors declare there is no competing interest related to the study, authors, other individuals or organizations. Contributors: Droege F proposed the study and wrote the first draft. All authors read and approved the fi nal version of the paper.
REFERENCES
1 Cohen SR, Herbert WI, Lewis GB Jr, Geller KA. Foreign bodies in the airway. Five-year retrospective study with special reference to management. Ann Otol Rhinol Laryngol. 1980;89(5 Pt 1):437–42.
2 Hada MS, Samdhani S, Chadha V, Harshvardhan RS, Prakash M. Larnygeal foreign bodies among adults. J Bronchology Interv Pulmonol. 2015;22(2):145–7.
3 Mahendra SH, Chadda V, Mishra P, Gupta P, Grover M. Unusual metallic foreign bodies in the larynx: two case reports. Indian J Pediatr. 2012;79(8):1100–2.
4 Heggie AAC, Walker J. Traumatic Pharyngeal Displacement of a Full Maxillary Denture: Case Report. J Oral Maxillofac Surg. 1989;47(11):1208–10.
5 Chrcanovic BR, de Souza LN. Tracheotomy for a foreign body in the larynx. Oral Maxillofac Surg. 2009;13(1):55–8.
Received October 9, 2016
Accepted after revision February 6, 2017
10.5847/wjem.j.1920–8642.2017.02.014
Freya Droege, Email: freya.droege@uk-essen.de
 World journal of emergency medicine2017年2期
World journal of emergency medicine2017年2期
- World journal of emergency medicine的其它文章
- Instructions for Authors
- Information for Readers
- World Journal of Emergency Medicine
- Bacteremia or pseudobacteremia? Review of pseudomonas fl uorescens infections
- An unusual case of renal calculi leading to myocardial infarction and cardiogenic shock
- Diverse coagulopathies in a rabbit model with different abdominal injuries