
An unusual cause of simultaneous bilateral spontaneous pneumothorax
2017-02-10 10:46:59MohammedIsmailNizamiNarendraKumarNarahariGogantiKruparaoParamjyothiAshimaSharma
Mohammed Ismail Nizami, Narendra Kumar Narahari, Goganti Kruparao Paramjyothi, Ashima Sharma
1Department of Emergency Medicine, Nizam's Institute of Medical Sciences, Hyderabad 500082, Telangana, India
2Department of Respiratory Medicine, Nizam's Institute of Medical Sciences, Hyderabad 500082, Telangana, India
An unusual cause of simultaneous bilateral spontaneous pneumothorax
Mohammed Ismail Nizami1, Narendra Kumar Narahari2, Goganti Kruparao Paramjyothi2, Ashima Sharma1
1Department of Emergency Medicine, Nizam's Institute of Medical Sciences, Hyderabad 500082, Telangana, India
2Department of Respiratory Medicine, Nizam's Institute of Medical Sciences, Hyderabad 500082, Telangana, India
INTRODUCTION
Scrub typhus, a tropical febrile vector borne disease also known as "Tsutsugamushi disease", is caused by Orientia tsutsugamushi, a gram negative obligate intracellular slow growing bacteria. The infection is transmitted by the bite of larval stage (chiggers) mites belonging to the family Trombiculidae. The disease is transmitted from larval stage mites to rats, where humans are an accidental host. The name scrub typhus is derived from the prevalence of the mites in areas of heavy scrub vegetation. Here we report a case of a young man with primary ciliary dyskinesia presenting with bilateral pneumothorax following Scrub typhus infection.
CASE
A 32-year-old male farmer was brought to emergency room (ER) in severe respiratory distress and hypotension. He had a history of fever with chills of one week duration. He developed cough and sudden worsening of breathlessness two days before he was referred to our hospital. On examination, he was febrile with a body temperature of 102 ℉, pulse rate of 120/minute, respiratory rate of 30/minute and diminished bilateral breath sounds. His blood pressure was 80/60 mmHg and oxygen saturation was 86%. A chest radiograph was ordered which revealed bilateral pneumothoraces with dextrocardia. An urgent right sided tube thoracostomy was done in the ER (Figure 1). The patient was moved to the ICU where he was intubated for respiratory distress and connected to a mechanical ventilator followed by left sided tube thoracostomy. Complete blood count (CBC) revealed a white cell count of 14 500/mm3, serum creatinine of 1.3 mg/dL, platelet count of 130 000 and elevated liver enzymes. In view of seasonal endemicity of Scrub typhus, Weil Felix test was done which showed positive titres (OX 19 – 1:160 and OXK– 1:320). Screening by 2D Echo revealed dextrocardia with normal bi-ventricular function. CT scan of the chest showed bilateral basal interstitial thickening and bronchiectatic changes in the right middle lobe (Figure 2). Bilateral pneumothorax was confirmed apart from the incidental finding of situs inversus totalis (Figure 3). The patient was started on intravenous doxycycline 100 mg twice daily. The blood cultures were sterile after 72 hours of incubation, however the ET secretions grew Acinetobacter spp. during the ICU stay. Colistin injections were started as per the antibiotic sensitivity pattern. The condition improved clinically and pneumothorax resolved following which the patient wasextubated and the ICD tubes removed. The total duration of the hospital stay was 12 days following which the patient was discharged in a healthy stable state. A detailed past history revealed infertility, with semen analysis showing oligospermia and 100% immotile sperms. He also had a history of recurrent upper respiratory tract infections since childhood.

Figure 1 Chest radiograph showing bilateral pneumothorax (arrows) with right sided chest drain in-situ and dextrocardia.
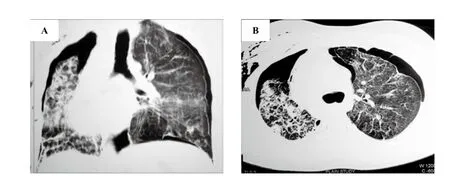
Figure 2. Non contrast CT scan of the chest in coronal (A) and axial (B) sections showing bilateral interstitial thickening and bronchiectatic changes predominantly in the right lung.
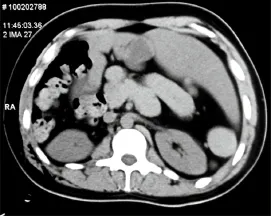
Figure 3. Abdominal section of the CT scan conf rming situs inversus totalis.
DISCUSSION
Simultaneous bilateral spontaneous pneumothorax is an extremely rare clinical condition representing approximately 1% of all cases of spontaneous pneumothorax.[1]The common associations include sarcomas of various origins, histiocytosis X, lymphomas, primary and metastatic lung malignancies, interstitial lung diseases, and infections.[2]Our patient had scrub typhus infection with pulmonary complications like interstitial pneumonitis with acute respiratory distresssyndrome (ARDS) and simultaneous bilateral spontaneous pneumothorax (SBSP). Scrub typhus is widespread across the world, extending from Japan to Australia and from India to Pacific. It has recently been described in India from areas where it was previously unreported.[3]Though the disease is traditionally considered as rural, it is also well described in urban areas. An estimated one billion people are at risk for scrub typhus and one million cases occur annually. Weil-Felix test, although not very sensitive, is considered as a useful tool in the diagnosis of scrub typhus when interpreted in the appropriate clinical context. A single titre of 1:320 (or more) or four fold rise in titre starting from 1:50 is considered positive.[4]The clinical symptoms are fever, headache, malaise, rash and lymphadenopathy which are commonly seen in other acute febrile illnesses. The pathognomonic clinical sign is "eschar" (cigarette burn like appearance) which is a skin lesion at the site of mite bite, which was however not seen in our case. The severity of illness varies from mild to multi organ involvement causing high mortality.[5,6]Scrub typhus involves multiple organs, histologically characterized by microangiopathies. Pulmonary manifestations include varying degrees of interstitial pneumonitis progressing to acute respiratory distress syndrome, consolidation, pulmonary oedema, focal atelectasis, reticulonodular opacities, bronchial wall thickening, centrilobular nodules and hilar adenopathy. Scrub typhus is a potentially lethal but treatable condition and is associated with life threatening complications like pneumonitis and ARDS due to delayed diagnosis.[7]
Primary ciliary dyskinesia is a rare autosomal recessive disease which affects ~1:20 000 individuals.[8]It occurs as a result of a congenital defect in motile cilia covering the respiratory epithelium, leading to impaired mucociliary clearance. Mutations in more than 30 different genes have been attributed to primary ciliary dyskinesia (PCD).[9]The association of pneumothorax in PCD is unusual. Simpleneedle aspiration may be attempted; however bilateral tube thoracostomy is the preferred modality of management in view of severely compromised lung function. Chemical pleurodesis or video assisted thoracoscopic surgery (VATS) may be offered in cases of recurrence. Pneumonitis and ARDS are the most commonly reported complications of scrub typhus, however bilateral pneumothorax has never been reported previously. Rupture of the apical blebs secondary to scrub typhus infection in an underlying diseased lung could possibly explain the etiology of pneumothorax. The occurrence of two infrequent conditions in our patient was a rare co-incidence.
CONCLUSION
This case signif es the importance of early diagnosis and prompt intervention in cases of simultaneous bilateral spontaneous pneumothoraces. Although the initial radiographic picture was confusing in view of a simultaneous dextrocardia, the decision of decompressing the thoracic cavities was life saving in this case.
Funding:None.
Ethical approval:Not needed.
Conflicts of interest:The authors declare there is no competing interest related to the study, authors, other individuals or organizations.
Contributors:Nizami MI proposed the study and wrote the f rst draft. All authors read and approved the f nal version of the paper.
REFERENCES
1 Lee SC, Cheng YL, Huang CW, Tzac C, Hsu HH, Chang H. Simultaneous bilateral primary spontaneous pneumothorax. Respirology. 2008;13(1):145–8.
2 Sayar A, Turna A, Metin M, Kü?ükya?ci N, Solak O, Gürses A. Simultaneous bilateral spontaneous pneumothorax report of 12 cases and review of the literature. Acta Chir Belg. 2004;104(5):572–6.
3 Sharma PK, Ramakrishnan R, Hutin YJ, Barui AK, Manickam P, Kakkar M, et al. Scrub typhus in Darjeeling, India: opportunities for simple, practical prevention measures. Trans R Soc Trop Med Hyg. 2009;103(11):1153–8.
4 Mahajan SK, Kashyap R, Kanga A, Sharma V, Prasher BS, Pal LS. Relevance of Weil-Felix test in diagnosis of scrub typhus in India. J Assoc Physicians India. 2006;54:619–21.
5 Varghese GM, Janardhanan J, Trowbridge P, Peter JV, Prakash JA, Sathyendra S, et al. Scrub typhus in South India: clinical and laboratory manifestations, genetic variability, and outcome. Int J Infect Dis. 2013;17(11):e981–7.
6 Kim D, Kim SW, Choi SH, Yun NR. Clinical and laboratory findings associated with severe scrub typhus. BMC Infect Dis. 2010;10:108.
7 Tsay RW, Chang FY. Acute respiratory distress syndrome in scrub typhus. QJM. 2002;95(2):126–8.
8 Knowles MR, Daniels LA, Davis SD, Zariwala MA, Leigh MW. Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease. Am J Respir Crit Care Med. 2013;188(8):913–22.
9 Kurkowiak M, Zi?tkiewicz E, Witt M. Recent advances in primary ciliary dyskinesia genetics. J Med Genet. 2015;52(1):1–9.
Received April 28, 2016
Accepted after revision September 20, 2016
Mohammed Ismail Nizami, Email: ismail_nizami@rediffmail.com
World J Emerg Med 2017;8(1):74–76
10.5847/wjem.j.1920–8642.2017.01.015
 World journal of emergency medicine2017年1期
World journal of emergency medicine2017年1期
- World journal of emergency medicine的其它文章
- Information for Readers
- World Journal of Emergency Medicine
- Instructions for Authors
- An unusual emergency department case: ruptured ectopic pregnancy presenting as chest pain
- Vasospastic myocardial infarction: An even rarer occurrence of a rare entity
- Toxoplasma encephalitis and AIDS in a patient with seizure and altered mental status: A case report