
Recovery of corticospinal tract injured by traumatic axonal injury at the subcortical white matter: a case report
2016-12-01 12:46:49SungHoJang,SeongHoKim,WooHyukJang
中國神經(jīng)再生研究(英文版) 2016年9期
IMAGING IN NEURAL REGENERATION
Recovery of corticospinal tract injured by traumatic axonal injury at the subcortical white matter: a case report
The corticospinal tract (CST) is a major neural tract for motor function in the human brain. In addition, CST is mainly concerned with execution of movement of the hand (Jang, 2014). However, few studies are reported on the mechanism underlying CST recovery after traumatic brain injury (Seo and Jang, 2015). In this study, we report on a case that showed recovery of an injured CST by traumatic axonal injury (TAI) at subcortical white matter, as detected on follow-up diffusion tensor tractography (DTT).
A 54-year-old male patient who had suffered head trauma after being hit by a bus at a crosswalk as a pedestrian underwent conservative management for an intracerebral hematoma in the right frontotemporal lobes at the department of neurosurgery in a university hospital (Figure 1A). The patient lost consciousness for approximately 30 minutes and experienced post-traumatic amnesia for 2 weeks from the time of the accident. He was transferred to the rehabilitation department of another university hospital for rehabilitation at 2 weeks after onset. Although he presented with quadriparesis, the left finger extensor showed more severe weakness than the right finger extensor (Medical Research Council [right/left]: 4/3; 0: no contraction, 1: palpable contraction, but no visible movement, 2: movement without gravity, 3: movement against gravity, 4: movement against a resistance lower than the resistance overcome by the healthy side, 5: movement against a resistance equal to the maximum resistance overcome by the healthy side) (Council, 1976). The grip strength of the hands was evaluated using a dynamometer (Kim et al., 1994). The average scores across three trials were 17/13 kg [right/left]. The Purdue pegboard scores which were the average peg counts across three trials during 30 seconds, were 6/4 [right/left] (Kim et al., 1994). Higher score indicates much stronger muscle strength or hand function in all tests. For about 9.5 months from 2 weeks to 11 months after onset, the patient underwent comprehensive rehabilitative management in the university hospital and a local rehabilitation hospital. Until 11 months after onset, quadriparesis had improved to a nearly normal state as follows: in particular, the left weakness was more improved than the right weakness: finger extensors (Medical Research Council: 5/5), the grip strength of the hands was 34/30 kg, and the Purdue pegboard scores were 14/13.
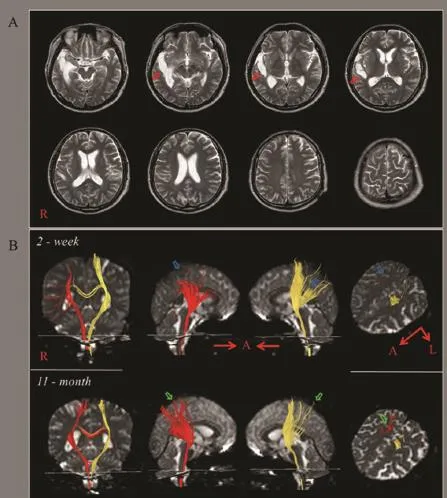
Figure 1 Brain magnetic resonance (MRI) and diffusion tensor tractography (DTT) images in a patient with traumatic axonal injury at the subcortical white matter.
Diffusion tensor imaging (DTI) data were acquired twice (2 weeks, and 11 months after onset) using a 6-channel head coil on a 1.5 T Philips GyroscanIntera (Philips, Ltd, Best, the Netherlands) with single-shot echo-planar imaging. For each of the 32 non-collinear diffusion sensitizing gradients, we acquired 70 contiguous slices parallel to the anterior commissure-posterior commissure line. Imaging parameterswere as follows: acquisition matrix = 96 × 96, reconstructed matrix = 192 × 192 matrix, field of view = 240 × 240 mm2, repetition time = 10,398 ms, echo time = 72 ms, parallel imaging reduction factor (SENSE factor) = 2, EPI factor = 59 and b = 1,000 s/mm2, NEX = 1, and a slice thickness of 2.5 mm.
Fiber tracking was performed using the fiber assignment continuous tracking algorithm implemented within the DTI task card software (Philips Extended MR Workspace 2.6.3). Each of the DTI replications was intra-registered to the baseline “b0” images to correct for residual eddy-current image distortions and head motion effect, using a diffusion registration package (Philips Medical Systems, the Netherland). The CSTs were determined by selection of fibers passing through two regions of interest at the upper and lower pons on the axial image of the colour map (portion of anterior blue colour) (fractional anisotropy-threshold of > 0.2, direction threshold of < 40°) (Kunimatsu et al., 2004). Diffusion tensor tractography (DTT) is derived from fiber tracking of DTI, and it is able to visualize the architecture and integrity of the CST in three dimensions. On 2-week DTT, the majority of the right CST fibers showed complete discontinuation at the subcortical white matter except for a few fibers connected to the cerebral cortex. By contrast, the left CST showed partial tearing at the subcortical white matter. On 11-month DTT, the majority of the discontinued right CST fibers were elongated to the right cerebral cortex and recovery of some fibers from the left torn CST was observed (Figure 1B).
In this patient, we followed up the changes of the CST along with the motor recovery until 11 months after onset, using DTT. On 2-week DTT, the right CST showed more severe injury than the left CST at the subcortical white matter: the right CST showed almost complete discontinuation, and the left CST showed partial tearing. We believe that the injuries of both CSTs in this patient were caused by traumatic axonal injury (TAI) because the conventional brain magnetic resonance imaging (MRI) of the patient did not show any abnormality in both subcortical white matter which showed discontinuation or tearing on DTT (Seo and Jang, 2015). It appeared that these DTT findings coincided with the characteristics of quadriparesis in which the left weakness was more severe than the right weakness (Jang, 2014). On 11-month DTT, the right discontinued CST showed significant recovery in which the majority of the discontinued CST fibers, were recovered to the cortex level, although recovery of some fibers from the left torn CST was observed. These DTT findings appeared to also be compatible with the recovery characteristics of quadriparesis: the left weakness better recovered than the right weakness; as a result, the degree of weakness had become almost similar between the two sides at 11 months after onset (Jang, 2014). Although a few studies have demonstrated the recovery of TAI since the introduction of DTI (Skoglund et al., 2008) and many previous studies have reported the recovery of injured CST in other brain pathologies (Hou et al., 2015; Jin et al., 2015; Wang et al., 2015), to the best of our knowledge, this is the first study to demonstrate recovery of a CST injured by TAI at the subcortical white matter, using DTT. However, limitations of DTI should be considered. First, DTI may underestimate the fiber tracts because regions of fiber complexity and crossing cannot fully reflect the underlying fiber architecture. Second, fiber tracking technique is operator-dependent (Yamada et al., 2009).
This work was supported by the National Research Foundation (NRF) of Korea Grant funded by the Korean Government (MSIP) (No. 2015R1A2A2A01004073).
Sung Ho Jang, Seong Ho Kim, Woo Hyuk Jang*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daemyungdong, Namku, Daegu, Republic of Korea (Jang HS, Jang WH)
Department of Neurosurgery, College of Medicine, Yeungnam University, Daemyungdong, Namku, Daegu, Republic of Korea (Kim SH)
*Correspondence to: Woo Hyuk Jang, Ph.D.,
wlqtksek@hanmail.net.
Accepted: 2016-06-20
orcid: 0000-0002-7012-4565 (Woo Hyuk Jang)
How to cite this article: Jang HS, Kim SH, Jang WH (2016) Recovery of corticospinal tract injured by traumatic axonal injury at the subcortical white matter: a case report. Neural Regen Res 11(9):1527-1528.
References
Council MR (1976) Aids to the Examination of the Peripheral Nervous System. London: H.M. Stationery Office.
Hou TT, Yang XY, Xia P, Pan S, Liu J, Qi ZP (2015) Exercise promotes motor functional recovery in rats with corticospinal tract injury: anti-apoptosis mechanism. Neural Regen Res 10:644-650.
Jang SH (2014) The corticospinal tract from the viewpoint of brain rehabilitation. J Rehabil Med 46:193-199.
Jin D, Liu Y, Sun F, Wang X, Liu X, He Z (2015) Restoration of skilled locomotion by sprouting corticospinal axons induced by co-deletion of PTEN and SOCS3. Nat Commun 6:8074.
Kim YT, Kang SY, Kim HS (1994) Hand strength and dextricity evaluation with age. J Korean Acad Rehab Med 18:780-788.
Kunimatsu A, Aoki S, Masutani Y, Abe O, Hayashi N, Mori H, Masumoto T, Ohtomo K (2004) The optimal trackability threshold of fractional anisotropy for diffusion tensor tractography of the corticospinal tract. Magn Reson Med Sci 3:11-17.
Seo JP, Jang SH (2015) Traumatic axonal injury of the corticospinal tract in the subcortical white matter in patients with mild traumatic brain injury. Brain Inj 29:110-114.
Skoglund TS, Nilsson D, Ljungberg M, Jonsson L, Rydenhag B (2008) Long-term follow-up of a patient with traumatic brain injury using diffusion tensor imaging. Acta Radiol 49:98-100.
Wang Z, Reynolds A, Kirry A, Nienhaus C, Blackmore MG (2015) Overexpression of Sox11 promotes corticospinal tract regeneration after spinal injury while interfering with functional recovery. J Neurosci 35:3139-3145.
Yamada K, Sakai K, Akazawa K, Yuen S, Nishimura T (2009) MR tractography: a review of its clinical applications. Magn Reson Med Sci 8:165-174.
10.4103/1673-5374.191230
- 中國神經(jīng)再生研究(英文版)的其它文章
- Galanin and its receptor system promote the repair of injured sciatic nerves in diabetic rats
- Stem Cell Ophthalmology Treatment Study (SCOTS):improvement in serpiginous choroidopathy following autologous bone marrow derived stem cell treatment
- Changes in microtubule-associated protein tau during peripheral nerve injury and regeneration
- Does crossover innervation really affect the clinical outcome? A comparison of outcome between unilateral and bilateral digital nerve repair
- Effects of triptolide on hippocampal microglial cells and astrocytes in the APP/PS1 double transgenic mouse model of Alzheimer's disease
- Can long-term thiamine treatment improve the clinical outcomes of myotonic dystrophy type 1?