
Intestinal obstruction after radical surgery of cervical cancer in a patient with situs inversus
2016-09-14 08:24:22DanSunYuanYingLiuTaoYuZhiHuaZhangShengJunXuYiCao
Traditional Medicine Research 2016年2期
Dan Sun , Yuan-Ying Liu , Tao Yu, Zhi-Hua Zhang, Sheng-Jun Xu,Yi Cao*
Case presentation
A 53-year-old female patient was transferred to our hospital after her suffering abdominalgia for 12 hours.Situs inversus was known to her for decades. She was once diagnosed with cervical cancer and treated by the radical surgery in another hospital ten years ago.
Computed tomography showed incomplete situs inversus (the liver was located mainly in the upper right portion of the abdomen, the stomach was located in the right abdomen and the spleen in the right hypochondrium, the location and shape of the heart were normal), intestinal dilatation and effusion,cholecystolithiasis (one gallstone, above 1cm in diameter) (Figure 1). Chest radiograph showed intestinal obstruction and right diaphragm elevation.Electrocardiogram showed normal (Figure 2).Furthermore, laboratory examination revealed leukocyte, 12.37×109/L; Neutrophil, 10.46×109/L;General bilirubin, direct and indirect bilirubin were all high.

Figure 1 Computed tomography shows a huge liver(a) and incomplete situs inversus (b) with cholecystolithiasis (c) and intestinal obstruction (d).
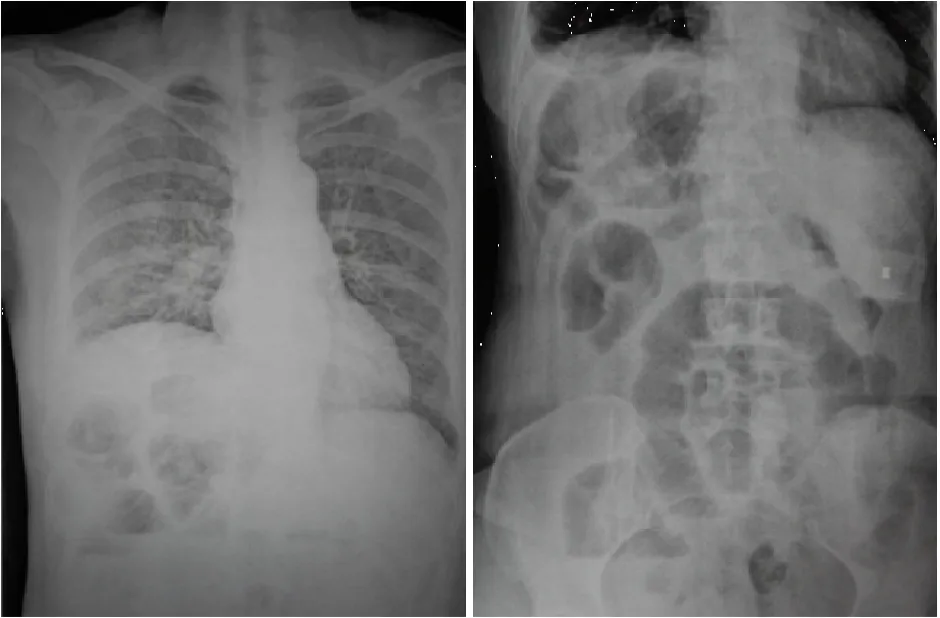
Figure 2 A chest radiograph demonstrates a normal heart, a liver located mainly in the left portion of the abdomen and a right subphrenic gastric bubble in the right subphrenic area.
According to the findings above, laparoscopic cholecystectomy and enterodialysis were performed in turn. The patient was placed supine, the operator stood on the left side of patient, while the assistant stood on the right side. As the same procedure of general laparoscopic cholecystectomy, the surgery was completed successfully. During the operation, a metastasis of pelvic cavity, liver and omentum had not been found. Besides, an adhesion between the small intestine and abdominal wall existed under the old operative incision from the radical surgery of cervical cancer. The patient was discharged on the sixth postoperative day after a conventional care.
Discussion
The incidence of the situs inversus (SI) which is the malposition of internal organs has been reported as approximately 0.02% [1]. Its etiology is unknown, but possibly has a genetic correlation [2]. SI consists of situs inversus totalis and incomplete situs inversus, the latter is infrequent [3] and supposed to be associated with visceral malformations and tumors. Therefore,relevant physical examination and laboratory examination should be conducted for SI patient to estimate the clinical outcome. Park SS et al [4]reported one SI patient had been confirmed an esophageal malignancy in advanced stage after he accepted a subtotal gastrectomy because of unfamiliarity to the anomalies in situs inversus. So it is important to focus on the preoperative evaluation.
There were many reports about SI patient associated with visceral malformations or/and tumors, the case described here also has a history of cervical cancer and a huge liver, although there is no evidence of the association between each other. With the Syndrome differentiation and treatment system, decoctions (e.g.Da-chen-qi decoction) or acupuncture are often given to patients with intestinal obstruction in traditional Chinese medicine (TCM). Acupuncture played a good role in treating functional intestinal obstruction. While,it did not have effects on mechanical intestinal obstruction, especially combined with tumor [5].Because of less surgical complications and better recovery, intestinal obstruction patients choosing surgery in TCM [6]. The report about SI is rare,especially for the case with tumor postoperative intestinal obstruction. The relationship between SI and intestinal obstruction after operation is not clear. On the other hand, these patients rarely receive TCM treatment.
According to literature reviews, there are more than 70 kinds of tumor have been reported to co-exist with SI in the database of NCBI. And the following points are included. 1) top three types of tumor are colorectal carcinoma, lung cancer and kartagener's syndrome(nasal polypus); 2) M-F is about 0.89:1; 3) the cases were mainly distributed in Europe and Asia (Table 1).
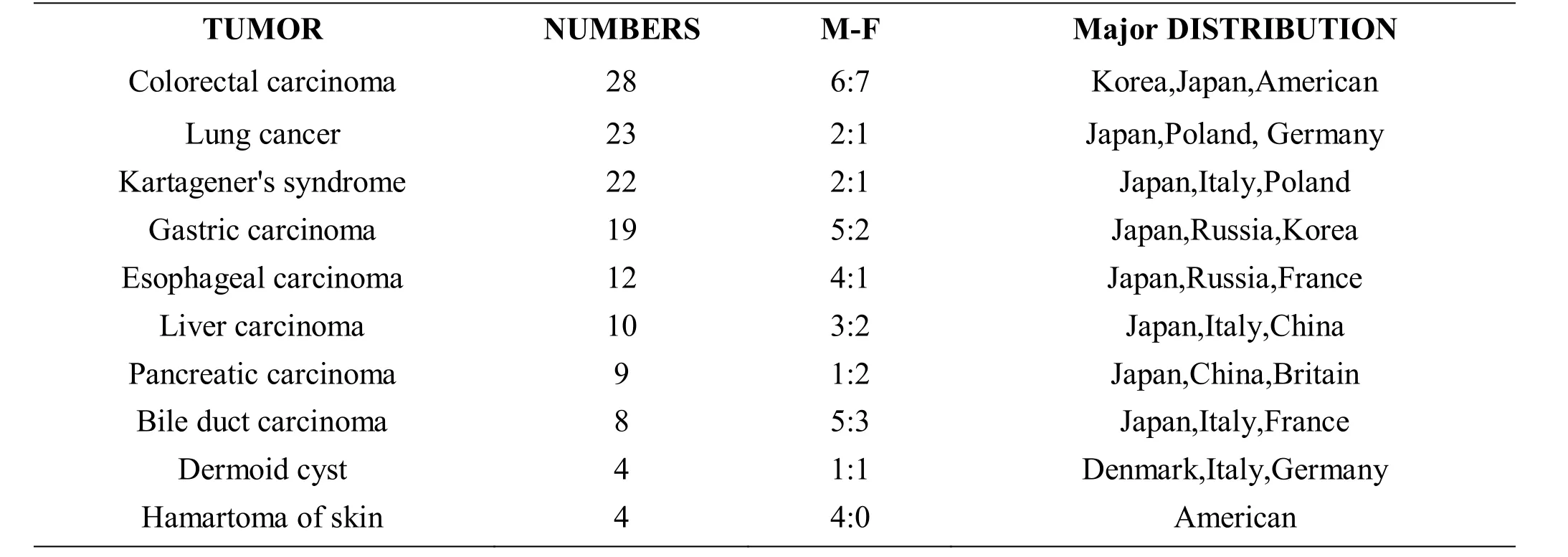
Table 1 Top ten types of tumors coexist with SI reported in NCBI
Discussion
The incidence of the situs inversus (SI) which is the malposition of internal organs has been reported as approximately 0.02% [1]. Its etiology is unknown, but possibly has a genetic correlation [2]. SI consists of situs inversus totalis and incomplete situs inversus, the latter is infrequent [3] and supposed to be associated with visceral malformations and tumors. Therefore,relevant physical examination and laboratory examination should be conducted for SI patient to estimate the clinical outcome. Park SS et al [4]reported one SI patient had been confirmed an esophageal malignancy in advanced stage after he accepted a subtotal gastrectomy because of unfamiliarity to the anomalies in situs inversus. So it is important to focus on the preoperative evaluation.
There were many reports about SI patient associated with visceral malformations or/and tumors, the case described here also has a history of cervical cancer and a huge liver, although there is no evidence of the association between each other. With the Syndrome differentiation and treatment system, decoctions (e.g.Da-chen-qi decoction) or acupuncture are often given to patients with intestinal obstruction in traditional Chinese medicine (TCM). Acupuncture played a good role in treating functional intestinal obstruction. While,it did not have effects on mechanical intestinal obstruction, especially combined with tumor [5].Because of less surgical complications and better recovery, intestinal obstruction patients choosing surgery in TCM [6]. The report about SI is rare,especially for the case with tumor postoperative intestinal obstruction. The relationship between SI and intestinal obstruction after operation is not clear. On the other hand, these patients rarely receive TCM treatment.
According to literature reviews, there are more than 70 kinds of tumor have been reported to co-exist with SI in the database of NCBI. And the following points are included. 1) top three types of tumor are colorectal carcinoma, lung cancer and kartagener's syndrome(nasal polypus); 2) M-F is about 0.89:1; 3) the cases were mainly distributed in Europe and Asia (Table 1).
It is necessary to note the following in the application of laparoscopic cholecystectomy surgery for SI patient. Firstly, as many published literatures reported, operator’s station should be determined by the position of cholecyst. For example, operator should stand between the two legs of the patient to operate incision. Among the cases reported, operator stations were almost adjusted to various degrees in the laparoscopic cholecystectomy surgery for SI patient.Secondly, the procedure was uncomplicated under a skilled operator who is proficient in performing an operation and need to appreciate mirror-image aspects and overcome technique difficulties in handling instruments. Finally, as the discussion above, the SI patient needs careful preoperative evaluation.
Competing interests
The authors declare that they have no competing interests.
Reference
1. Nursal TZ, Baykal A, Iret D, et al. Laparoscopic cholecys -tectomy in a patient with situs inversus totalis. J Laparoendosc Adv Surg Tech A 2001, 11:239-241.
2. Balci S, Bostano?lu S, Altinok G, et al. New syndrome: Three sibs diagnosed prenatally with situs inversus totalis, renal and pancreatic dysplasia, and cysts. Am J Med Genet 2000, 90(3):185–187.
3. Vijayakumar V, Brandt T. Prolonged survival with isolated levocardia and situs inversus. Cleve Clin J Med 1991, 58(3): 243-247.
4. Park SS, Min BW, Kim WB, et al. Double cancer of the stomach and oesophagus with situs ambiguus with polysplenia: The importance of preoperative evaluation. Dig Liver Dis 2005,37(10): 799-802.
5. Bi HJ, He YY, Shu S, et al. Failed acupuncture treatment of small intestinal obstruction after distal gastric cancer: a case report. Acupunct Med 2013,31(3): 334-335.
6. Tan KY, Liu CB, Chen AH, et al. The role of traditional Chinese medicine in colorectal cancer treatment Reply. Tech Coloproctol 2008, 12(1): 6.
 Traditional Medicine Research2016年2期
Traditional Medicine Research2016年2期
- Traditional Medicine Research的其它文章
- The mechanism of electro-acupuncture at Shu and Mu acupoints of lung and large intestine meridians for relieving acute gastrointestinal injury in rats with acute pancreatitis
- The regulation of method of tonifying Qi and activating blood circulation in the related gene expressions after spinal cord injury
- Epigenetic regulations of hematopoietic stem cells ageing and the regulation of traditional Chinese medicine
- Revaluation of Xihuang Pill on tumor treatment: from ancient literatures to modern studies
- Two Proved Recipes for Hemostasis
- Tradition and Modern: Public Debate between Traditional Medicine Researcher and Philosopher