
Distraction osteogenesis for correction of post ankylosis mandibular deformities
2015-12-22 09:15:18AhmedKhanWamiqMusheerFareedParulTandonMuhammadSohailZafar
Ahmed Khan,Wamiq Musheer Fareed,Parul Tandon,Muhammad Sohail Zafar,?
1BabuBanarsi Das College of Dental Sciences,Lucknow 226028,India;
2College of Dentistry,Taibah University,Al Madinah Al Munawwarah43353,Saudi Arabia.
Distraction osteogenesis for correction of post ankylosis mandibular deformities
Ahmed Khan1,Wamiq Musheer Fareed2,Parul Tandon1,Muhammad Sohail Zafar2,?
1BabuBanarsi Das College of Dental Sciences,Lucknow 226028,India;
2College of Dentistry,Taibah University,Al Madinah Al Munawwarah43353,Saudi Arabia.
Temporomandibular joint ankylosis,a debilitating disease mainly affecting children,is characterized by progressive restriction of mouth opening and maxilla-mandibular developmental deformities.Craniofacial distraction osteogenesis has been developed as a standard surgical strategy for rectification of craniofacial deformities.The purpose of this study was to assess mono-planar distraction devices for the correction of various mandibular asymmetries in patients with unilateral temporomandibular joint ankylosis who developed restricted mouth opening and mandibular retrognathia.All patients were treated using one-stage distraction osteogenesis followed by temporalis fascia interpositional arthroplasty under general anesthesia.A significant increase in mandibular ramus and base length was observed.Although an increase in anterior lower facial height was observed,it was not significant statistically. A decrease in posterior lower facial height and corpus was observed.Oblique distraction with angular osteotomy allowed lengthening of both the ramus and corpus,yielding satisfactory results and hence eliminating the need of secondary surgery.In conclusion,univector internal distractors are effective for correction of multi-planar mandibular deficiencies by optimizing its placement through meticulous planning.
distraction osteogenesis,temporomandibular joint disorders,mandibular asymmetry,atrophy
Introduction
Temporomandibular joint(TMJ)ankylosis is a prevalent cause of mandibular deformity and distortion in children due to trauma or infection[1].The major goals towards the treatment of TMJ ankylosis are to establish movement and functioning of the jaws,avoid relapse or setback and achieve normal growth,occlusion and deformity correction[2].Untreated TMJ ankylosis in children may result in a significant functional and aesthetic adverse consequences including facial asymmetry.It can progressively worsen due to hypomobility and abnormal muscle functions.The longer the duration of hypomobility,the more severe muscular atrophy and facial asymmetry will be.The short ramus condyle unit also restricts mid-face growth to a varying degree.One of the major complications of TMJ ankylosis is mandibular retrognathia,giving rise to bird face deformity.It likewise causes inadequate delicate soft tissue of the lower third of the face and at the neck,deficiency of the neck angle and abbreviated suprahyoid muscles.While TMJ ankylosis essentially requires surgical arthrectomy,correction of growth lag can either be achieved through conventional orthognathic procedures,distraction osteogenesis or both.
The treatment of such defects using the arthrectomy technique results in mouth opening,but deprives the patient of growth lag compensation and enhanced psychological development owing to compromised esthetics and function.Limitations of the conventional osteotomy procedures for correction of deformity are surgical neurosensory complication,condylar resorption,postoperative relapse,bone graft failure,limitation of advancement,bone graft donor site morbidity, and bone formation by secondary healing[3].Although bone grafting is a compelling device,it conveys the danger of benefactor site and resorption of the grafted bone along with donor site pain.Furthermore,bone grafting for augmentation requires adquate volume of soft tissue to prevent surgical site infection by obtaining water tight tension free closure.Moreover,the skeletal relapse may occur as a result of ductile/tensile stresses generated by the muscles and soft tissue following bone lengthening techniques.
Distraction osteogenesis can be an alternative technique for handling such defects.It can be defined as a procedure of new bone formation between the surfaces of bone portions or fragments that are gradually differentiated in response to incremental traction[4]. Distraction osteogenesis has also drawn attention in the treatment of extreme mandibular retrognathia. Inherent aberrances are associated with severe mandibular retrognathia or micrognathia including craniofacial syndromes such as hemifacial microsomia, Treacher-Collins syndrome,Pierre-Robin syndrome, and Nager syndrome[5].
The first bone distraction procedure was performed for the treatment of reduced/shortened femur bone and reported by a British scientist Codivilla[6].However, due to a high disorganized rate,the distraction osteogenesis technique did not draw much attention until 1954 when Ilizarov had extensive research on this technique and practical applications for the lower extremity showed encouraging clinical outcomes[7]. Distraction osteogenesis has been used for the treatment of long bones for many years until Synder[8]utilized external fixator to stretch and lengthen a canine mandible.Further extensive work by McCarthy in 1990s reported distraction osteogenesis in the mandible of patients with one-sided craniofacial microsomia and related disorders[9-10].
Mandibular lengthening acquired by gradual distraction results in expansion of mandibular bony tissues as well as additionally relative coordination,congruence modification of muscles and the surrounding soft tissues.The forces produced and transformed by the distractor on the mandible are alike to physiological forces throughout the course of mandibular development[11].These factors combine to achieve a better postoperative correction.The objective of this study was to assess the role of mono-planar distraction devices in correction of various post ankylosis mandibular deformities.
Patients and Methods
Patients
We selected TMJ ankylosis patients who had restricted mouth opening and mandibular retrognathia.All patients were treated using distraction osteogenesis followed by temporalis fascia interpositional arthroplasty under general anesthesia.Eight adult patients fulfilling the inclusion criteria(restricted mouth opening along with mandibular retrognathia clinically and radiographically diagnosed as unilateral TMJ ankylosis,irrespective of socioeconomic status)were included in this study. Patients suffering from chronic and debilitating diseases (diabetes mellitus,pulmonary tuberculosis,etc)were excluded from this study.
Each patient was educated about the surgical procedure and an informed consent was obtained for the surgical treatment and for participation in this study.The study protocol was approved by the research ethics committee at BabuBanarsi Das College of Dental Sciences,Lucknow.To determine the discrepancies of the body and ramus of the mandible,a detailed preoperative radiographic analysis for each patient was performed to trace cephalometric landmarks on lateral and posteroanterior cephalogram.For this purpose, quadrilateral and Steiner's analysis were performed. The quadrilateral analysis demonstrated a ratio of 1:1 between maxillary and mandibular base length for a balanced facial pattern.In the case of normal physiological growth of facial structures,the maxillary base length was equal to the mandibular base length.Both the affected and non-affected sides of the mandible were traced to focus on the ramus height bilaterally, and ramus height proportions were calculated accordingly.
Surgical procedure
The surgical protocol involved one-stage distraction osteogenesis followed by temporalis fascia interpositional arthroplasty post consolidation using the extraoral approach(Risdon incision).A custom fabricated internal distractor was placed after corticotomy of both the buccal and lingual cortex.Osteotomy at the mandibular angle with oblique placement of the internal distractor was done in 5 patients based on treatment planning by Wolfgang Losken[4].In the remaining 3 patients,ramus osteotomy was performed to achieve
the desired ramus height followed by consolidation body osteotomy for corpus lengthening.Distraction was started on the 5th-7thday postoperatively and continued at the rate of 0.5 mm 12 hourly till completion of the calculated deficiency and was left to consolidate for a period of 8-10 weeks.The results were then evaluated and compared using preoperative and postoperative cephalograms.Statistical analysis was performed using the IBM SPSS V19(IBM Corp.,Armonk,NY, USA)and Wilcoxon Signed Rank test(2-tailed)of significance was applied.
Results
As per inclusion criteria,all the patients exhibited deviation of the mandible as well as non-palpable or diminished TMJ movements during preoperative examination.Mouth opening ranged from 2 to 10 mm(mean value of 6.25 mm± 3.24 mm),which was lower than normal physiological mouth opening. For the purpose of comparison,preoperative measurements were recorded(Table 1)for maxillary and mandibular basal lengths and their mutual skeletal relationships.The preoperative measurements of skeletal tissues were suggestive of compromised mandibular growth requiring therapeutic intervention.
Distraction devices were applied in each case and activated after every 12 hour(1 mm/day).The mean latency and consolidation periods and total distraction obtained are shown inTable 2.The applied distraction resulted in a significant increase in mandibular base length during the period(P=0.017).Although an increase in anterior lower facial height was observed, it was not significant statistically(P=0.180).A decrease in posterior lower facial height and corpus was observed,but it was significant only for change in corpus(P=0.018).A significant increase in mandibularbase length was observed during the period(P=0.017). Although an increase in anterior lower facial height was observed,it was not significant statistically (P=0.180).A decrease in posterior lower facial height and corpus was observed,but it was significant only for change in corpus(Table 3).
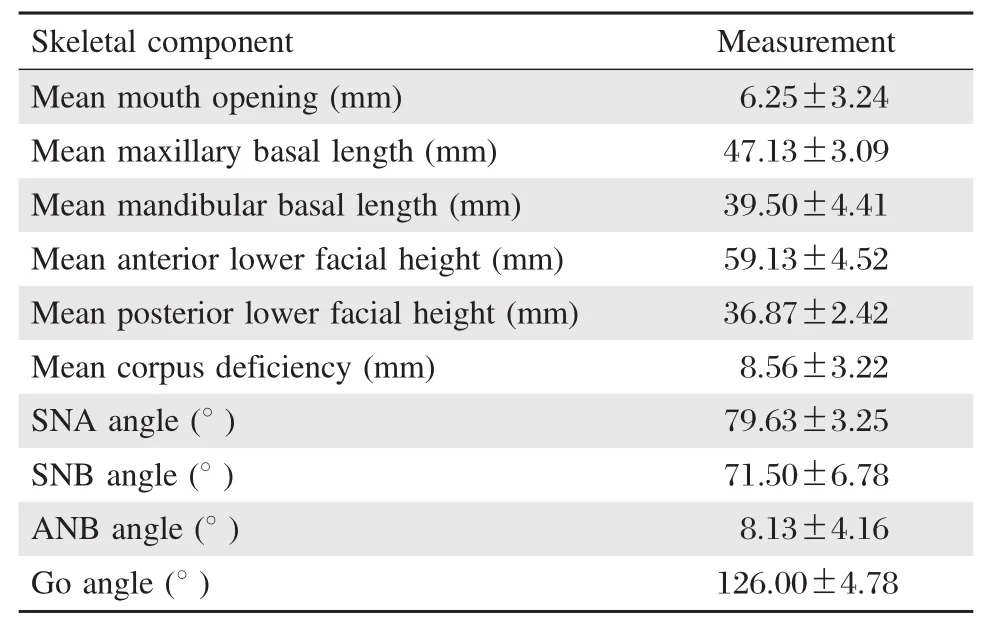
Table 1Preoperative measurements for skeletal tissue and their relationships
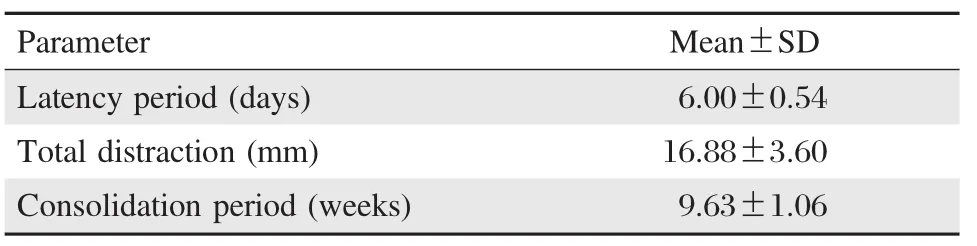
Table 2Distraction osteogenesis parameters
A remarkable growth of the mandible bone was observed at the first follow up in response to the distracter devices;however,no change was recorded in any of the linear parameters between the first and second follow up intervals.Similar results were observed for vertical mandibular growth.A significant change in the vertical height of mandible was observed with achievement of a mean value of 1.00 mm at the first follow up.
Discussion
To overcome developmental jaw defects,excessive advancement of the mandible(more than 7 mm)is challenging and becomes increasingly more unstable with traditional osteotomies[12].The masseter and pterygoid muscles in combination with other extended delicate tissues assume a part in the relapse connected with the incremental protracting of the ramus during orthognathic intervention[13-14].In addition,if the advancement is more than 10 mm with conventional osteotomies,the inferior alveolar nerve would be stretched resulting in neurosensory deficit.Such types of complications can be avoided while using distraction osteogenesis hence becomes the treatment of choice for mandibular hypoplasia[15].Moreover,the degree of advancement that can be achieved by distraction osteogenesis is much better(sometime more than 20-22 mms)than that obtained by conventional osteotomies[16].In the current study,the diversion was from 12 to 23 mm and none of the patients reported neurosensory deficits of the inferior alveolar nerve.
In case of conventional mandibular advancement using osteotomies and bone grafts in similar patients, the muscles and the tight skin envelop results in compromised correction and aesthetics.Whereas using distraction osteogenesis,all the tissues from skeleton to skin are lengthened at the same time with optimum aesthetic and useful outcomes.In distraction osteogenesis, the extension of the muscle occurs all around the muscles along with the site of osteotomy[17].Most importantly,thedirection,course and amount of bone lengthening might be controlled alongside lengthening of soft tissues[18]. Throughout distraction osteogenesis,animated histogenesis happens in distinctive tissues including the gingiva,blood vessels,ligaments,cartilage,muscle and nerve[19-20].The debate does not in any way undermine the integrity of conventional orthognathic procedures,but only highlights its limitation towards patient selection.Certain cases requiring mild to moderate skeletal corrections can be best managed using orthognathic surgical approaches that offer immediate correction with minimal hospitalization.

Table 3Changes in linear variables at follow up(post distraction)compared to baseline
Timing of distraction has incited significant debate amongst various authors.Lopez and Dogliotti[11]exhorted that arthroplasty ought to be carried out prior to mandibular distraction osteogenesis.However,other school of thought says that it may prompt the condyles moving upward and backward within the glenoid fossa during distraction[21-22].The measurement of displacement is associated with mandibular lengthening, adverse outcomes during distraction may happen due to eccentric vector administration,active and dynamic mouth opening after ankylosis release[23-24].In contrast, mandibular distraction osteogenesis procedures help to avoid rotary as well as upward motions of the condylar segment throughout the distraction course[18].Kwon et al.reported that this may result in unstable occlusion and distraction during arthroplasty and has the likelihood of mobility of the distraction site throughout rumination or functional exercise based recuperation (physiotherapy),consequently expanding the likelihood of pseudo-arthrosis at the distraction site[24].It is difficult to manipulate the distraction vectors using‘‘molding to regenerate’’and the application of maxillo-mandibular elastics during dynamic distraction phase to close an open bite.Moreover,it is unreliable to handle the occlusal plane in instantaneous and simultaneous distraction and arthroplasty as a result of an active physical treatment needed for avoidance of re-ankylosis;in addition,it is difficult to anticipate the mandibular position after condylectomy[25].
Gonzalez[12]suggested that for cases of TMJ ankylosis,two-stage surgeries should be performed.During the first stage,ramal and corpus lengthening should be achieved,which allows the clinician a predictable mandibular ramus and vertical augmentation and mandibular lengthening and the second stage surgery is planned once the consolidation is completed,which consists of freeing of TMJ ankylosis by arthroplasty. Following this protocol,there is a better control of distraction segments as the immobile joint denoted to the foundation that might move the mandible in the forward direction,instead of the retrogressive direction[23]. This avoids pressure against the new surgically created joint,and allows active physiotherapy after releasing the joint[12].These findings are in with the current study where horizontal and vertical advancement yielded separately to optimum results with enhanced chin prominence.
In two-stage distraction,ramus distraction was done first,assuming that ramus distraction would not only increase the ramus height but also eliminate potential occlusal interferences and would additionally yield certain degree of corpus lengthening.Oblique placement of distractor on the other hand allows lengthening of both ramus and corpus at the same time yielding satisfactory results,and eliminating the need of the second surgery, thus giving an edge over differential vertical and horizontal distraction.However,we observed that instances of hardware failure in our cases were related to oblique distraction especially where more than 12 mm of correction was desired.Hardware related complications were observed in 3 patients in which breakage of distractor was seen.This complication did not influence the final treatment result as in 2 patients the distraction procedure had already been completed to the strategic,calculated endpoint.They were subsequently put on maxillamandibular fixation with acrylic wafer at inter-cuspation in occlusion during the consolidation period.However, in one patient,breakage was seen during the third day of distractor activation,in which the second surgery was performed with re-fixation of new distraction device.
In conclusion,separate horizontal and vertical advancements are required to yield optimal results. Oblique placement of distractor with angular osteotomy allows lengthening of both the ramus and corpus at the same time,yielding satisfactory results and eliminating the need of second surgery,thus giving an edge over differential vertical and horizontal distraction.Univector internal distractor can effectively be used for correction of multiplanar mandibular deficiencies by optimizing its placement through meticulous planning.
[1] Heggie AA.Concepts in the management of temporomandibular ankylosis[J].Ann R Australas Coll Dent Surg, 1996,13:132-135.
[2] Rowe NL.Ankylosis of the temporomandibular joint[J]. J R Coll Surg Edinb,1982,27(2):67-79.
[3] Gc RK,Ramaiha S.Distraction osteogenesis in the management of temporomandibular joint ankylosis;Series of cases[J].Int J Clin Dent Sci,2011,2(1):22-26.
[4] Samchukov ML,Cope JB,Cherkashin AM.Craniofacial distraction osteogenesis[M].1stedition.London:St. Louis,Mosby Inc.2001.
[5] Nanci A.Ten Cate’s oral histology:development,structure and function[M].8thedition.London:St.Louis, Mosby Inc.2012.
[6] Codivilla A.On the means of lengthening,in the lower limbs,the muscles and tissues which are shortened through deformity[J].J Bone Joint Surg,1905,2(4):353-369.
[7] Ilizarov G.A new principle of osteosynthesis,using cross wires and rings.Sb Nauchn Rab Kurgan Obi Nauchn Med Ova,1954:146-160.
[8] Snyder CC,Levine GA,Swasson HM,et al.Mandibular lengthening by gradual distraction:preliminary report[J]. Plast Reconstr Surg,1973,51(5):506-508.
[9] McCarthy JG.The role of distraction osteogenesis in the reconstruction of the mandible in unilateral craniofacial microsomia[J].Clin Plast Surg,1994,21(4):625-631.
[10]McCarthy JG,Schreiber J,Karp N,et al.Lengthening the human mandible by gradual distraction[J].Plast Reconstr Surg,1992,89(1):1-10.
[11]Lo′pez EN,Dogliotti PL.Treatment of temporomandibular joint ankylosis in children:is it necessary to perform mandibular distraction simultaneously?[J].J Craniofac Surg,2004,15(5):879-884.
[12]Gonzalez M,Egbert M,Guerrero CA,et al.Vertical and horizontal mandibular lengthening of the ramus and body[J].Atlas Oral Maxillofac Surg Clin,2008,16(2): 215-236.
[13]Proffit WR,Turvey TA,Phillips C.Orthognathic surgery: A hierarchy of stability[J].Int J Adult Orthodon Orthognath Surg,1996,11(3):191-204.
[14]Swennen G,Schliephake H,Dempf R,et al.Craniofacial distraction osteogenesis:A review of the literature.Part 1: clinical studies[J].Int J Oral Maxillofac Surg, 2001,30(2):89-103.
[15]Posnick JC.Orthognathic surgery for the cleft lip and palate patient[J].Semin Orthod,1996,2(3):205-214.
[16]RileyRW,PowellNB,LiKK,etal.Surgeryandobstructive sleep apnea:long-term clinical outcomes[J].Otolaryngol Head Neck Surg,2000,122(3):415-421.
[17]Sato M,Maruoka Y,Kunimori K,et al.Morphological and immunohistochemical changes in muscle tissue in association with mandibular distraction osteogenesis[J]. J Oral Maxillofac Surg,2007,65(8):1517-1525.
[18]Yoon H,Kim H.Intraoral mandibular distraction osteogenesis in facial asymmetry patients with unilateral temporomandibular joint bony ankylosis[J].Int J Oral Maxillofac Surg,2002,31(5):544-548.
[19]Hawkinson RT.Retrognathia correction by means of an arcing osteotomy in the ascending ramus[J].J Prosthet Dent,1968,20(1):77-86.
[20]Liou EJ,Huang CS.Rapid canine retraction through distraction of the periodontal ligament[J].Am J Orthodont Dentofac Orthoped,1998,114(4):372-382.
[21]Michieli S,Miotti B.Lengthening of mandibular body by gradual surgical-orthodontic distraction[J].J Oral Surg, 1977,35(3):187-192.
[22]Shang H,Xue Y,Liu Y,et al.Modified internal mandibular distraction osteogenesis in the treatment of micrognathia secondary to temporomandibular joint ankylosis: 4-Year follow-up of a case[J].J Craniomaxillofac Surg, 2012,40(4):373-378.
[23]Azumi Y,Sugawara J,Takahashi I,et al.Positional and morphologic changes of the mandibular condyle after mandibular distraction osteogenesis in skeletal class II patients[J].W J Orthodont,2004,5(1):32-39.
[24]Kwon T,Park H,Kim J,et al.Staged surgical treatment for temporomandibular joint ankylosis:intraoral distraction after temporalis muscle flap reconstruction[J].J Oral Maxillofac Surg,2006,64(11):1680-1683.
[25]Nam JS,Lee YG,Kwon TG,et al.Interpositional arthroplasty of temporomandibular joint ankylosis with temporalis myofascial flap[J].J Korean Assoc Oral Maxillofac Surg,2000,26(5):544-549.
?Corresponding author:Muhammad Sohail Zafar,Ph.D,College of Dentistry,Taibah University,P.O.Box 2898,Madinah Al Munawwarah Saudi Arabia.Tel:00966507544691,E-mail:drsohail_78@hotmail. com.
Received 07 May 2014,Revised 29 September 2014,Accepted 24 February 2015,Epub 10 May 2015
R782,Document code:A
The authors reported no conflict of interests.
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年4期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年4期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Class II transactivator(CIITA)mediates transcriptional repression of pdk4gene by interacting with hypermethylated in cancer 1(HIC1)
- TYMSgene 5′-and 3′-untranslated region polymorphisms and risk of non-syndromic cleft lip and palate in an Indian population
- Delorme's operation plus sphincteroplasty for complete rectal prolapse associated with traumatic fecal incontinence
- Impact of crosslinking/riboflavin-UVA-photodynamic inactivation on viability,apoptosis and activation of human keratocytesin vitro
- Co-firing of levator palpebrae and masseter muscles links the masticatory and oculomotor system in humans
- Comparison of dimension reduction-based logistic regression models for case-control genome-wide association study:principal components analysisvs.partial least squares