
Unruptured pregnancy in a noncommunicating rudimentary horn at 37 weeks with a live fetus:a case report
2015-01-10 06:16:33ChenChengWeiweiTangLeiZhangMeiLuoMeihuaHuangXiulingWuGuipingWan
Chen Cheng,Weiwei Tang,Lei Zhang,Mei Luo,Meihua Huang,Xiuling Wu,Guiping Wan
Laboratory of Gynecological Oncology,Jiangsu Province Hospital on Integration of Chinese and Western Medicine Affiliated to Nanjing University of Traditional Chinese Medicine,Nanjing,Jiangsu 210028,China.
Unruptured pregnancy in a noncommunicating rudimentary horn at 37 weeks with a live fetus:a case report
Chen Cheng,Weiwei Tang,Lei Zhang,Mei Luo,Meihua Huang,Xiuling Wu,Guiping Wan?
Laboratory of Gynecological Oncology,Jiangsu Province Hospital on Integration of Chinese and Western Medicine Affiliated to Nanjing University of Traditional Chinese Medicine,Nanjing,Jiangsu 210028,China.
We reportan extremely rare case ofan unruptured non-communicating rudimentary horn full-term pregnancy.A woman who had a uterine malformation was misdiagnosed as uterus didelphys and gave birth to a live,healthy fetus.The correctdiagnosis was notmade untilcesarean section at37 4/7 weeks.The case suggests that women who are pregnantin a rudimentary horn could obtain a full-term delivery and give birth to a live and healthy baby.
unruptured,non-communicating rudimentary horn,full-term delivery
Introduction
Unicornuate uterus with a rudimentary horn is a rare m u¨llerian anomaly which has a high incidence of obstetric complications including ectopic pregnancy in the rudimentary horn.The true prevalence of m u¨llerian duct abnormalities is not well established because the majority of patients are asymptomatic and it is approximately 1:200-1:600 in fertile women. However,rudimentary horn pregnancy occurs in approximately 1 of every 76,000 pregnancies and commonly presents with first-or second-trimester uterine rupture.The unicornuate uterus with a noncommunicating uterine horn is one ofthese conditions. In such cases,only 50%to 55%are symptomatic,and only 8%of rudimentary horn pregnancies are diagnosed before the symptoms appear.Term pregnancies with delivery of a live fetus have been rarely reported in such unusual and life-threatening condition.We report an extremely rare case of a pregnancy in a non-communicating rudimentary uterine horn which reached a full-term delivery,without rupture,to a healthy neonate.
Case report
A 25-year-old woman,gravida 1 para 0,presented at our hospital.According to her reliable dates,she was at a 37 2/7-week that pregnancy.A review of her menstrualhistory revealed her menarche was achieved at thirteen.The patient had a regular menstrualcycle of 30 days and her menstruation was consistently about 7 days duration.A previous ultrasound at early pregnancy revealed a single fetus intrauterine pregnancy with congenital uterine malformation,diagnosed as didelphys.During her pregnancy,the patient was not on regular follow-up.A single,meticulous examination was performed atthe 7thmonth,revealing a single live intrauterine fetus which conformed to her gestationalweeks.Threatened premature delivery did notemerge until34 5/7 weeks.She then received tocolysis upon admission into anotherhospital.Magnesium sulfate was used to inhibituterine contractions in orderto delay delivery until the gestationalage of 37 weeks. Two weeks later,her condition stabilized and she was discharged.In follow-up examinations,her pulse rate and blood pressure were both normaland the fundus ofthe uterus corresponded to the date ofherpregnancy.
Upon admission to ourhospital,she was required to complete the related auxiliary examination.Laboratory examinations and fetalmonitoring were normalexcept thatthe latestultrasound showed thatthe amniotic fluid index was only 7.3 cm and the patient was diagnosed with borderline oligohydramnios and breech presentation.No slight lower abdominal pain,no vaginal bleeding,or no uterine contractions was detected.In order to raise her amniotic fluid levels,fluid replacement therapy was performed immediately.The next day,the results of her examinations showed thather cholic acid was 6.741μg/mL,highly suggestive of intrahepatic cholestasis of pregnancy.The amniotic fluid index returned to normal.Regular contractions were detected in fetalmonitoring.Because her pregnancy was primigravida with breech presentation with suspected intra-hepatic cholestasis of pregnancy and her uterine malformation,vaginal delivery was not feasible.The patient and her family consented to cesarean section delivery.
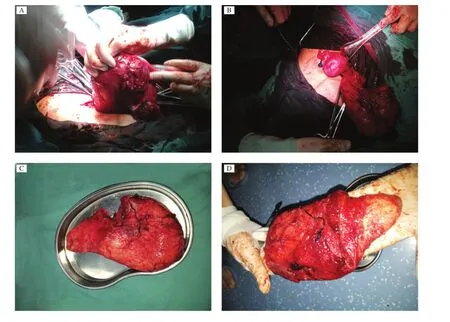
Fig.1 The rudimentary horn of a patient with an unruptured non-communicating rudimentary horn who reached full-term pregnancy and delivered a healthy baby.A:View of the right sided rudimentary horn intra-uterine pack with sterilized gauze before excision. B:Intra-operative photograph showing the normaluterus with the rudimentary horn attached to its right.C:Sectioned rudimentary horn.D:Innerview of the non-communicating rudimentary horn with the cavity.
The nextday,cesarean section was performed and, intraoperatively,a large intactright-sided uterine horn was observed to be the size of a full-term pregnancy, while the leftsided uterine horn increased to the size of two monthsˊpregnancy.The uterine surface was coarse and full of congestive blood vessels.The right-side uterine horn was incised to deliver a fetus of 37 4/7 weeks gestation.The neonate was a live girl weighting 2,550 g,and the Apgar score was normal. The placenta could not be easily stripped,so artificial stripping oftheplacenta wasperformed.Uterine massage was performed in orderto promote uterine contractions;however,intractable bleeding from the placenta bed was uncontrollable and an intra-uterine pack with sterilized gauze was applied(Fig.1A).During this process,the rudimentary horn was identified and excised from the uterus to controlbleeding.There was no communication between the rudimentary horn and the main uterine cavity.The stump wasthen sutured(Fig.1B).A peritoneal lavage wasdone and the abdomen wasclosed.Resection of the rudimentary horn was completed successfully (Fig.1C).Total blood loss was about 1,500 mL and 200 mL fresh frozen blood plasma and 4 units of red blood cellwere transfused followed by 1,200 mL crystalloid and 1,300 mL colloid.
A pregnancy in a non-communicating rudimentary horn was confirmed after the operation(Fig.1D). Pathological and histological findings confirmed a right-sided non-communicating rudimentary horn with cavity.Her postoperative course was uneventful.Her temperature,pulse and blood pressure were allnormal the nextday exceptthatherhemoglobin was 82.0 g/L. An anti-infection treatmentand a blood-tonifying drug were used until she was discharged.As a result of blood loss,she was stillanemic when discharged,with the hemoglobin showing 74.0 g/L,and she required further treatmentfor anemia during follow-up.
Discussion
The unicornuate uterus with a non-communicating rudimentary horn results from the normaldevelopment and maturation ofone ofthe m u¨llerian ducts with concomitant hypoplasia of the contralateral m u¨llerian duct[1].According to the American Fertility Society (AFS),‘‘unicornuate’’uterus m u¨llerian ductanomalies are classified as follows:‘‘classa’’iswith cavity,communicating with the uterus;‘‘class b’’is with cavity, notcommunicating with the uterine;‘‘class c’’is withoutcavity;and‘‘class d’’is withouthorn.
Pregnancy in a non-communicating rudimentary horn is considered to be the result of transperitoneal migration of either the ovum or the zygote from the contralateral side.Previous reports demonstrated that uterine rupture occurred in 80%of rudimentary horn pregnancies and mostpregnancies in these cases ruptured in the second trimester before the 20thweek of gestation[2].Despite early ultrasonography,it is still difficult to make a clear diagnosis of pre-rupture rudimentary horn pregnancy.The preoperative diagnosis is provided in only 22%gynecologic and 29%obstetric cases,so most diagnoses are confirmed only after laparotomy.Few casesare diagnosed in the firsttrimester and most of them are asymptomatic or have a uterine abnormality as described previously.Magnetic resonance imaging hasproven to be a very effective,noninvasive toolforthe diagnosis ofm u¨llerian abnormalities, but this modality is expensive for routine use,except when rudimentary horn pregnancy is suspected either by history or by early suspicious ultrasound examinations.As a result,late or wrong diagnosis resulting in uterine rupture is frequent.
For a precise diagnosis and protectmaternalhealth, routine ultrasonographic diagnosis in the firsttrimester is important[3-5].However,the overall sensitivity of ultrasonography for diagnosing a rudimentary horn or rudimentary horn pregnancy is actually low at early pregnancy,especially when itis used for the differentialdiagnosis of ectopic pregnancy with other uterine malformations,such as uterus biconis,uterus duplex and mediastinum uterus,suggesting that clinicians should pay more attention to pregnancy combined with uterine malformation during routine obstetric examinations,especially,when there isa possibility ofan ectopic pregnancy in a rudimentary horn which is characterized by malpresentation or other complications.When these circumstances occur,some necessary measures mustbe implemented immediately according to symptoms. Termination of pregnancy should also be performed,if necessary,once a rudimentary horn pregnancy is confirmed and the horn excised[6].
The case of rudimentary horn pregnancy presented in this report was misdiagnosed as uterus didelphys priorto the cesarean section.However,severalworthy points should be focused on.Firstly,cases of pregnancy in the rudimentary horn with a full-term delivery have seldom been reported,so far,especially a patient who gave birth to a healthy baby[7].Secondly,during routine obstetric examination,our patienthad none of the typicalmanifestations usually found in rudimentary horn pregnancies.Borderline oligohydramnios and intrahepatic cholestasis ofpregnancy should notbe due to rudimentary horn,while malpresentation mightbe attributed to rudimentary horn because there was less space available forfavorable adaptation ofthe fetalhead in the uterus.Thirdly,although such cases are rare,clinician should be aware of this life-threatening condition and,once itis identified,mandatory life saving proceduressuch as timely laparotomy and immediate removal of the horn should be performed as was done in our case[8-10].Laparoscopic resection is limited to pre-rupture firsttrimestercases and itwas reported to be successful in some cases.Lastbutnotleast,thiscase may shed light on correctdiagnosis and differentialdiagnosis of rudimentary horn pregnancy when this circumstance occurs in the future,in order to effectively reduce the rate of missed diagnosis and misdiagnosis of this condition.
[1]Junqueira B,Allen L,Spitzer R,et al.M u¨llerian duct anomalies and mimics in children and adolescents:correlative intraoperative assessment with clinical imaging. Radiographics 2009;29(4):1085-1103.
[2]Goel P,Saha PK,Mehra R,et al.Unruptured postdated pregnancy with a live fetus in a noncommunicating rudimentary horn.Indian J Med Sci 2007;61(4):23-27.
[3]Arslan T,Bilgi c?E,Sent u¨rk MB,etal.Rudimentary uterine horn pregnancy:a mystery diagnosis.Fertil Steril 2009; 92(6):203.e1-3.
[4]D Reichman,MR Laufer,BK Robinson.Pregnancy outcomes in unicornuate uteri:a review.Fertil Steril 2009; 91(5):1886-1894.
[5]S Chopra,A Keepanasseri,M Rohilla,et al.Obstetric morbidity and the diagnostic dilemma in pregnancy in rudimentary horn:retrospective analysis.Arch Gynecol Obstet 2009;280(6):907-910.
[6]Lennox G,Pantazi S,Keunen J,etal.Minimally invasive surgicalmanagementofa second trimester pregnancy in a rudimentary uterine horn.J Obstet Gynaecol Can 2013; 35(5):468-472.
[7]Patra S,Puri M,Trivedi SS,et al.Unruptured term pregnancy with a live fetus with placenta percreta in a noncommunicating rudimentary horn.Congenit Anom(Kyoto) 2007;47(4):156-157.
[8]Thakur S,Sood A,Sharma C.Ruptures noncommunicating rudimentary horn pregnancy at19 weeks with previous cesarean delivery:a case report.Case Rep Obstet Gynecol 2012;2012:308476.
[9]Kanagal DV,Hanumanalu LC.Ruptured rudimentary horn pregnancy at25 weeks with previous vaginal delivery:a case report.Case Rep Obstet Gynecol 2012;2012: 985076.
[10]Singh N,Singh U,Verma ML.Ruptured bicornuate uterus mimicking ectopic pregnancy:A case report.J Obstet Gynaecol Res 2013;39(1):364-366.
?Corresponding author:Guiping Wan,MD,Laboratory of Gynecological Oncology,Jiangsu Province Hospital on Integration of Chinese and Western Medicine Affiliated with Nanjing University of Traditional Chinese Medicine,100 Hongshan Road,Nanjing,Jiangsu 210029,China.Tel/fax:+86-25-85608658/+86-25-85637817,E-mail:wgplab@163.com. Received 04 July 2013,Revised 15 August2013,Accepted 04 December 2013,Epub 28 February 2014
The authors reported no conflict of interests.
?2015 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.29.20130089
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年1期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年1期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Ventricular tachycardia ablation and substrate modification in ICD patients with electrical storm
- Induced pluripotentstem cells are induced pluripotentstem cell-like cells
- HLA antigens and anti-sperm antibody production in Iranian vasectomized men
- Surgicaloutcomes ofmini-open Wiltse approach and conventional open approach in patients with single-segment thoracolumbar fractures withoutneurologic injury
- Portalvein arterialization promotes liver regeneration after extended partialhepatectomy in a rat model
- Prevalence ofenteric pathogen-associated community gastroenteritis among kindergarten children in Gaza