
Squamous Cell Carcinoma of Small Intestine: a Case Report△
2014-04-20 01:37:36YiBaoZhengxiangZhongandYaweiYu
Chinese Medical Sciences Journal 2014年4期
Yi Bao, Zheng-xiang Zhong, and Ya-wei Yu
1Department of Oncology, 2Department of Surgery, 3Department of Pathology, The Second Hospital of Jiaxing, Jiaxing 314000, China
NEOPLASMS derive from small intestine are rare and most cases are adenocarcinomas and carcinoid.1Squamous cell carcinoma of small intestine is even rarer and only few cases reported in literature.1In this article, we report a case of a 68-year-old male who underwent a laparotomy due to perforation of the small intestine and was diagnosed with squamous cell carcinoma of the small intestine.
CASE DESCRIPTION
A 68-year-old male Chinese underwent a laparoscopy with removal of an abdominal mass in January 2013. The histopathological examination suggested that the mass was a grade II squamous cell carcinoma, with the primary site unclarified. No evidence of tumor cells metastasis to local lymph nodes was found. After surgery, the patient did not receive any chemotherapy. In August 2013, the patient took a routine check, in which increased squamous cell carcinoma antigen (56.40 μg/L, normal reference values 0-2 μg/L) and cytokeratin (15.39 μg/L, normal reference values 0-5 μg/L) were observed. He was given 4 cycles of Tegafur Gimeracil Oteracil Potassium Capsule (S1) 60 mg twice a day from day 1 to 14, combined with recombinant human endostatin (Endostar) 15 mg from day 1 to 14. During the treatment, the patient complained of occasional abdominal pain but no other discomfort. No positive signs were detected in abdominal physical examination. No evidence of other new tumor lesions was revealed by routine CT scans. On November 5, 2013, the patient suddenly felt a persistent abdominal pain, accompanied by nausea, vomiting, and diarrhea. Physical examination showed his temperature at 37.7°C, blood pressure dropped to 70/42 mmHg, increased abdominal muscle tension and a slight rebound pain at the hypogastria region. An emergent abdominal CT scan suggested increased edema of the small intestine at the hypogastria region but without subdia- phragmatic free-air (Fig. 1A) compared with a CT image obtained 5 days earlier (Fig. 1B). Purulent ascites was observed with diagnostic abdominal puncture. The patient was diagnosed with acute peritonitis and an emergency laparotomy was performed. A hard lump about 4 cm × 5 cm with partial perforation of the tumor was observed at the small intestine (ileum) approximately 100 cm proximal to the ileocecus, and no metastatic nodules were found in the intra-peritoneal cavity, liver, pancreas, and celiac artery and mesenteric root. Histopathological examination of the removed tumor showed “a poorly differentiated squamous cell carcinoma” at the small intestine, with size measured 4 cm× 5cm. Tumor cells were present at all layers of the small intestine and infiltrated the mucosa, submucosa, muscle, serosa, and mesentery (Fig. 2). Mesenteric lymph nodes were negative of tumor cells (0/8), and no evidence of tumor cells was found at both edges of resection. Immunohistochemical test showed tumor protein p63 (+), cytokeratin (CK)5/6 (+), caudal-related homeobox 2 (CDX2) (-), CK20 (-), chromogranin A (CgA) (-), synaptophysin (SYN) (-), thyroid transcription factor-1 (TTF1) (-). Postoperative diagnosis was squamous cell carcinoma of the small intestine with acute perforation.
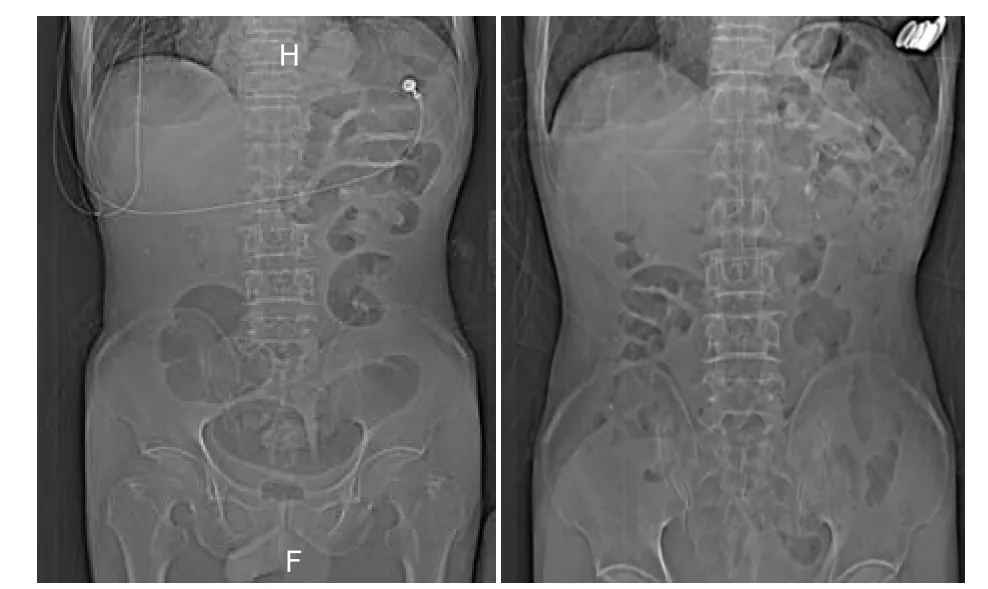
Figure 1. The CT image of a 68-year-old male patient shows increased edema of the small intestine at the hypogastria region (A) compared with a CT image obtained 5 days earlier (B).
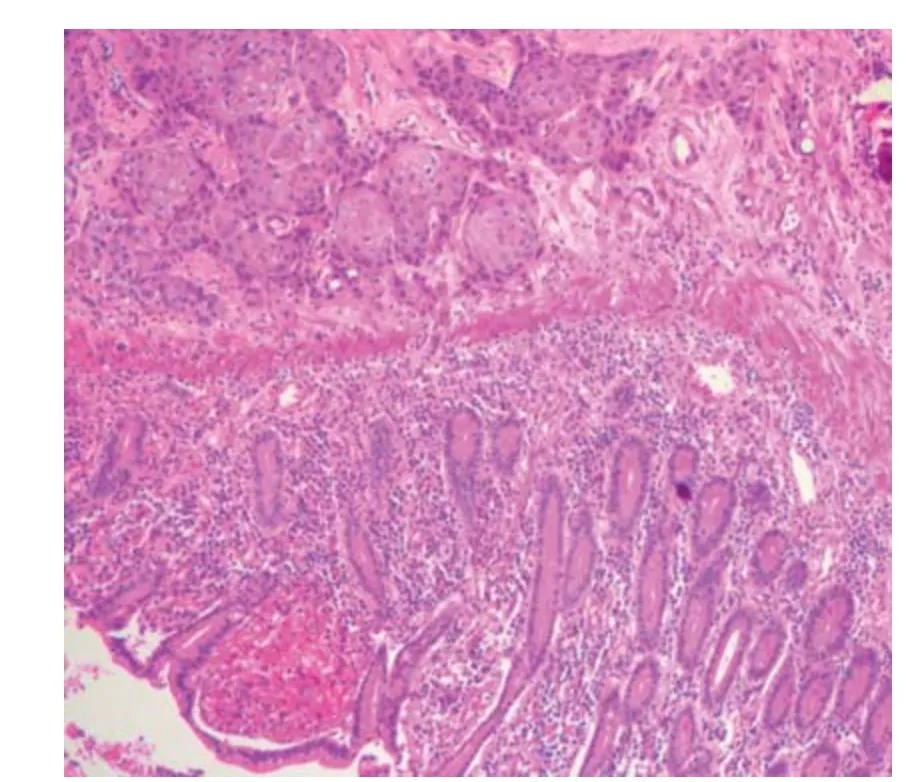
Figure 2. Histopathological examination of the resected lump at the small intestine shows the presence of squamous tumor cells in mucosa, submucosa, muscle, serosa and mesentery. (HE×200)
DISCUSSION
Both primary and metastatic squamous cell carcinoma is a very rare malignancy.2In literature, abdominal pain and acute peritonitis are common symptoms; however, squamous cell carcinoma of the small intestine usually has no specific clinical symptoms and signs. It is often diagnosed after laparotomy as a result of concurrent obstruction or perforation. The etiology of primary small intestine squamous cell carcinoma may be congenital defects of the small intestine, such as intestinal duplication and Meckel’s diverticulum.3The primary neoplastic lesions with metastasis to the small intestine have been reported in the lung, breast, ovary, melanoma, liver and tongue.4-7Histologically, well differentiated squamous cell carcinoma has a high proportion of large, differentiated, keratinocyte- like squamous cells and a low proportion of small basal- type cells.8Basal-type cells presents predominantly in poorly differentiated squamous cell carcinoma.8
In this case report, the patient initially received an abdominal tumor mass resection (grade II squamous cell carcinoma) and the origin of the tumor was unclear. Seven months later, a squamous cell carcinoma of the small intestine with acute perforation was diagnosed. Based on the previous reports, if the majority of cancer cells are deep in the wall of the small intestine, only a few at mucosa, the small intestine tumors may be metaplasia.7The criteria for metastatic tumors of the small intestine are: a clearly primary lesion; the presence of symptoms such as obstruction, perforation and bleeding; positive histopath- ological findings after laparotomy; no signs of a direct invasion by the original tumors from intraperitoneal cavity. The gross observation during laparotomy found that a tumor lesion located at the small intestine, partial perforation. The primary lesion of the abdominal mass of this case has not been clarified, and in analysis of the intestinal resection specimen, the serosal surface was smooth. This observation helps us rule out the adjacent tumor invasion. We consider that in this case, squamous cell carcinoma of the small intestine is most likely to be the primary lesion.
1. Mumtaz S, Ahmad Z, Fatima S, et al. Squamous cell carcinoma in the small intestine. BMJ Case Rep 2011 [cited 2014 Mar 1]. Available from: http://casereports. bmj.com/content/2011/bcr.01.2011.3762.full.
2. Terada T. Malignant tumors of the small intestine: a histopathologic study of 41 cases among 1,312 consecutive specimens of small intestine. Int J Clin Exp Pathol 2012; 5:203-9.
3. Terada T. Primary pure squamous cell carcinoma of the duodenum: a case report. Gastroenterol Res 2010; 3:39-40
4. Yamada H, Akahane T, Horiuchi A, et al. A case of lung squamous cell carcinoma with metastases to the duodenum and small intestine. Int Surg 2011; 96:176-81.
5. Aoyagi Y, Matsuda K, Shimada R, et al. Perforation of the small bowel due to metastasis from tongue cancer. Int Surg 2011; 96:90-3.
6. Azevedo CR, Cezana L, Moraes ES, et al. Synchronous thyroid and colon metastases from epidermoid carcinoma of the lung: case report. Sao Paulo Med J 2010; 128:371-4.
7. Thomas RM, Sobin LH. Gastrointestinal cancer. Cancer 1995; 75:154-70.
8. Cockerell CJ. Histopathology of incipient intraepidermal squamous cell carcinoma (“actinic keratosis”). J Am Acad Dermatol 2000; 42:11-7.
 Chinese Medical Sciences Journal2014年4期
Chinese Medical Sciences Journal2014年4期
- Chinese Medical Sciences Journal的其它文章
- Inhibition of Xanthine Oxidase Activity by Gnaphalium Affine Extract
- Evaluation of Risk Factors for Arytenoid Dislocation after Endotracheal Intubation: a Retrospective Case-control Study
- Non-enhanced Low-tube-voltage High-pitch Dual-source Computed Tomography with Sinogram Affirmed Iterative Reconstruction Algorithm of the Abdomen and Pelvis
- Primary Combined Intra-articular and Extra-articular Synovial Osteochondromatosis of Shoulder: a Case Report
- BRAF V600E Mutation as a Predictive Factor of Anti-EGFR Monoclonal Antibodies Therapeutic Effects in Metastatic Colorectal Cancer: a Meta-analysis
- Multiple Myeloma Mimicking Spondyloarthritis: a Case Report